
Abstract
Background:
Social inclusion is crucial to mental health and well-being and is emphasised in Australia’s Fourth National Mental Health Plan. There is a recognition that a measure of social inclusion would complement the suite of outcome measures that is currently used in public sector mental health services. This paper is an initial scope of candidate measures of social inclusion and considers their suitability for this purpose.
Methods:
We identified potential measures through searches of PsycINFO and Medline and a more general Internet search. We extracted descriptive and evaluative information on each measure identified and compared this information with a set of eight criteria. The criteria related to the measure’s inclusion of four domains of social inclusion outlined in Australia’s Fourth National Mental Health Plan, its usability within the public mental health sector and its psychometric properties.
Results:
We identified 10 candidate measures of social inclusion: the Activity and Participation Questionnaire (APQ-6); the Australian Community Participation Questionnaire (ACPQ); the Composite Measure of Social Inclusion (CMSI); the EMILIA Project Questionnaire (EPQ); the Evaluating Social Inclusion Questionnaire (ESIQ); the Inclusion Web (IW); the Social and Community Opportunities Profile (SCOPE); the Social Inclusion Measure (SIM); the Social Inclusion Questionnaire (SIQ); and the Staff Survey of Social Inclusion (SSSI). After comparison with the eight review criteria, we determined that the APQ-6 and the SCOPE–short form show the most potential for further testing.
Conclusions:
Social inclusion is too important not to measure. This discussion of individual-level measures of social inclusion provides a springboard for selecting an appropriate measure for use in public sector mental health services. It suggests that there are two primary candidates, but neither of these is quite fit-for-purpose in their current form. Further exploration will reveal whether one of these is suitable, whether another measure might be adapted for the current purpose or whether a new, specifically designed measure needs to be developed.
Keywords
Background
People with mental health problems are one of the most socially excluded groups in society (Social Exclusion Unit, 2004). While social exclusion is known to be a risk factor for the development of mental health problems (Bertram and Stickley, 2005), social inclusion can have protective benefits, ameliorating the negative effects of stress, and contributing to mental illness recovery (Harrison and Sellers, 2008). Once established, mental illness in turn can have a detrimental effect on social competence, confidence and self-esteem (Anthony, 1993; Borba et al., 2011; Hooley, 2010) and can reduce opportunities for social interaction and participation in all aspects of life (Hooley, 2010; Social Exclusion Unit, 2004), creating a maintaining cycle of social isolation that is seen most vividly in those with chronic mental illness (Anthony, 1993; Borba et al., 2011; Hooley, 2010). For this reason, Australia’s Fourth National Mental Health Plan (Australian Health Ministers, 2009) emphasises social inclusion for people with a mental illness, with the first of its five priority areas being ‘Social Inclusion and Recovery’.
Despite increasing recognition of the importance of ‘social inclusion’ to mental health and well-being, the precise meaning of the term is the subject of some debate (Marino-Francis and Worrall-Davies, 2010). Different commentators have offered different definitions (see Box 1 for examples) that vary widely (Morgan et al., 2007). However, a number share commonalities in their focus on the importance of those with mental illness having access to, and participating in, all opportunities and choices afforded to other people (Bates and Repper, 2001; Mental Health Commission, 2009; Slade, 2009) and the inclusion of both an objective and a subjective element (Huxley et al., 2006; Le Boutillier and Croucher, 2010; Morgan et al., 2007). The objective element relates to the extent to which the individual participates in various life domains and is often measured by counting time spent participating in activities within the community (e.g. ‘Number of days in the past week in which participated in employment’) (Lloyd et al., 2008) and the number of activities participated in and/or the number of social contacts available (e.g. ‘Total number of people in support network “when feeling down in the dumps” ’) (Lloyd et al., 2008). The subjective element refers to whether the individual feels that their participation matches his or her preferences; this is generally measured by assessing the person’s satisfaction with his or her experience (e.g. ‘How do you feel about your range of opportunities to access suitable accommodation?’) (Huxley et al., 2012) or a desire for change (e.g. ‘Are you interested in increasing your participation in the following: employment, unpaid, education and training?’) (Stewart et al., 2010).
