
Abstract
Background:
Social inclusion is a key priority of the Fourth National Mental Health Plan for Australia (2009–2014), with strong evidence for its protective impact on mental health. Social integration has been associated with enhanced well-being for people with mental illnesses such as psychosis.
Objective:
To explore the impact of psychosis on an individual’s social and community participation.
Method:
The second Australian national survey of psychosis was conducted across seven Australian sites. Semi-structured interviews with adults living with psychosis assessed mental health status, social and role functioning, life satisfaction and future goals. The cohort comprised 1825 adults with a psychotic illness (59.6% were male; 42.4% were aged 18–34 years; 31.5% had 12 years or more of education) of whom 32.7% had been employed in the past year.
Results:
Most adults indicated experiencing loneliness (80.1%) and a need for more friends (48.1%). Men were more likely to have never had a long-term relationship (59.4% M, 33.2% F). Even though women were more likely to experience anxiety in social situations [(χ2(1) = 8.95, p < 0.01)], they were more likely to have attended a social activity in the past year [χ2(2) = 11.84, p < 0.01]. Just over half of the survey participants (56.7%) reported having daily or nearly daily contact with family members. In the past year, 69% had not attended any social activity and 43% described stigma as a barrier. Although 63.2% showed significant impairment in social functioning, only 29.5% had received help for this in the last year. Social isolation and loneliness were rated as major challenges by 37.2% of the cohort.
Conclusions:
Social isolation and dysfunction experienced by people with psychosis have not decreased since the last Australian national survey of people with psychosis. Alongside education and employment, social functioning and participation must be addressed to improve social inclusion for people with psychosis. Programs targeting social opportunities (befriending, peer support), social anxiety and social functioning for all stages of psychosis are warranted.
Background
Social inclusion refers to the participation of a person in society and is evidenced by an individual having the opportunities, resources and abilities to build and maintain relationships, engage in education and employment, and participate in community events and organisations. A recent review of social exclusion for people with mental health problems recognised the complex, multidimensional and dynamic nature of social exclusion and defined it as ‘enforced lack of participation in key social, cultural and political activities’ (Morgan et al., 2007). This paper focuses on a core component of social exclusion, namely participation in social networks.
The Australian Government’s social inclusion agenda prioritises prevention and early intervention efforts to reduce the major causes of social exclusion, namely, poor educational outcomes, poor health and well-being, and lack of access to, and opportunities for, social supports and networks (Australian Government, 2009a; 2009b). Actions in the Fourth National Mental Health Plan (Australian Government, 2009a) to improve social inclusion focus on education, employment and training with little attention given to social engagement and community participation. Recovery was defined by a consumer with mental illness thus: ‘the aspiration is to live, work and love in a community in which one makes a significant contribution’ (Australian Government, 2009a). Surprisingly, the Plan was launched without comprehensive actions to improve community participation, despite noting the need for further development of an outcome measure of community participation (Australian Government, 2009a). Similarly, a United Kingdom 2011 policy release recognised the role of mental health in overall well-being but did not include reduced social functioning or participation as one of the personal costs of mental health problems (HM Government, 2011).
Historically, the focus on symptom reduction has led to the neglect of the basic human rights of people with psychosis, namely the right to education, to work, to marry, to raise a family and to participate in the community. It is imperative to obtain population-based data on the social inclusion of people with psychosis to evaluate the effectiveness of services and, if necessary, advocate for change.
High rates of comorbidity for social anxiety with schizophrenia, ranging from13 to 36% (Cosoff and Hafner, 1998; Gumley et al., 2004), have driven intervention studies to focus on social anxiety, thereby improving social functioning (Michail and Birchwood, 2009). One study found only weak associations between social anxiety and positive symptoms in schizophrenia, but showed that severity of negative symptoms and the experience of discrimination both predicted concurrent and prospective social anxiety (Lysaker et al., 2010). High rates of perceived discrimination (62% of sample) and self-stigma (42%) were reported by a large European sample of people with schizophrenia and were associated with reduced social self-efficacy and fewer social contacts (Brohan et al., 2010). Other studies have shown that self-stigma is associated with lower psychosocial functioning (Muñoz et al., 2011) and that women and men have different worries with regard to perceived stigma and relationships (Jenkins and Carpenter-Song, 2009).
Men and women with psychosis may differ in social functioning, therefore requiring different approaches for improving social participation. In a 1990 study, women attended psychotherapeutic treatment more than men, while workplace rehabilitation and social skills training was focused on the men (Salokangas and Stengård, 1990). However, premorbid heterosexual development, negative symptoms, and working capacity were poorer in men than women, and poorer functioning was attributed to premorbid development (Salokangas and Stengård, 1990). Gender differences in social functioning for adults with psychosis show mixed findings. For example, a Finnish cohort found that living with their family rather than alone was associated with better social functioning for men with schizophrenia but that the reverse was true for women (Salokangas, 1997). The first Australian survey of psychosis revealed that men with psychosis had poorer self-care, fewer friends, less family support and less employment than women (Evert et al., 2003).
Opportunities for social participation and the practical conditions that enable participation are crucial to the social inclusion of people with psychosis. Reduced social support and opportunities for social participation are evident for young people experiencing a first episode of psychosis, as shown by smaller social networks and having fewer people to turn to in a crisis than peers without a mental illness (Macdonald et al., 2000). Similarly, elderly people with schizophrenia reported having less contact with their community, fewer outings from their home and fewer leisure activities than either peers with depression or peers without a mental illness (Graham et al., 2002). Further, a time use study within a British prevalence survey indicated that older people with schizophrenia spent less time socialising than their younger counterparts, resembling findings in the general population (Harvey et al., 2006; Shimitras et al., 2003). Young people with schizophrenia reported that insufficient finances impeded engagement in social activities (Mattsson et al., 2008); and this was also found in a more middle aged sample (Borras et al., 2007). Worryingly, 72% of discretionary income for the older sample was spent on addictive substances rather than social or leisure activities (Borras et al., 2007).
