
Abstract
Background:
Most people diagnosed with a psychotic disorder will be prescribed psychotropic medication. The second Australian national survey of psychosis provided a unique opportunity to examine the pharmacological treatment of psychotic disorders from the perspective of the consumer. The aim of this paper is to report on medication use, adherence and perceived efficacy, and to describe side effect profiles.
Method:
Data on self-reported medication use in the 4 weeks prior to interview, including type, duration, adherence, side effects and helpfulness was collected from participants interviewed in the course of the second Australian national survey of psychosis.
Results:
The majority (91.6%) of participants were using psychotropic medication: 89.0% of people aged 18–34 years and 93.5% of people aged 35–64 years. The most commonly used class of medication was antipsychotic medication (81.6%). In addition, 37.4% were using antidepressants, 26.7% were using mood stabilisers and 17.8% were using anxiolytics/hypnotics. Polypharmacy was common with almost two-thirds (63.4%) using more than one class of medication and over a quarter (28.1%) of people with schizophrenia using more than one antipsychotic. Many participants (84.4%) reported experiencing side effects. The side effect profile of people using atypical antipsychotics was on average better than that of people using typical antipsychotics. Most people (85.2%) felt their medication relieved their mental health symptoms and most (88.2%) medication was taken as prescribed.
Conclusions:
Many people with a psychotic disorder are receiving antipsychotics, with a substantial proportion also taking antidepressants, mood stabilisers and anxiolytics/hypnotics. Medication use differs by age group, diagnostic group and course of illness. Many people using antipsychotics describe significant impairment in their everyday life as a result of medication side effects. Users of typical antipsychotics reported more side effects and more impairment than people using atypical antipsychotics. Most of our participants were prescribed psychotropic medications, and most reported that they were taking them.
Background
Most people diagnosed with a psychotic disorder will be prescribed psychotropic medication. The number of new medications available to treat the symptoms of psychosis and associated depression and anxiety has grown over the last 20 years. The new atypical antipsychotics with reportedly improved side effect profiles play an important role in the treatment and management of schizophrenia and other psychotic disorders (Keks, 2004; Ucok and Gaebel, 2008). The use of two or more antipsychotics has become increasingly common (McCue et al., 2003), despite the increased likelihood of side effects and the lack of evidence to support this practice (Miller and Craig, 2002; Barnes and Paton, 2011). People with psychotic disorders are known to have high rates of cardiometabolic risk factors, cardiovascular disease and diabetes (Galletly et al., 2012; McEvoy et al., 2005) and evidence emerging suggests that antipsychotics may be a contributing factor (Brunero et al., 2009). The second Australian national survey of psychosis provided a unique opportunity to examine recent trends in the use of pharmacological agents in the management of psychotic disorders and to explore adherence, side effects and treatment efficacy from the participant’s perspective.
Methods
Participants were drawn from the second Australian national survey of psychosis. The full details of the methodology are described elsewhere in this volume (Morgan et al., 2012). In summary, the survey was conducted within seven catchment sites across five Australian states, covering an area of around 62,000 square kilometres and a population of some 1.5 million people aged 18–64 years, approximately 10% of the Australian population in this age group. A two-phase design was used. In Phase 1, screening for psychosis took place in public specialised mental health services and in non-government organisations supporting people with a mental illness in the census month (March 2010). A psychosis screener developed for the first national psychosis survey was used to identify individuals likely to meet criteria for formal diagnosis (Jablensky et al., 2000). Administrative records were scanned to identify people with a recorded diagnosis of psychosis and in contact with public specialised mental health services in the 11 months prior to census but not in the census month. In Phase 2, people who were screen positive for psychosis in Phase 1 were randomly selected, stratified by age group (younger people, 18–34 years, and older people, 35–64 years), for interview and assessment. Age stratification was used to ensure good coverage of younger as well as older age groups. Of 7955 people who were screen positive for psychosis and eligible, 4189 people were contacted and 1825 consented to interview. Data were assessed and rated by the interviewers who had professional mental health backgrounds and who based their judgements on participant responses throughout the course of the interview. Data collected included: symptomatology, substance use, cognitive ability, functioning, disability, physical health, health service utilisation, education, employment and housing. Course of illness was assessed and rated based on the semi-structured diagnostic interview. It refers to the number of episodes of mental illness that a person had experienced and the degree of recovery after each episode.
Assessments
Participants were asked to bring to the interview all medication they were taking or a list of these medications. Medication charts were referred to for those participants who were currently in hospital. Questions relating specifically to medication use for at least the previous 4 weeks were included in the interview, and all data gathered were based on self-report. For each medication, participants were asked about duration, frequency and quantity of use, efficacy and, if not taken as recommended, the main reason why. We have presented aggregated comparisons between ‘atypical’ and ‘typical’ antipsychotics. This follows what has become conventional terminology, but a simple dichotomy between classes does not convey the fact that medications within each of these groupings are heterogeneous in terms of efficacy and tolerability. Our survey was not powered to report individual medication data. Adherence was defined as taking medication as prescribed, missing only the occasional dose, while non-adherence was defined as taking more or fewer doses than prescribed or taking them more or less frequently than advised. Participants were shown a list of 26 specific side effects and asked to indicate whether they had experienced any in the previous 4 weeks, which they attributed to their current medication.
Statistical analysis
Univariate logistic regression (SPSS v19) was used to examine the impact of age and course of illness on psychotropic medication use.