Selected definitions of social inclusion
Social inclusion is …
… about each person taking part in society and having control over his or her own resources. It is also about a community that cares for its members, makes them feel welcome and is willing to adjust to fit their various needs (Marino-Francis and Worrall-Davies, 2010)
… the extent to which people are able to exercise their rights and participate, by choice, in the ordinary activities of citizens (Mental Health Commission, 2009)
… a person’s right to participate as an equal citizen in all the opportunities available, employment, education and other social and recreational activities (Slade, 2009)
… full access to mainstream statutory and post-16 education, open employment and leisure opportunities alongside citizens who do not bear these (mental illness) labels (Bates and Repper, 2001)
… a virtuous circle of improved rights of access to the social and economic world, new opportunities, recovery of status and meaning, and reduced impact of disability (Sayce, 2001)
Those life domains that are seen as essential to social inclusion are also not well established (Morgan et al., 2007). However, there is some degree of acceptance of the importance to mental health of access to employment and/or education (Department of Health, 2001; HM Government, 2010; Social Inclusion Unit, 2011), stable housing (Harvey et al., 2002; Huxley et al., 2006), community participation (Harvey et al., 2002; Social Inclusion Unit, 2011) and social networks (Harvey et al., 2002; Huxley et al., 2006). Consequently, Australia’s Fourth National Mental Health Plan outlines five indicators against which to measure desired change in the area of social inclusion: (1) participation rates by people with mental illness of working age in employment; (2) participation rates by young people aged 16 to 30 with mental illness in education and employment; (3) percentage of mental health consumers living in stable housing; (4) rates of community participation by people with mental illness; and (5) rates of stigmatising attitudes within the community (Australian Health Ministers, 2009). Note that, given this is a government initiative, these domains reflect indicators that can be measured at the population level, rather than the individual level; hence the exclusion of social networks. Measuring levels of social inclusion for individuals accessing mental health services can help to measure progress across Australia on this important component of Australia’s mental health strategy. It can also help services to identify whether their practices are promoting social inclusion as a key component of recovery and measurement can promote discussion between individual service providers and mental health service users about strategies to promote social inclusion.
In addition to striving to perform well against the above indicators, the Fourth National Mental Health Plan commits to measuring outcomes for consumers using public sector mental health services (Australian Health Ministers, 2009). The current suite of outcome measures, which includes the Health of the Nation Outcomes Scale (HoNOS) (Wing et al., 2000), the Mental Health Inventory (MHI) (Veit and Ware, 1983), the Behaviour and Symptom Identification Scale 32 (BASIS-32) (Eisen et al., 1986) and the Kessler-10 Plus (K-10+) (Centre for Population Studies in Epidemiology, 2002), is fairly clinical in focus and emphasises reductions in symptomatology and improvements in levels of functioning (Pirkis and Callaly, 2010). A national protocol specifies those measures that should be collected within particular mental health settings and at which time points. For example, the HoNOS is collected for all adults in inpatient, community residential and ambulatory settings at admission, review and discharge from mental health care (Australian Mental Health Outcomes and Classification Network, 2005).
There is recognition that a measure of social inclusion may need to be added to this suite. Such a measure should reflect the first four indicators described above (the fifth needs to be gauged through community surveys) and should include some of the more subjective components of social inclusion (Le Boutillier and Croucher, 2010). The process for collection of social inclusion data would need to be developed in consideration of the measure chosen for this purpose and specified in the national protocol.
A suitable measure for standard use would need to meet certain psychometric criteria as well as being usable within community mental health services. Psychometrically, the measure must be valid, reliable and sensitive to change (Stewart et al., 2010). In order to increase the likelihood of completion, the measure should also be brief, inexpensive, simple to administer, score and interpret (Stewart et al., 2010), preferably be completed by consumer self-report, and be acceptable to mental health consumers.
The imperative to identify a quality measure of social inclusion for potential use in public sector mental health services led us to review the existing measures. We aimed to identify available individual-level candidate measures of social inclusion, to describe their characteristics and to undertake a preliminary examination of their potential for routine use in the current context.
Method
We searched PsycINFO and Medline for articles published between January 2010 and the end of January 2012, using the terms (‘social inclusion’ OR ‘community participation’ OR ‘social capital’ OR ‘social isolation’) AND (‘mental health’) AND (‘measure’). We also conducted a general Internet search, via Google, using the term ‘social inclusion measure’.
We then used the measure names as search terms in PsycINFO and Medline to identify any papers that outlined further psychometric testing of the social inclusion measures identified in the initial search. Where the actual measures were not publicly available, we wrote to the corresponding author to request a copy.