Being employed rather than on a disability pension provides opportunity for social contact with others at work and increases the income available for leisure activities. People with schizophrenia who are employed show better social functioning, possibly because more socially able people are successful at gaining and maintaining employment (Burns et al., 2009). Compared to individuals who were unemployed and had no history of mental illness, young adults with schizophrenia spent less time in social or leisure activities (Hayes and Halford, 1996). There is an opportunity for intervention as leisure activities and social relationships have been frequently cited as impacting positively on quality of life for people with schizophrenia (Pitkanen et al., 2009).
While substantial research is underway on the other two important factors for social inclusion, namely education and employment, less progress has been made with research into social participation, and in particular, opportunities for social participation, which will be addressed in a forthcoming article. Our research aims to examine the social functioning and opportunity for social participation of adults with psychosis to identify barriers to participation and potential modes of intervention to enhance social inclusion.
Method
Participants
A total of 1825 adults aged 18–64 years (M = 38.36 years, SD = 11.16) who participated in the second national survey of psychosis in Australia were included in the present study. The survey covered an area of 62,000 km2 and a population of 1.5 million people aged 18–64 years, approximately 10% of the Australian population in this age group. A two-phase design was used. In phase 1, screening for psychosis took place in public specialised mental health services and in non-government organisations supporting people with a mental illness, using face-to-face screening during the census month, March 2010, and through an audit of hospital records for all contact with psychosis-positive persons within the age range during the 11 months prior. In phase 2, people who were screened positive for psychosis in phase 1 were randomly selected and stratified by age group (18–34 years and 35–64 years), for interview and assessment. Of the 7955 people who were screened positive for psychosis and eligible, 1825 were interviewed in phase 2. Data were collected on symptomatology, substance use, cognitive ability, functioning, disability, physical health, mental health service utilisation, medication use, education, employment and housing. The study was approved nationally and by the Institutional Ethics Committees of each of the seven sites, and all participants provided written informed consent. The full details of the methodology can be found in this issue of the journal (Morgan et al., 2012).
Measures
Items were extracted from the main interview schedule to assess: (1) the nature of participants’ relationships with family and friends; (2) the availability of supportive relationships; (3) engagement in social activities and/or programs during the previous year; (4) social isolation and withdrawal; (5) participants’ perceptions of the barriers to engaging in social activities; and (6) participants’ overall level of social functioning. Socio-demographic variables and items assessing illness characteristics were examined in relation to their association with socialising, social isolation and withdrawal. Items were sourced from the Diagnostic Interview for Psychosis-Diagnostic Module (DIP-DM) (Castle et al., 2006), the 2007 National Survey of Mental Health and Wellbeing (NSMHWB) (Slade et al., 2009), SANE Australia Research Bulletins (SANE Australia, 2012) and the STIGMA Shout Survey (SSS) (Corry, 2008). The Personal and Social Performance (PSP) scale (Morosini et al., 2000) provided measures of overall social functioning. The overall socialising measure from the DIP-DM was used to create two groups for comparative analyses: (1) those with ‘no dysfunction’ and (2) those with ‘obvious or severe dysfunction’ (decreased social drive, no friends/limited social interaction with others outside the household) in socialising during the last year. Items relating to illness characteristics were sourced from the DIP-DM and diagnoses were derived from the 10th revision of the International Statistical Classification of Diseases and Related Health Problems (ICD-10) (World Health Organization, 2010).
Data analyses
The chi-square test of independence was used to assess possible associations between gender/illness characteristics and the categorical socialising factors variables. Adjusted standardised residuals were used to identify cells that contributed to significant chi-square values. Independent samples t-tests were used to assess group differences on socialising factors/illness characteristics by gender and social adjustment. The effect size of all significant results was assessed by Cramér’s V and Cohen’s d for categorical and continuous analyses, respectively. All analyses were conducted using the Statistical Package for Social Sciences (SPSS) for Windows, version 19 (SPSS Inc., Chicago, Illinois, USA).
Results
More than half the sample was male (59.6%), single or never married (61.2%), and 48.8% had attained post- secondary educational qualifications. Almost one-third of participants (31.7%) lived alone and similarly about one-third (32.7%) had been engaged in some form of employment in the past year. The average duration of illness was 14.65 years (SD = 10.4), with many participants (61.5%) having experienced multiple episodes. About half of the participants had a diagnosis of schizophrenia (47%), while 17.5% and 16.1% had been diagnosed with bipolar disorder or schizo-affective disorder, respectively. A total of 37.2% of participants identified loneliness and social isolation as some the biggest challenges or difficulties expected in the next year, while 11.6% identified the experience of stigma and 6.7% the absence of family and carers as their biggest expected challenges.