Results
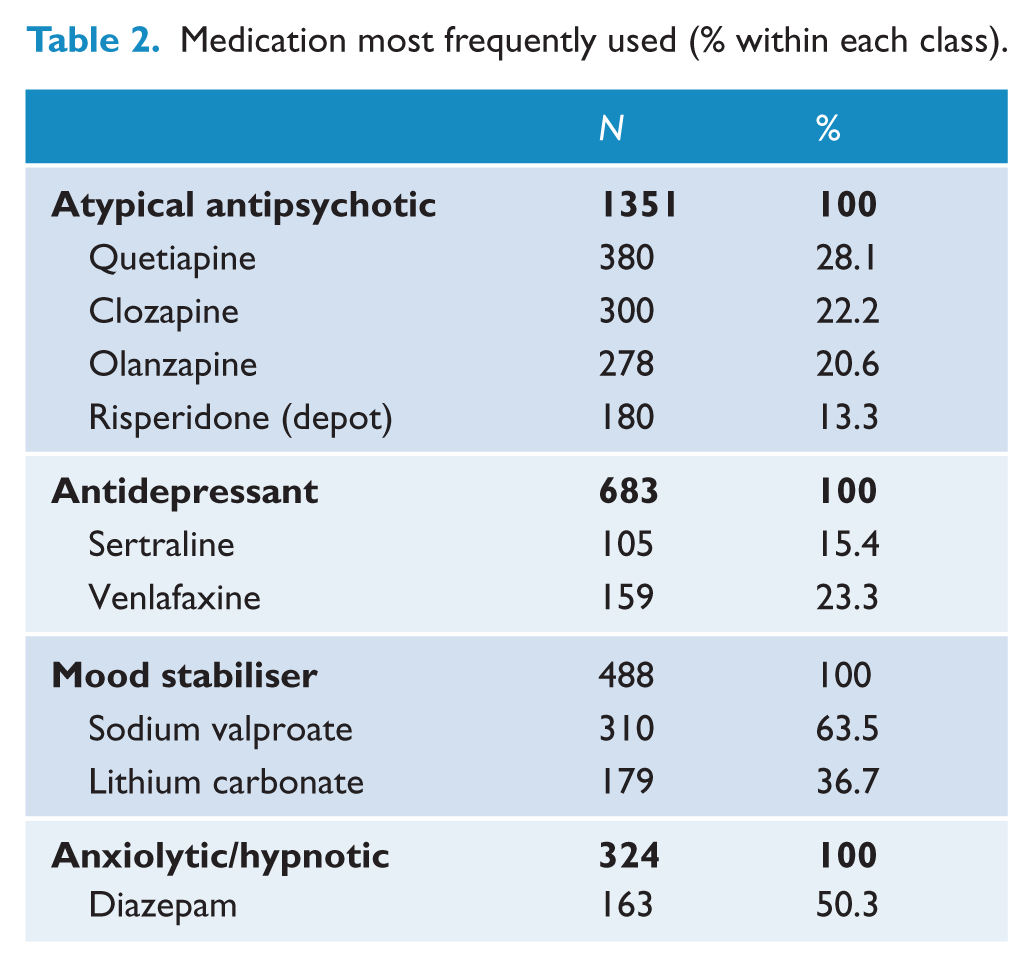
Almost all (91.6%) participants indicated they were using psychotropic medication (typical antipsychotics, atypical antipsychotics (AAP), antidepressants, mood stabilisers, anxiolytic/hypnotics or nicotine/opioid/alcohol dependence medication). Antipsychotic agents were the most commonly prescribed, being reported by 81.6% of all participants (Table 1). AAP formed the bulk of the antipsychotics prescribed (74.0% compared to 15.2% for typical agents). Oral formulations were more commonly used than the long-acting intramuscular (depot) medications (66.4% compared to 12.1%). Older people were significantly more likely to be using a typical antipsychotic than younger people (OR 1.4; 95% CI: 1.1 to 1.9). Quetiapine and clozapine were the most frequently used antipsychotics (28.1% and 22.2% of people taking antipsychotics were using these specific antipsychotics, respectively) (Table 2). In addition to antipsychotic medications, 37.4% of all participants were using antidepressants, 26.7% mood stabilisers and 17.8% anxiolytics/hypnotics. Older people were also significantly more likely than younger participants to be using all classes of medication other than AAP (antidepressants OR 1.5, 95% CI: 1.3 to 1.9; mood stabilisers OR 1.5, 95% CI: 1.2 to 1.9; anxiolytics/hypnotics OR 1.4, 95% CI: 1.1 to 1.8).
Psychotropic medication use by age group a (% of all participants).
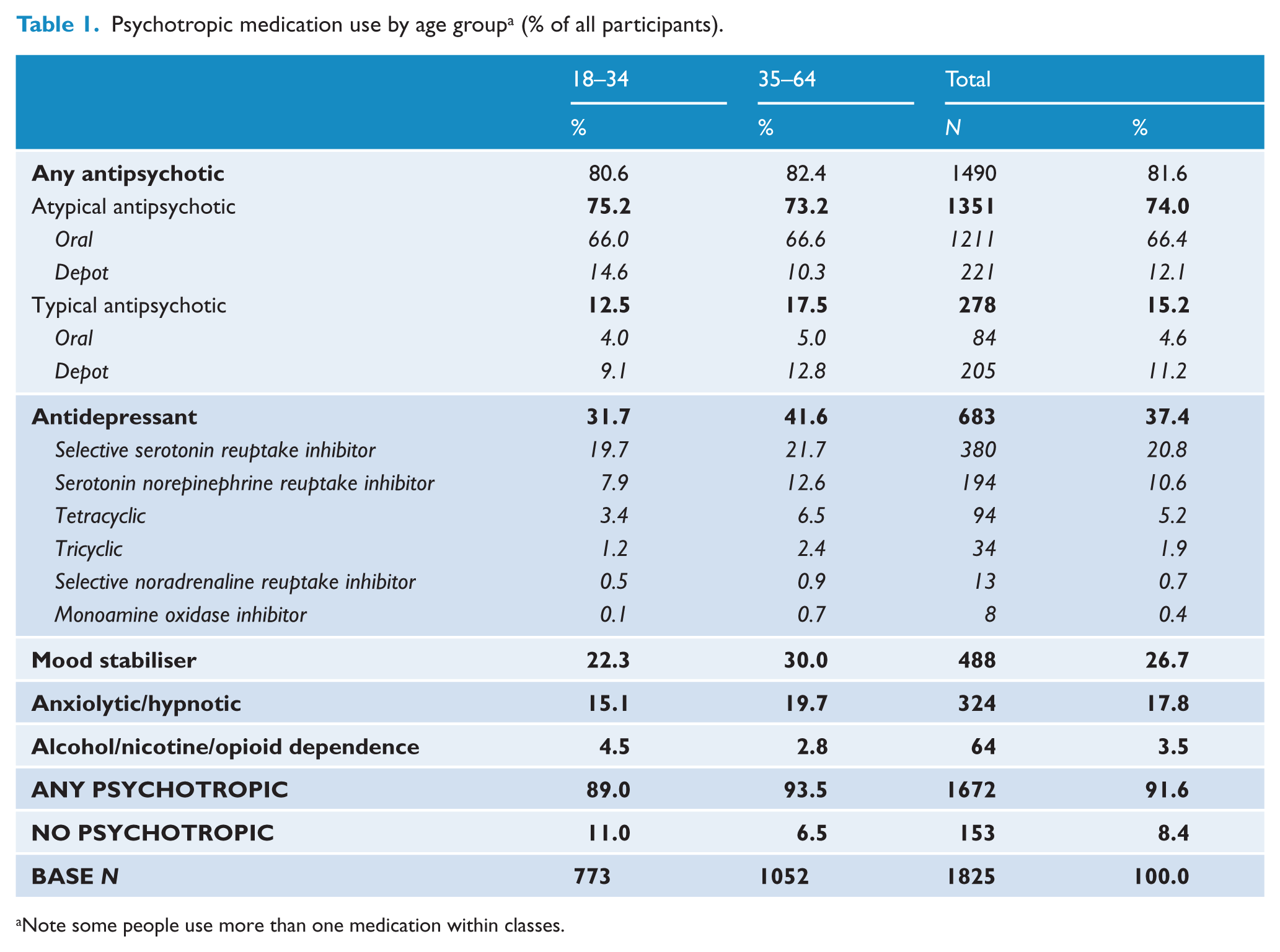
Note some people use more than one medication within classes.
Medication most frequently used (% within each class).
Diagnosis
Medication use varied greatly by diagnosis (Table 3). Antipsychotic agents were the most commonly used medication by people in all diagnostic categories except the depressive psychosis group. Anxiolytics/hypnotics were also used across all diagnostic categories, but the proportion using these medications was smaller and more stable across the diagnostic groups. Antipsychotics were most commonly used by people with an ICD-10 diagnosis of schizophrenia (92.1%), with the majority (83.7%) using an AAP. A small proportion (5.3%) of people with schizophrenia had received no psychotropic medication in the previous 4 weeks. The majority (88.7%) of people with schizoaffective disorder were using an antipsychotic, and approximately one-third was using an antidepressant or mood stabiliser (38.9% and 32.4%, respectively). Mood stabilisers were most frequently used by people with a diagnosis of bipolar affective disorder and antidepressants by people with a depressive psychosis.
Psychotropic medication use by diagnosis. a
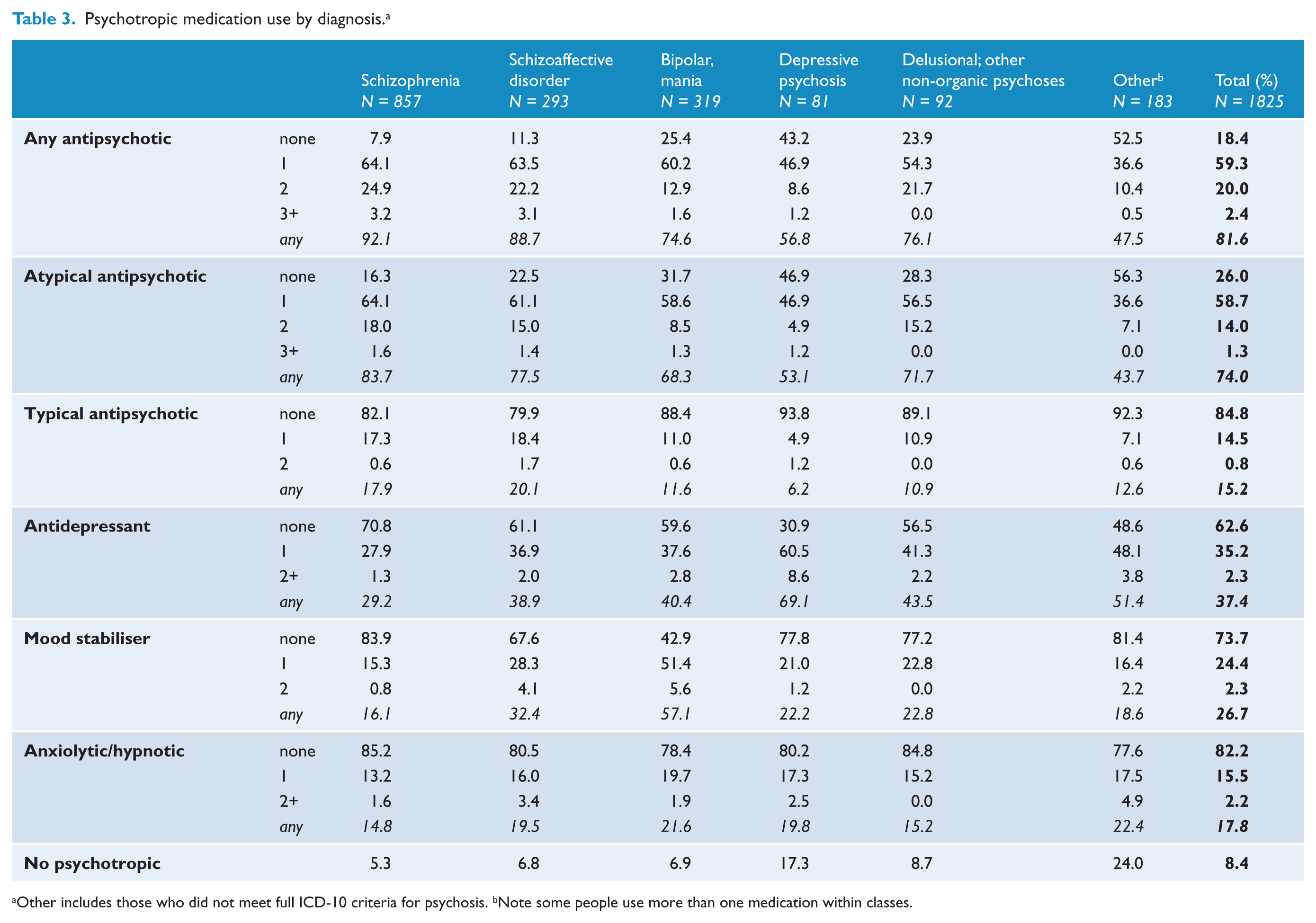
Other includes those who did not meet full ICD-10 criteria for psychosis.