Demographics and clinical characteristics by social functioning (No dysfunction vs. obvious or severe dysfunction)
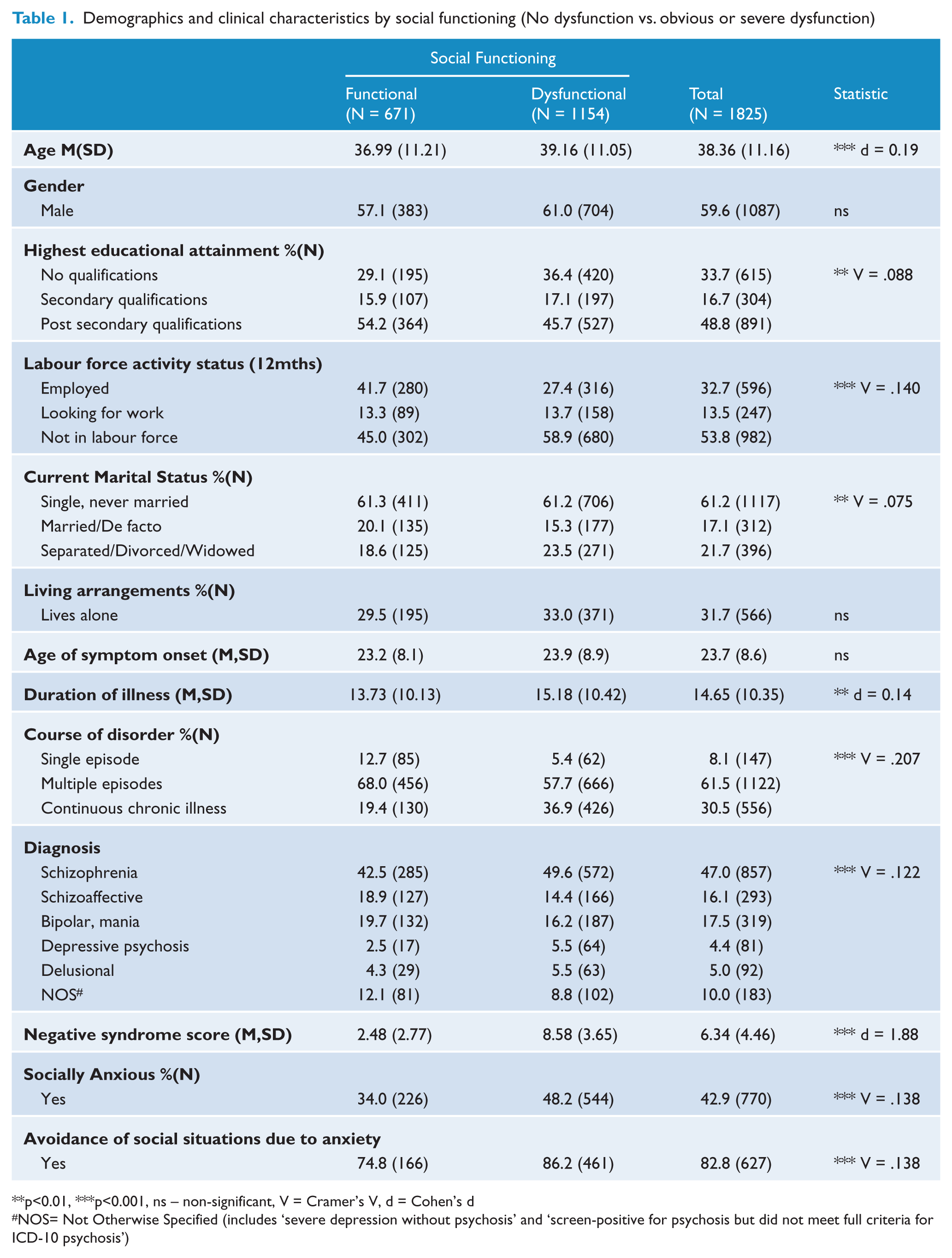
p<0.01, ***p<0.001, ns – non-significant, V = Cramer’s V, d = Cohen’s d
NOS= Not Otherwise Specified (includes ‘severe depression without psychosis’ and ‘screen-positive for psychosis but did not meet full criteria for ICD-10 psychosis’)
Social functioning and relationships in the past 12 months (by gender)
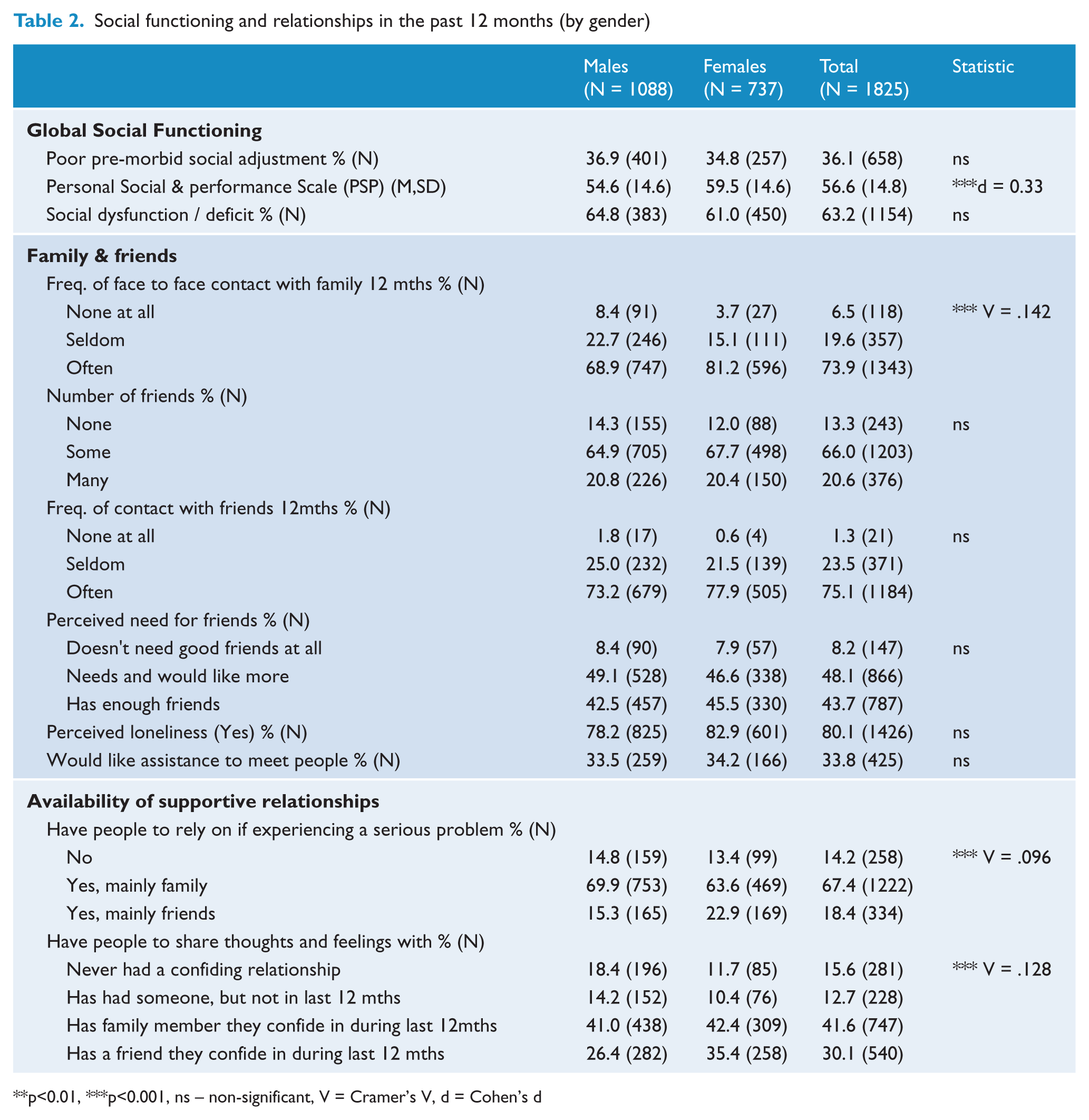
p<0.01, ***p<0.001, ns – non-significant, V = Cramer’s V, d = Cohen’s d
The socially dysfunctional group (obvious or severe dysfunction) was significantly older than the socially functional group. [t(1823) = −4.02, p < 0.001]. Significant associations were identified between level of social functioning and: (1) educational attainment [no qualifications were associated with poorer social functioning; χ2(4) = 14.22, p < 0.01]; (2) labour force activity [those not in the labour force were more likely to have poorer functioning; χ2(2) = 35.57, p < 0.001]; and (3) marital status [married or de facto participants were more likely to have good social functioning; χ2(2) = 10.28, p < 0.01].
Those classified as socially dysfunctional reported a longer duration of illness [t(1813) = −2.87, p < 0.01] and had a higher negative syndrome score than the functional group [t(1823) = −40.26, p < 0.001]. Significant associations were identified between the level of social functioning and: (1) course of the disorder [chronic continuous illness more likely to be socially dysfunctional; χ2(2) = 78.13, p < 0.001]; (2) diagnosis [a diagnosis of schizophrenia or depressive psychosis associated with the socially dysfunctional group; χ2(5) = 27.10, p < 0.001]; and (3) social anxiety [socially dysfunctional group more likely to indicate experiencing social anxiety; χ2(1) = 78.13, p < 0.001; and to avoid social situations due to this anxiety; χ2(1) = 14.32, p < 0.001].