Note some people use more than one medication within classes.
Course of illness
Course of illness refers to the number of episodes of mental illness a person experiences and the degree of recovery after each episode. At the time of interview, 8.1% had experienced just a single episode of illness; 61.5% had had multiples episodes with good or partial recovery of symptoms between episodes (29.7% and 31.8%, respectively); 20.6% had a continuous chronic illness with persistent symptoms; and 9.9% had a chronic illness with ongoing deterioration in their symptoms. No matter what the course of illness, the proportion of participants using any psychotropic medication was similar, with the exception of people who had experienced a single episode of illness where 25.2% were not using any medication (Table 4). The proportion of people using psychotropic medication increased as the course of illness deteriorated, as did the use of multiple antipsychotics. For all classes of medication, when compared to people with a single episode of illness, people in all other categories of course of illness were significantly more likely to be using psychotropic medication with the exception of antidepressants. In the case of antidepressants, people with multiple episodes of illness with partial recovery and those with a chronic illness were more likely to be using an antidepressant (OR 1.9, 95% CI: 1.3 to 2.9 and OR 1.7, 95% CI: 1.1 to 2.6, respectively), while people with multiple episodes of illness with good recovery and those with a chronic illness with deterioration were not (OR 1.3, 95% CI: 0.8 to 1.9 and OR 1.5, 95% CI: 0.9 to 2.3, respectively). (Full data output is available from the authors on request).
Psychotropic medication use by course of illness.
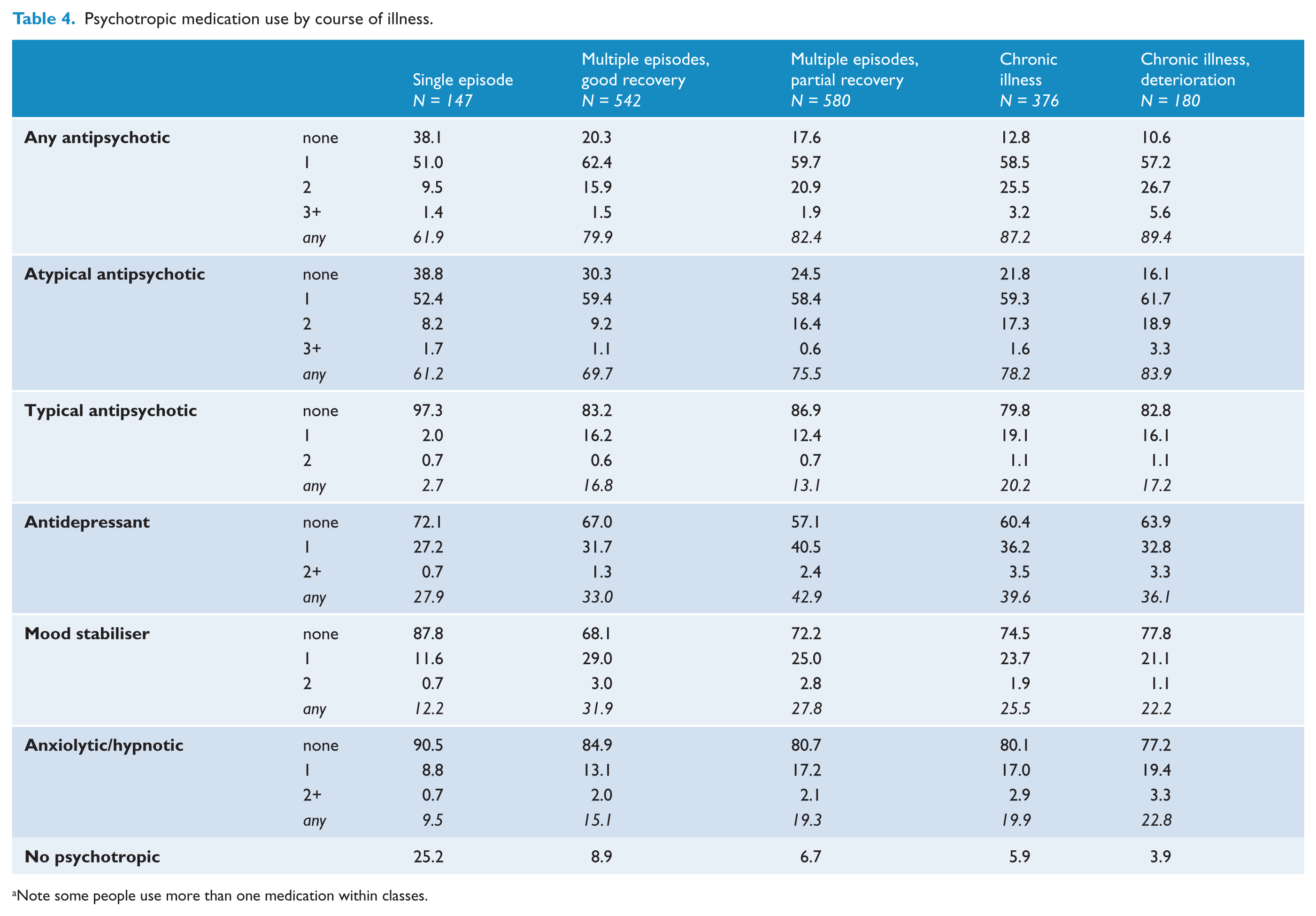
Note some people use more than one medication within classes.
Polypharmacy
Overall, 69.0% of people on psychotropic medication had been using more than one medication in the month prior to interview, some as many as eight (Table 5). Almost two-thirds (63.4%) were using more than one class of medication, 41.2% were using two classes and 22.2% three or more. The majority (47.4%) of people using two or more classes of medication were using psychotropic medication in combination with an AAP: 8.3% were on both an AAP and a typical antipsychotic. Older rather than younger people were more likely to be using more than one class of medication (67.1% compared to 58.1%), with a quarter (25.0%) of older people using three or more classes of medication.