Social activities, programs, and perceived barriers to participation in the past 12 months (by gender)
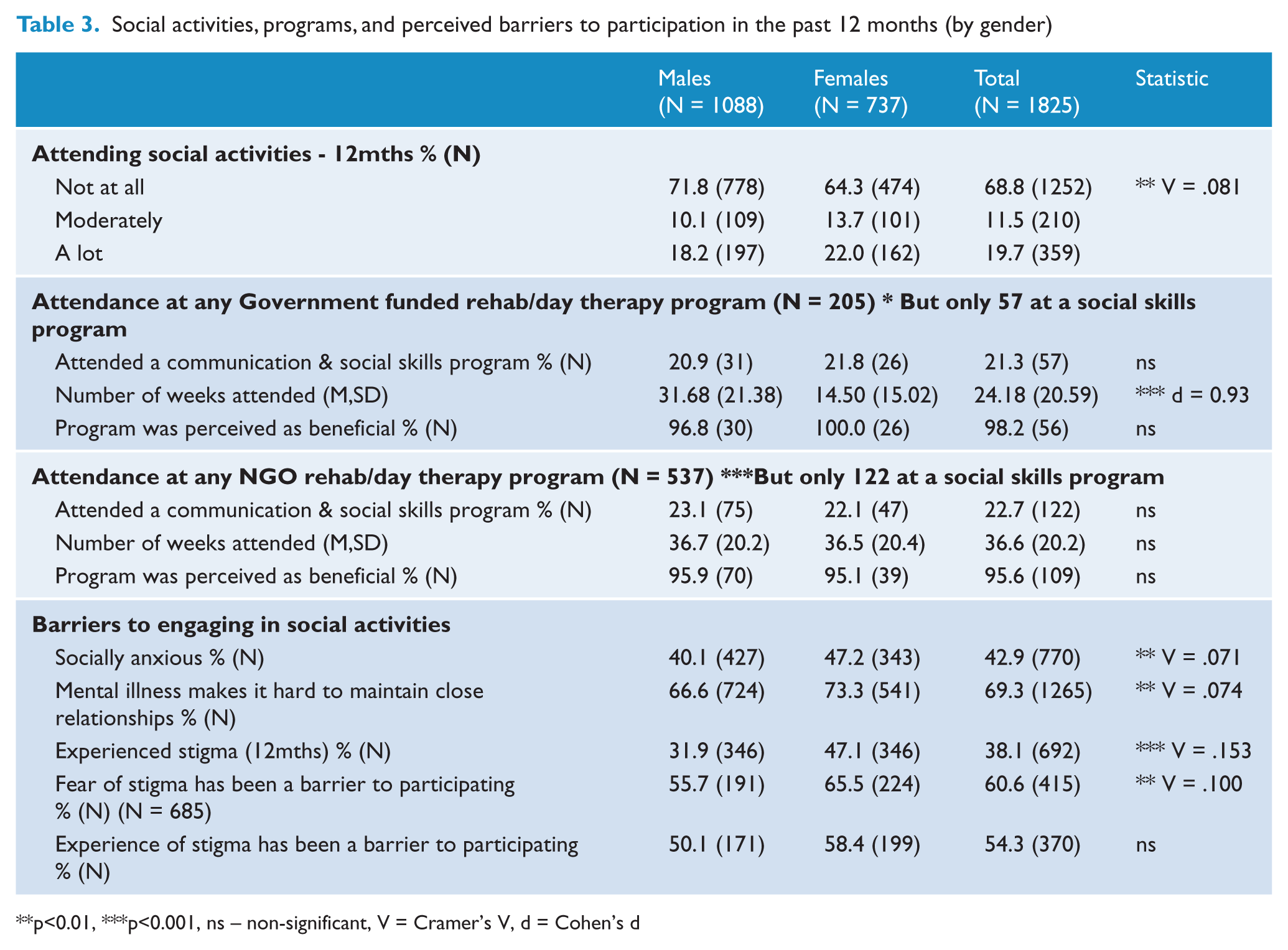
p<0.01, ***p<0.001, ns – non-significant, V = Cramer’s V, d = Cohen’s d
Friends and supportive relationships
Overall, 63.2% of participants were classified as having a social deficit, with a mean score of 56.6 (SD = 14.8) out of a possible score of 100 on the PSP (indicative of marked difficulties in one or more social activities, or manifest but not marked difficulties accompanied by disturbing or aggressive behaviour). Most respondents reported having daily or nearly daily contact with family members (56.7%), relying mainly on family members for support in an emergency (67.4%) and confiding in family members (41.6%) during the past year. Just over half the sample (54.7%) reported having ‘a few friends’ with whom they had at least weekly (75.1%) contact. Despite this, many participants indicated experiencing loneliness (80.1%) and a need for more friends (48.1%). In addition, one-third of participants (33.8%) stated that they would like assistance to develop new friendships.
Females scored significantly higher on the PSP than males [t(1823) = −6.99, p < 0.001]. Significant associations were found between gender and: (1) frequency of contact with family members [females were more likely to have daily contact with family members in the past year; χ2(2) = 36.72, p < 0.001]; (2) having someone to rely on in an emergency [females were more likely to have people they can rely on; χ2(2) = 16.87, p < 0.001]; and (3) having someone to confide in [females were more likely to have confided in a friend in the past year; χ2(3) = 29.21, p < 0.001].
Social activities, programs and barriers