Number of classes of psychotropic medication used (% of participants using any medication).
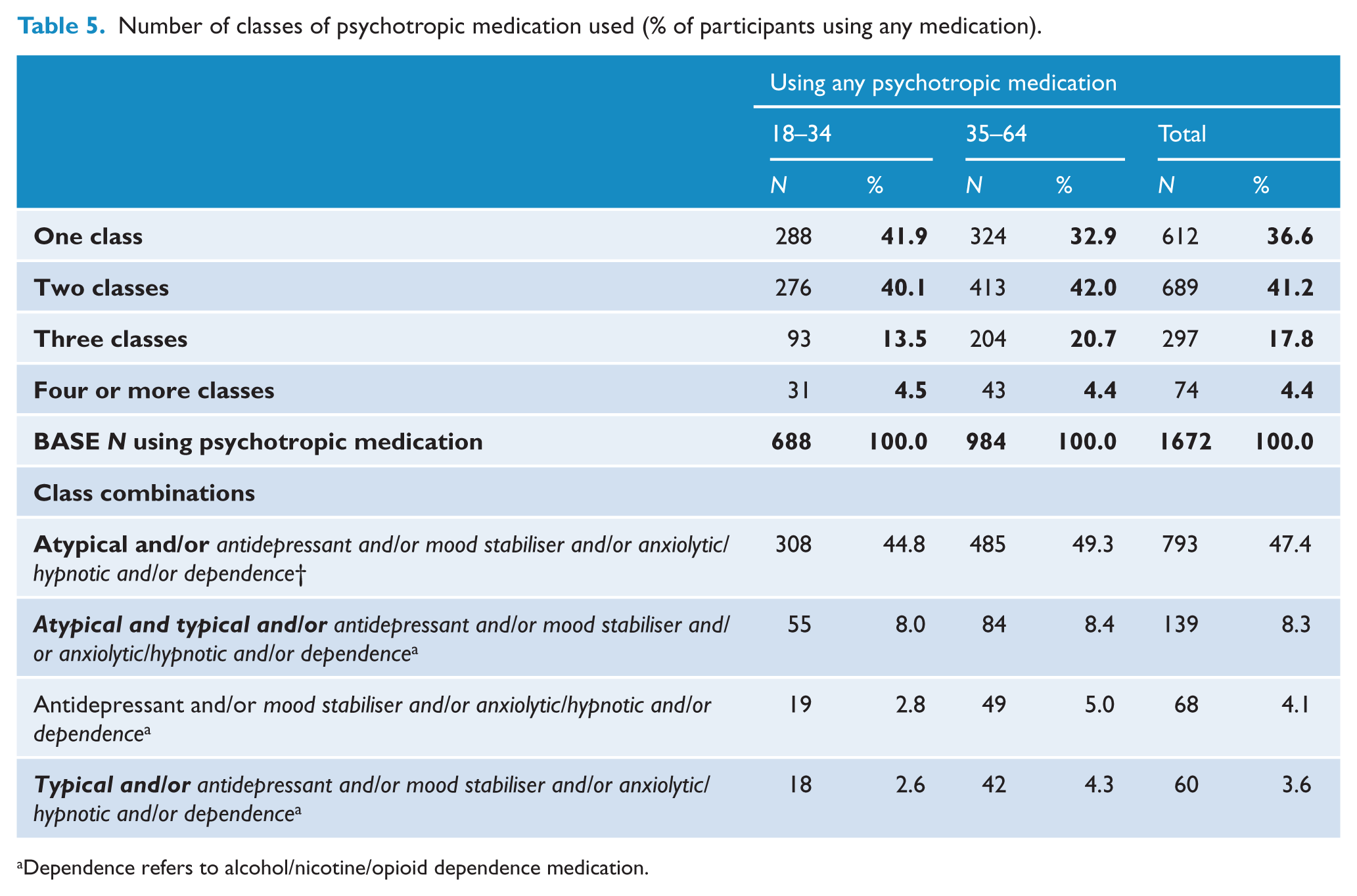
Dependence refers to alcohol/nicotine/opioid dependence medication.
While the use of many classes of medication was common, the use of multiple medications within a class was not. Most people were using only one medication within a class, with the exception of antipsychotics where a quarter (24.9%) of people with schizophrenia were using two antipsychotics and a small percentage (3.2%) were using three or more. Use of multiple antipsychotics was most common in people with a chronic illness with deterioration. The majority (89.4%) of people with a chronic course of disorder with deterioration were using antipsychotic medication, and one-third (32.3%) were using two or more antipsychotics compared to 10.9% of people with a single episode of illness.
Side effects
Analysis of side effects was restricted to participants using only one class of medication in order to be able to compare side effect profiles more accurately (Table 6). Drowsiness, dry or more watery mouth, limbs trembling or shaking and weight gain were the most commonly reported side effects across all classes of medication. Almost half the people using AAP experienced sedation and anticholinergic side effects (49.4% and 47.7%, respectively), and a third reported extrapyramidal side effects (EPSE), akathisia, weight gain and ‘other’ side effects (34.1%, 30.3%, 36.8%, 37.0%, respectively). Female users of AAP (12.3%) most frequently noted period changes or menstrual pain. A comparison of typical and atypical side effect profiles showed that people using typical antipsychotics were more likely to report any side effects (86.1% compared to 80.7%, respectively), and the proportion reporting 10 or more side effects was almost double for typical users (17.7% compared to 9.8%). Users of typical antipsychotics were also twice as likely to experience tardive dyskinesia (15.2% compared to 6.0%), and one and a half times more likely to report akathisia (43.0% compared to 30.3%), and EPSE (51.9% compared to 34.1%) than users of AAP. A slightly greater proportion of people using AAP than typical antipsychotics reported gaining weight over the previous 6 months (36.8% compared to 30.4%), but their median weight gain was slightly less (6 kg compared to 7 kg). The majority of people (69.7%) using antipsychotics describe impairment in their everyday life as a result of medication side effects: 33.9% reported moderate or severe impairment.
Self reported side effect by class of medication.