The main barriers to engaging in social activities were the perception that mental illness makes it hard to maintain close relationships (69.3%), and a fear of stigma or discrimination due to mental illness (60.6%). Significant associations were found between gender and: (1) attending a social activity [females were more likely to have attended a social activity; χ2(2) = 11.84, p < 0.01]; (2) social anxiety [females were more likely to experience anxiety in social situation; χ2(1) = 8.95, p < 0.01]; (3) mental illness as a barrier [females were more likely to agree that mental illness interferes with the maintenance of close relationships; χ2(2) = 9.94, p < 0.01]; (4) experience of stigma [females were more likely to have experienced stigma; χ2(1) = 42.49, p < 0.001]; and (5) the fear of stigma associated with mental illness [females again were more likely to forgo social participation due to fear of stigma; χ2(1) = 6.09, p < 0.01].
Associations of social participation with illness course and onset
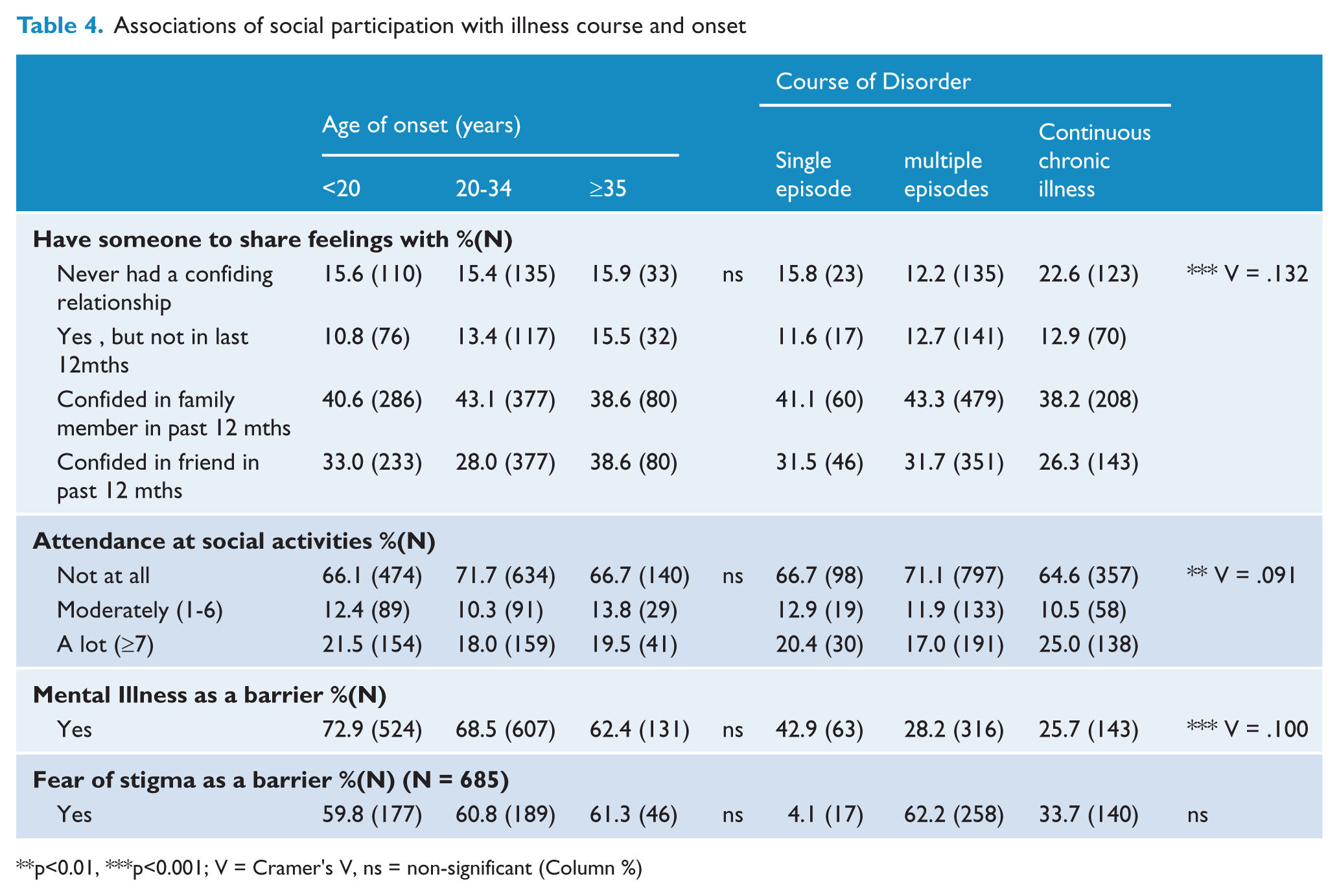
p<0.01, ***p<0.001; V = Cramer’s V, ns = non-significant (Column %)
Overall, the majority of participants had not attended any organised social rehabilitation programs (68.8%) over the past year. Of the 205 people who had attended a government-funded day therapy program, only 21.3% had participated in a program specifically designed to enhance communication and/or social skills in the last year. A similar proportion (22.7%) of people attending non-government-operated services had participated in communication and/or social skills programs in the last year. Of those people who did attend such programs, 98.2% and 95.6% of people found the government and non-government programs, respectively, to have been beneficial.
Illness course, premorbid adjustment and social anxiety