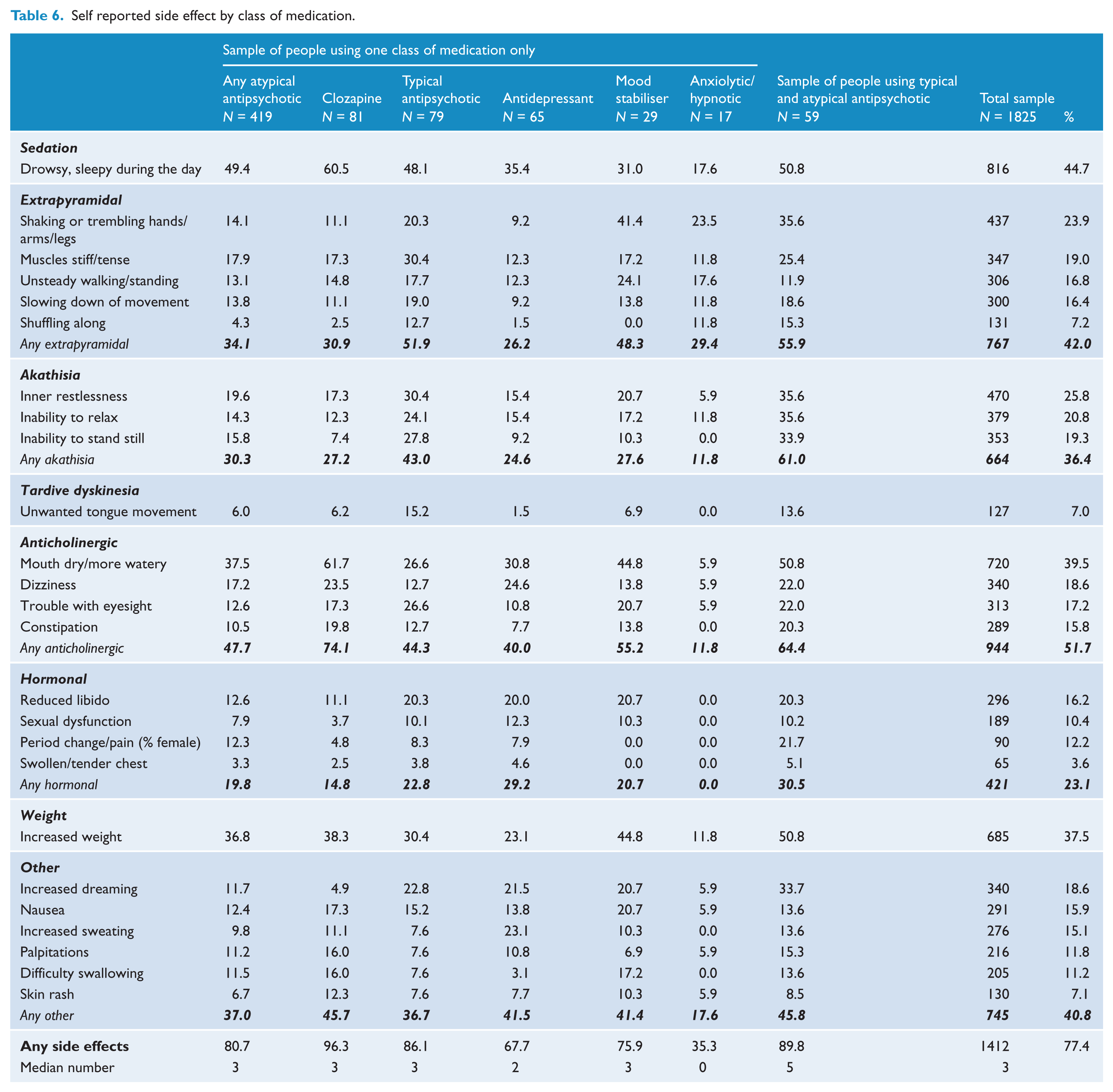
While the proportion of people using only an antidepressant, mood stabiliser or anxiolytic/hypnotic was small, those using only antidepressants were more likely than users of other classes of medication to experience hormonal side effects and more than half (55.2%) of the people using a mood stabiliser reported anticholinergic side effects. Two-thirds (64.7%) of people using an anxiolytic/hypnotic, a third (32.3%) using an antidepressant and a quarter (24.1%) using a mood stabiliser reported not having experienced any side effects in the 4 weeks prior to interview.
Because polypharmacy was so common, side effects were also examined in people using a combination of a typical and atypical antipsychotic only (N = 59). The majority (89.8%) of people exposed to antipsychotic polypharmacy experienced side effects, and were more likely than people using only a typical or atypical antipsychotic to experience any categories of side effect except tardive dyskinesia. The proportion reporting akathisia was doubled in this group compared to those using only an AAP (61.0% compared to 30.3%).