No significant association was found between age of onset and relationship or social activity variables. There were, however, significant associations between course of disorder and: (1) having someone to confide in [those who experienced multiple episodes were more likely to have never had a confiding relationship, and those with continuous chronic illness were more likely to have confided in a friend in the last year; χ2(6) = 31.35, p < 0.001]; (2) attendance at social activities [those who experienced multiple episodes were more likely to have not attended activities, and those with continuous chronic illness were more likely to have attended social activity programs in the last year; χ2(6) = 31.35, p < 0.001]; and (3) mental illness as a barrier [those who experienced a single episode were less likely to agree that mental illness is a barrier to participation; χ2(4) = 18.16, p = 0.001].
Significant associations were found between premorbid social adjustment and: (1) having someone to confide in [those with poor premorbid adjustment were more likely to have never had a confiding relationship in the past year; χ2(3) = 22.33, p < 0.001]; and (2) mental illness as a barrier [those with poor premorbid social adjustment were more likely to agree that mental illness is a barrier to maintaining close relationships; χ2(2) = 15.45, p < 0.001]. Significant associations were also found between social anxiety and: (1) having someone to confide in [people who were socially anxious were more likely to have never had a confiding relationship; χ2(3) = 11.55, p < 0.001]; (2) mental illness as a barrier [socially anxious adults were more likely to agree that mental illness is a barrier to maintaining close relationships; χ2(2) = 111.20, p < 0.001]; and (3) fear of stigma as a barrier to social participation [socially anxious participants were more likely to agree that fear of stigma prevented them from participating socially; χ2(1) = 26.60, p < 0.001].