Satisfaction with medication
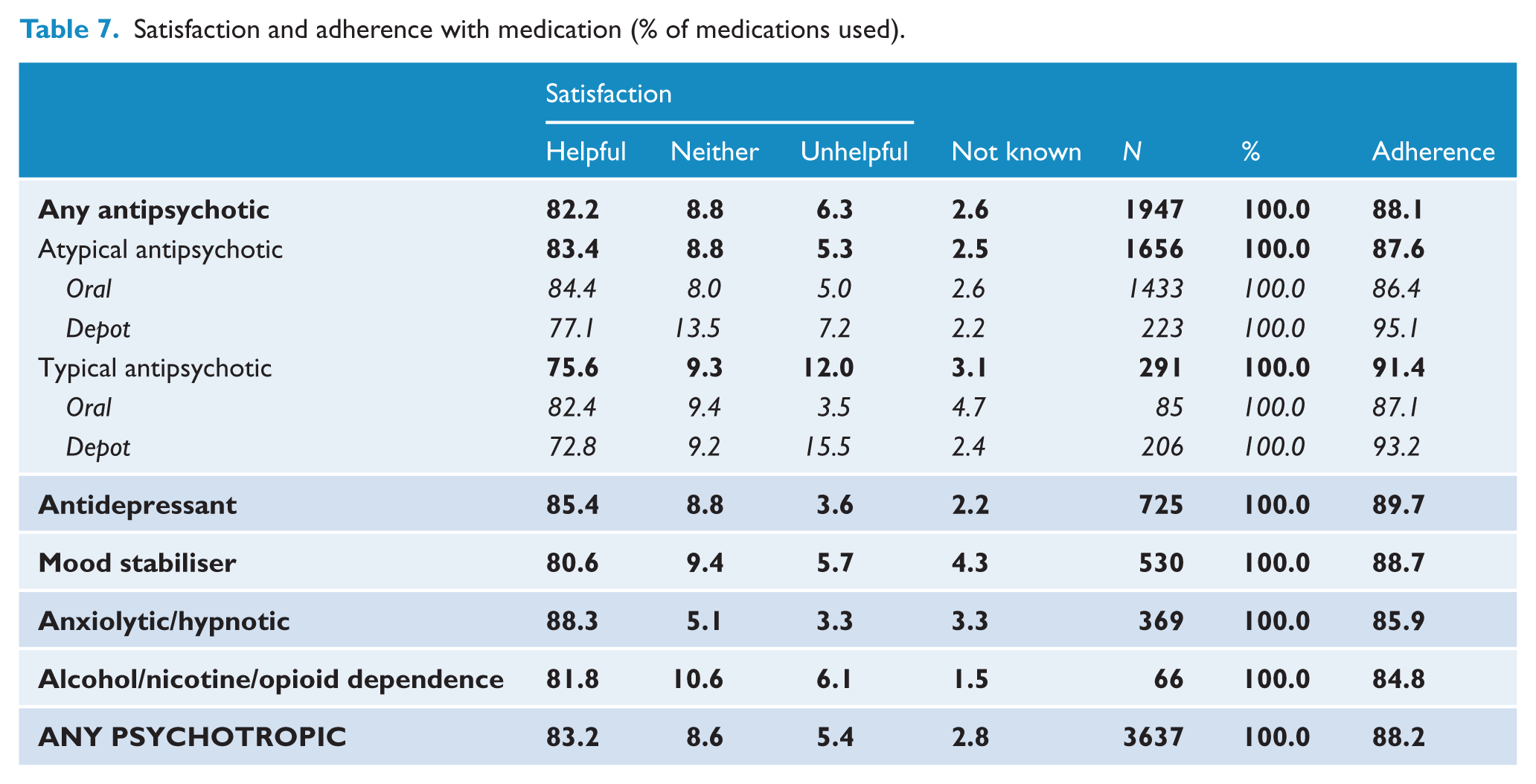
Participants rated the overall helpfulness of each of their medications (Table 7). The majority (83.2%) of the 3637 recorded prescribed psychotropic medications were considered to be somewhat or very helpful, with anxiolytics/hypnotics considered the most helpful (88.3%). Atypicals were considered more helpful than typical antipsychotic medication (83.4% compared to 75.6%), and oral antipsychotics were endorsed as more helpful than depot antipsychotics (84.3% compared to 75.1%). Most people (85.2%) indicated that their medication relieved their mental health symptoms; for 57.1%, they eased their symptoms ‘a lot’. People who indicated that medication did not ease their symptoms were more likely to experience 10 or more side effects (22.6% compared to 14.6%). Confidence that taking medication was good for them was high: 70.5% reported being very or somewhat confident in their medication, 13.6% neither confident nor unconfident and only 11.6% unconfident. A quarter (27.2%) of all participants identified medications for their mental health as the form of care that had helped them most in the previous 12 months.
Satisfaction and adherence with medication (% of medications used).
Adherence
Overall reported medication adherence was high: 88.2% of all psychotropic medication was reportedly being taken as prescribed (Table 7). Adherence with depot antipsychotics was better than for oral agents. Of note, 28.0% of people using depots were on a community treatment order compared to 11.6% of people using oral agents. A total of 253 participants reported that in the previous 4 weeks they had not taken one or more medications for their mental health as recommended. The characteristics of people who indicated they took medication as prescribed were compared to those who did not. There was very little difference in age, sex, educational level, type of medication used, or the number or type of side effects experienced in the two groups. A marginally higher proportion of people who were not adherent were taking more than one medication for their mental health (32.0% compared to 25.3%); lacked insight into their illness and need for treatment (26.5% compared to 22.3%); experienced negative symptoms (81.0% compared to 70.0%); or had a chronic course of illness with or without deterioration (37.1% compared to 30.5%). Participants who were not adherent were more likely to have a lifetime diagnosis of alcohol abuse and/or dependence (63.2% compared to 47.6%); to be moderately or severely impaired in their everyday life by medication side effects (41.1% compared to 30.8%); to feel their medication did not ease their mental health symptoms (16.2% compared to 8.3%); and be less likely to say they were confident that their medication was a good thing for them (56.9% compared to 73.0%). The most common reason given for not taking medication was that it was forgotten (28.6%). Older people were more likely than younger people to say they were unable to afford the medication (7.3% compared to 1.6%) or to report taking more medication than prescribed (12.7% compared to 6.3%). Other than forgetting, the most common reason given by younger people was the side effects they experienced (14.3%) and feeling that medication was not helping them (10.1%). Less than half (46.7%) the people using medication indicated that a clinician had discussed with them the benefits and disadvantages of their medications, and only 5.1% had been involved in medication management groups in the previous 12 months.
Clozapine
A total of 300 people (16.4% of the total sample, 22.2% of those using an AAP) were using clozapine: 72% were males and 58.3% were aged 35–64 years. The majority (71.7%) had a diagnosis of schizophrenia, 14.0% had a diagnosis of schizoaffective disorder and 5.7% bipolar affective disorder. A quarter (27.0%) of people using clozapine were using no other medication; a similar proportion (25.3%) was also on an AAP, with 5.3% were using it with both a typical and another AAP. The largest proportion (42.3%) was using it in combination with an antidepressant, mood stabiliser and/or anxiolytic/hypnotic. Most people (96.3%) taking clozapine reported side effects, with almost a third (30.9%) experiencing six or more side effects in the previous 4 weeks. The most commonly reported side effects were drowsiness (60.5%) and having a mouth dry or more watery than usual (61.7%); 74.1% noting anticholinergic side effects. The majority of clozapine users (92.3%) reported they were adherent with their medication, 87% said it was helpful for their mental health and 63% said it eased their mental health symptoms ‘a lot’.