Associations of social participation with premorbid social functioning and current social anxiety
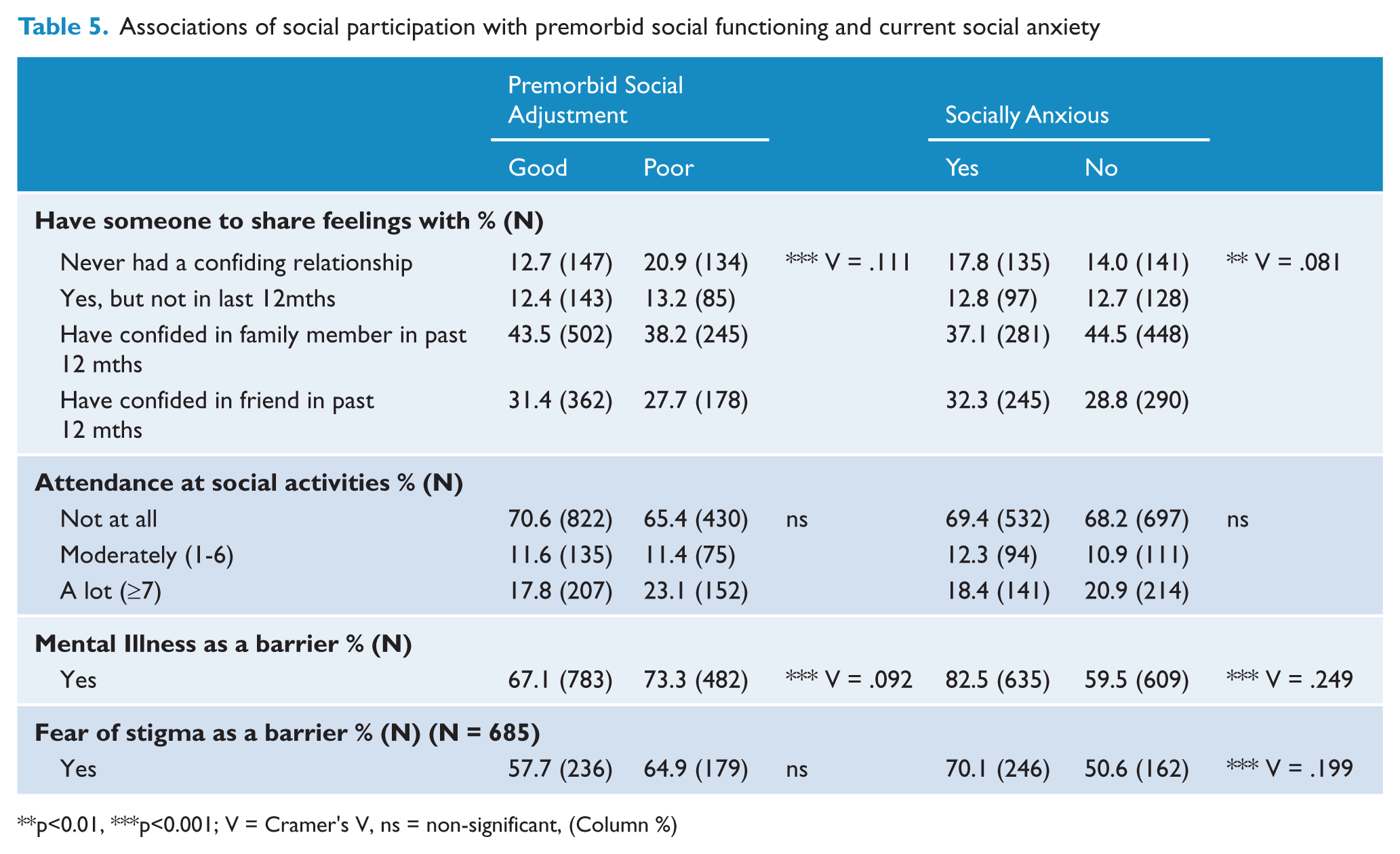
p<0.01, ***p<0.001; V = Cramer’s V, ns = non-significant, (Column %)
Significant associations were also found between scores on the global PSP measure and: gender (r = 0.162, p < 0.01; point-biserial correlation); age of onset (r = 0.096, p < 0.01; Pearson’s r); course of disorder (r = −0.264, p < 0.01, Pearson’s r); and premorbid social adjustment (r = −0.146, p < 0.01, biserial correlation). These results suggest that being female, older age at onset, less severe course of disorder and better premorbid social adjustment were associated with higher scores on the PSP measure.
Discussion
It is increasingly recognised that social relationships contribute to quality of life for people with serious mental illness (Pitkänen et al., 2009), as well as to overall outcome and recovery (Albert et al., 2011; Harvey et al., 2007). More than one-third of participants in the second Australian national survey of psychosis identified social isolation and loneliness as the biggest challenges facing them in the next year. By comparison, rates of social isolation in the general community are reported to be around 7% (Hawthorne, 2008). Further, almost two-thirds of survey participants were assessed to have significant levels of dysfunction in their capacity to socialise over the past year, compared with under 60% in the first national survey (Jablensky et al., 1999). Adults with significant social functioning impairment were more likely to be unemployed, single and have low educational attainment, thus illustrating the need to address education, employment and social functioning when seeking to improve social inclusion for people with psychosis, as suggested in the first national survey (Evert et al., 2003). The majority of adults reported experiencing loneliness, and nearly half expressed a need for more friends, slightly more than in the first survey (Jablensky et al., 1999). Only 20% of adults had accessed a social skills program in the past year and yet 34% stated they wanted help to meet people. Worryingly, the social isolation and dysfunction experienced by Australians with psychosis have not decreased since the last survey, despite evidence of greater access to community rehabilitation and day programs (Morgan et al., 2011). Therefore, these findings suggest that improved understanding of factors contributing to reduced social functioning and participation, as well as the identification of appropriate policy and service delivery responses, are warranted.
Nearly two-thirds of adults were rated as having significant social functioning impairment and this was associated with a longer duration of illness, having a chronic course of disorder and a diagnosis of schizophrenia or depressive psychosis. Unsurprisingly, social anxiety and its subsequent avoidance of social activities were more likely for this group. Higher levels of social functioning were associated with being female, older age at onset, less severe course of disorder, and better premorbid social adjustment.
Women showed significantly better overall social functioning than men. In the past year, women were more likely than men to have had daily contact with family, had friends to rely on in an emergency, to have confided in a friend and engaged in social activities. This is consistent with previous studies of people with psychosis (Sörgaard et al., 2001) and studies of the general population (Fuhrer and Stansfeld, 2002). However, women in this survey were also more likely to report barriers to engaging in social activities. For instance, women reported higher rates of social anxiety and were more likely to perceive their mental illness as interfering with their ability to maintain close relationships. Women in the study were more likely to have experienced stigma and to avoid social participation due to a fear of experiencing stigma.