Discussion
In this survey, the majority of people living with psychosis were prescribed psychotropic medication. Antipsychotic agents were the most frequently prescribed medications, most frequently prescribed to people with a diagnosis of schizophrenia. As well as antipsychotics, many participants were also using antidepressants, mood stabilisers and anxiolytics/hypnotics. Although AAP were the most commonly used antipsychotics, 15.2% of people were using a typical agent. Clozapine was more likely to be used by older males, but its use was not limited to people with schizophrenia, and it was frequently used in combination with other medication. Our finding of high rates of adherence with clozapine is similar to other studies (Gilmer et al., 2004) and may reflect the close medical monitoring associated with this agent. Younger people with a single episode of illness were almost three times more likely than older people with a similar course of disorder to be using a depot antipsychotic.
Polypharmacy was common. Possible rationales for combining antipsychotics include: ‘to target a particular symptom domain’, ‘to avoid high dosages of a single antipsychotic’ and ‘in an attempt to counteract adverse effects of the first antipsychotic’ (Barnes and Paton, 2011). Whatever the reasons, two-thirds of people were subject to polypharmacy, with one-quarter using a combination of more than one antipsychotic. Irrespective of the rationale, combining atypical and typical psychotics magnified the risk of experiencing side effects in almost all categories.
With so many people using more than one class of medication, inevitably it is difficult to determine which medication is responsible for which side effect, so side effect profiles were examined for single classes of medication. Atypical antipsychotics appear to be associated with a lower side effect burden than typical agents. Nonetheless, a third (34.1%) of participants on AAP still reported EPSE. Dosages may play a role, but this information was not ascertained.
Given the number and type of side effects reported by so many people, it was surprising to find such good reported adherence across all classes of medication. Adherence can be difficult to assess accurately. Methods frequently used include reviewing prescription and medical records, drug assays of blood, the use of electronic monitoring devices or pill counting. Adherence in this survey was based on self-reported use. In contrast to other studies (Gilmer et al., 2004) we found non-adherence, at least as reported by participants, to be uncommon, but we found familiar associations with non-adherence including lack of insight, negative symptoms and substance abuse. It could be that rates of adherence were inflated due to participants’ desire to tell interviewers what they thought the interviewer wanted to hear. To minimise this risk, no interview was undertaken by a researcher with whom the participant had had a previous professional relationship.
Not surprisingly, people who felt less positive about their medication and were more impaired by side effects were less likely to take their medication as prescribed. The reportedly more benign side effect profile of AAPs was not associated with better rates of adherence. People with chronic illness, a group at greater risk of non-adherence, are more likely to be prescribed depots, sometimes enforced by a treatment order, but 12.1% of younger people with only a single episode of illness were also using a depot. The use of long-acting intramuscular antipsychotics is one strategy to enhance adherence, but these agents were seen by participants as less helpful than oral agents, suggesting that further work is needed to determine the optimal use of these agents in clinical practice.
Although many people experienced numerous debilitating side effects, the most common reason cited for non-adherence was forgetfulness. Non-adherence may result in relapse of psychosis, but improving adherence rates has been found to be a difficult task (Gray et al., 2002), making strategies to counter modifiable non-adherence factors a focus for mental health services.
The analyses in this paper are limited to descriptive and univariate statistics. Further publications on medication use are planned in which multivariate analyses will be undertaken with adjustment for key covariates including age and duration.
What has changed?
Similar information on medication use was collected in the first Australian national psychosis survey in 1997–98 (Castle et al., 2002), enabling a comparison of data to assess change over time. Although the two survey populations differ slightly, the data show overall prescription of psychotropic medication has remained relatively stable (91.6% in 2010 compared to 88.6% in 1997–98). There has been a major shift from typical to atypical antipsychotics. The use of AAP more than doubled from 29.7% to 74.0%, while typical antipsychotic use fell from 54.3% to 15.2% in 2010. This could be seen as a welcome change, as many clinicians consider the atypical agents to have a more benign side effect profile, at least in terms of EPSE, than the typical agents. The data presented here suggest that this was also the experience of participants. The use of clozapine doubled from 8.3% to 16.4% in 2010, as did the use of antidepressants (16.0% to 36.1%). Hopefully the latter reflects clinicians being more aware of the high levels of depression in people with psychosis, and that they are actively addressing this. Finally, the use of more than one psychotropic medication also rose, from 58% in 1997–98, to 69% in 2010. In many ways this is understandable given the complexity of the clinical presentation in many of our participants, with difficult combinations of mood and psychotic symptoms, and often a sub-optimal response to treatment. Indeed, it has been shown that combination therapy with more than one antipsychotic can be helpful for some people, albeit at the cost of more side effects, notably weight gain (Essock et al., 2011).
Conclusion
Most of our participants were prescribed psychotropic medications, and most reported that they were taking them. However, the fact that many were on multiple medications, and that many still experienced psychotic and mood symptoms, underlines the fact that medications are still not fully effective for a substantial minority of people with psychosis. This, along with the high side effect burden associated with these medications, highlights the critical importance of developments in the field of psychopharmacology to develop medications better targeted to individual user profiles.
Footnotes
Acknowledgements
This publication is based on data collected in the framework of the 2010 Australian National Survey of High Impact Psychosis. The members of the Survey of High Impact Psychosis Study Group are: V Morgan (Project Director); A Jablensky (Chief Scientific Advisor); A Waterreus (Project Coordinator); A Mackinnon (Statistician); R Bush, D Castle, M Cohen, C Galletly, C Harvey, P McGorry, J McGrath, H Stain (Site Directors); V Carr (Australian Schizophrenia Research Bank); A Neil (Health Economics); B Hocking (SANE Australia); S Saw (Australian Government Department of Health and Ageing). Ethics approvals for the study were obtained from relevant institutional human research ethics committees.
This report acknowledges, with thanks, the hundreds of mental health professionals who participated in the preparation and conduct of the survey and the many Australians with psychotic disorders who gave their time and whose responses form the basis of this publication.
Funding
The study was funded by the Australian Government Department of Health and Ageing.
Declaration of interest
The authors report no conflicts of interest. The authors alone are responsible for the content and writing of the paper.