The findings of greater engagement in social activities of women compared with men, but greater perceived barriers for women, suggests women with psychosis may have a greater drive for social participation than their male counterparts. Certainly, community studies show that women focus more on relationships and value emotional connectedness more than men (Haines et al., 2008). However, despite only 10% of adults with psychosis accessing a social skills program in the past year, men were just as likely as women to attend such a program. Importantly, those accessing the social skills programs were more likely to have a chronic course of illness and this may reflect a lack of availability of social skills programs for adults with a less debilitating course of illness and/or the deliberate allocation of available resources to those most in need. Given that nearly all participants in these programs rated the programs as beneficial and the majority of the participants in the study expressed a need for assistance in making friends, wider implementation of social skills programs for adults with psychosis is warranted, consistent with recommendations in local and international clinical guidelines (see RANZCP, 2005). Further, greater access to companionship through befriending and peer support initiatives may also be useful to enhance social participation (Davidson et al., 2001).
The course of psychotic illness, and in particular the occurrence of multiple episodes of psychosis, was associated with less likelihood of having a confiding relationship or engaging in social activities. By contrast, a continuous chronic course of illness was associated with a greater likelihood of confiding in a friend in the past year or having attended a social skills program. Such findings for a chronic course of illness may reflect the targeting of ‘rehabilitation’ programs, such as social skills interventions, towards the more chronic end of the illness spectrum of psychosis. Alternatively, those with a chronic course may have more stability and predictability, enabling them to establish long-term friendships. The experiences and needs expressed by adults in this second national survey of psychosis highlight a potentially unmet need for social functioning interventions across the spectrum of illness and across the age range.
Poor premorbid social adjustment as assessed in the diagnostic interview was found to be associated with less likelihood of having a confiding relationship and increased likelihood of perceiving mental illness as a difficulty for maintaining close relationships. The lack of a significant association between age of onset and social participation requires further investigation and may have been the result of poor sensitivity of measures or limited assessment of premorbid features.
Social anxiety was reported by nearly half of the adults with psychosis and associated with less likelihood of having a confiding relationship and an increased chance of perceiving mental illness as a problem in maintaining close relationships or reporting a fear of stigma as a barrier to social participation. This is an important finding suggesting that it may be beneficial to separately address comorbid social anxiety with specific psychological interventions (Lucas et al., 2010) as an additional means of improving social participation among people with psychosis.
Limitations
These results provide some of the most comprehensive information available on social functioning in adults with psychosis. This area has received little attention to date, and the current research gives rise to as many questions as it does provide answers on social functioning needs and service delivery to enhance social inclusion. For example, the survey did not assess social cognition skills that are likely to be a barrier to social participation. As the survey was a cross-sectional study, it is not possible to delineate causality and therefore establish whether reduced social inclusion for people with psychosis arises from impaired social functioning or vice versa. A more detailed assessment of premorbid social functioning, such as that provided by the Strauss–Carpenter Scale of premorbid adjustment (Strauss and Carpenter, 1972) would have elicited more on the role of premorbid functioning in the social functioning of adults.
Conclusion
The study extends the knowledge of psychosis gained from the first Australian national survey of psychosis to provide an understanding of the real-life experiences of people with psychosis. Nearly two-thirds of adults with psychosis had significant social functioning impairment and this was associated with being unemployed, single and having low educational attainment. Although one-third of adults stated they wanted help to meet people, only a small proportion had accessed a social skills program and the majority of attendees were those with a chronic course of illness. Given such findings, it appears important to review the social intervention programs available for people with psychosis to ensure that all those in need are able to access appropriate programs. The UK Foresight Mental Capital and Wellbeing project recommended that people with mental illness focus on five ways of achieving well-being – connect with people, be active, take notice of the world around you, keep learning and give to others by taking part in volunteer activities (Government Office for Science, 2008). Population-based time use studies have shown that age-related differences in participation rates in social (and other) occupations for people with psychosis are similar to those for the general population (Harvey et al., 2006). This indicates that societal issues need to be addressed, in addition to treatment effectiveness, to improve social participation. Four recommended approaches to improve social inclusion for people with mental health problems are: legislation, community support and services, anti-stigma campaigns and system monitoring and evaluation (Cobigo and Stuart, 2010). The challenge remains for policymakers and service providers to implement such methods to achieve increased rates and quality of social and community participation for people with a mental illness.
Footnotes
Acknowledgements
This publication is based on data collected in the framework of the 2010 Australian National Survey of High Impact Psychosis. The members of the Survey of High Impact Psychosis Study Group are: V. Morgan (National Project Director), A. Jablensky (Chief Scientific Advisor), A. Waterreus (National Project Coordinator), R. Bush, V. Carr, D. Castle, M. Cohen, C. Galletly, C. Harvey, B. Hocking, A. Mackinnon, P. McGorry, J. McGrath, A. Neil, S. Saw and H. Stain. The site coordinators were: A. Baker, L. Campbell, J. Green, J. Griffith, M. Hanlon, M. Haydock, L. Hayes, A. Poon and S. Sweeney. The interviewers were: L. Anthes, N. Atkinson, F. Barclay, K. Barrack, L. Bates, A. Brown, R. Bush, I. Cairney, R. Caley, S. Dixon, L. Dixon, K. Douglas, L. Drinkwater, P. Edwards, V. Fenby, C. Harper, M. Heath, B. Hulse, E. Killen, L. Niven, D. Novello, D. Rich, G. Roddis, K. Scholes, S. Turner and J. Waterson. Population statistics from the 2007 National Survey of Mental Health and Wellbeing matching the psychosis survey age criteria were provided by Dr. Tim Slade. Ethics approvals for the study were obtained from the relevant institutional human research ethics committees. We acknowledge, with thanks, the hundreds of mental health professionals and general practitioners who participated in the preparation and conduct of the survey and the many Australians with psychotic disorders who gave their time and whose responses form the basis of this publication.
Funding
The study was funded by the Australian Government Department of Health and Ageing.
Declaration of interest
The authors report no conflicts of interest. The authors alone are responsible for the content and writing of the paper.