We used eight criteria to review the quality and utility of the candidate social inclusion measures:
measures multiple domains of social inclusion, including employment, education, housing and community participation;
measures both objective and subjective components of social inclusion;
is self-completed by the consumer;
yields qualitative data (not excluding measures that also yield qualitative data);
is relatively brief (50 items or less);
has tested usability with mental health consumers;
is applicable to the Australian context;
has sound, established, psychometric properties.
To compare the measures using this standard set of criteria, we extracted descriptive information on each measure identified through the search. We only considered the published form of each measure in comparison with the criteria, inclusive of all scales and items, and we only considered the published mode of administration. Research evidence suggests that altering the tested mode of administration can affect a measure’s validity and outcomes (Bowling, 2005) and shortening measures alters its psychometric properties such that the shortened form then requires its own psychometric testing (Coste et al., 1997).
We extracted any available information on the psychometric testing of each measure. Specifically, we identified any resulting indicators of validity (i.e. the extent to which they measure what they purport to measure) (Greenhalgh et al., 1998) and reliability (i.e. the extent to which they give stable, consistent results) (Greenhalgh et al., 1998). Specifically, we examined construct validity (which involves conceptually defining the construct to be measured and assessing the internal structure of its components and the theoretical relationship of its items and subscale scores) and concurrent validity (which pits the instrument against a comparable measure at the same point in time). We operationalised reliability in terms of internal consistency (i.e. the extent to which items that reflect the same construct yield similar results) and test-retest reliability (i.e. the degree of agreement when the same measure is completed by the same person at two different points in time). We also considered each measure’s sensitivity to change. Sensitivity to change is related to both validity and reliability: a measure that is both valid and reliable and which demonstrates change over time can be regarded as being sensitive to change. We also attempted to identify whether the measure had undergone testing with mental health consumers and whether it had been tested within Australia.
Results
Search results
We identified the following 10 candidate individual-level measures of social inclusion:
Activity and Participation Questionnaire (APQ-6) (Stewart et al., 2010);
Australian Community Participation Questionnaire (ACPQ) (Berry et al., 2007);*
Composite Measure of Social Inclusion (CMSI) (Lloyd et al., 2008);*
EMILIA Project Questionnaire (EPQ) (Ramon et al., 2009);*
Evaluating Social Inclusion Questionnaire (ESIQ) (Stickley and Shaw, 2006);*
Inclusion Web (IW) (Hacking and Bates, 2008);
Social and Community Opportunities Profile (SCOPE) (Huxley et al., 2012);
Social Inclusion Measure (SIM) (Huxley et al., 2012; Secker et al., 2009);*
Social Inclusion Questionnaire (SIQ) (Marino-Francis and Worrall-Davies, 2010);*
Staff Survey of Social Inclusion (SSSI) (Dorer et al., 2009).*
Those marked with an asterisk were not named by their creators, usually because they were developed with the purpose of evaluating a given service and there was no explicit intention that they might have ongoing use. We have named them, based on the terminology used about them by their creators, in order that we could readily make reference to them in the remainder of this review.
More detail about each of these measures is provided in Table 1. The measures identified have been developed relatively recently in countries that have a current emphasis on social inclusion, notably Australia and the United Kingdom. The candidate measures cover a range of domains related to social inclusion, often including those emphasised in the Fourth National Mental Health Plan (especially employment, education and community participation) (Australian Health Ministers, 2009), and often focus on both objective and subjective experiences. Some (e.g. the CMSI) draw on questions from related instruments and/or national surveys; others (e.g. the IW) were developed for a specific study purpose. With the exception of the ACPQ, all were explicitly developed for use with people with mental illness. They vary in length: the APQ-6 is the shortest, with a maximum of 14 possible items, and the SCOPE–long version is the longest, with 121 items. The majority of measures elicit responses in the form of quantitative data; only the EPQ generates qualitative data. Almost all seek responses directly from consumers; only the SSSI uses staff as informants. The measures also represent a mix of self-report and interviewer-administered instruments, and the latter are sometimes explicitly designed to promote dialogue between service providers and consumers (e.g. the IW) (Berry et al., 2007; Dorer et al., 2009; Hacking and Bates, 2008; Huxley et al., 2012; Lloyd et al., 2008; Marino-Francis and Worrall-Davies, 2010; Ramon et al., 2009; Secker et al., 2009; Stewart et al., 2010; Stickley and Shaw, 2006).
Profile of social inclusion measures.
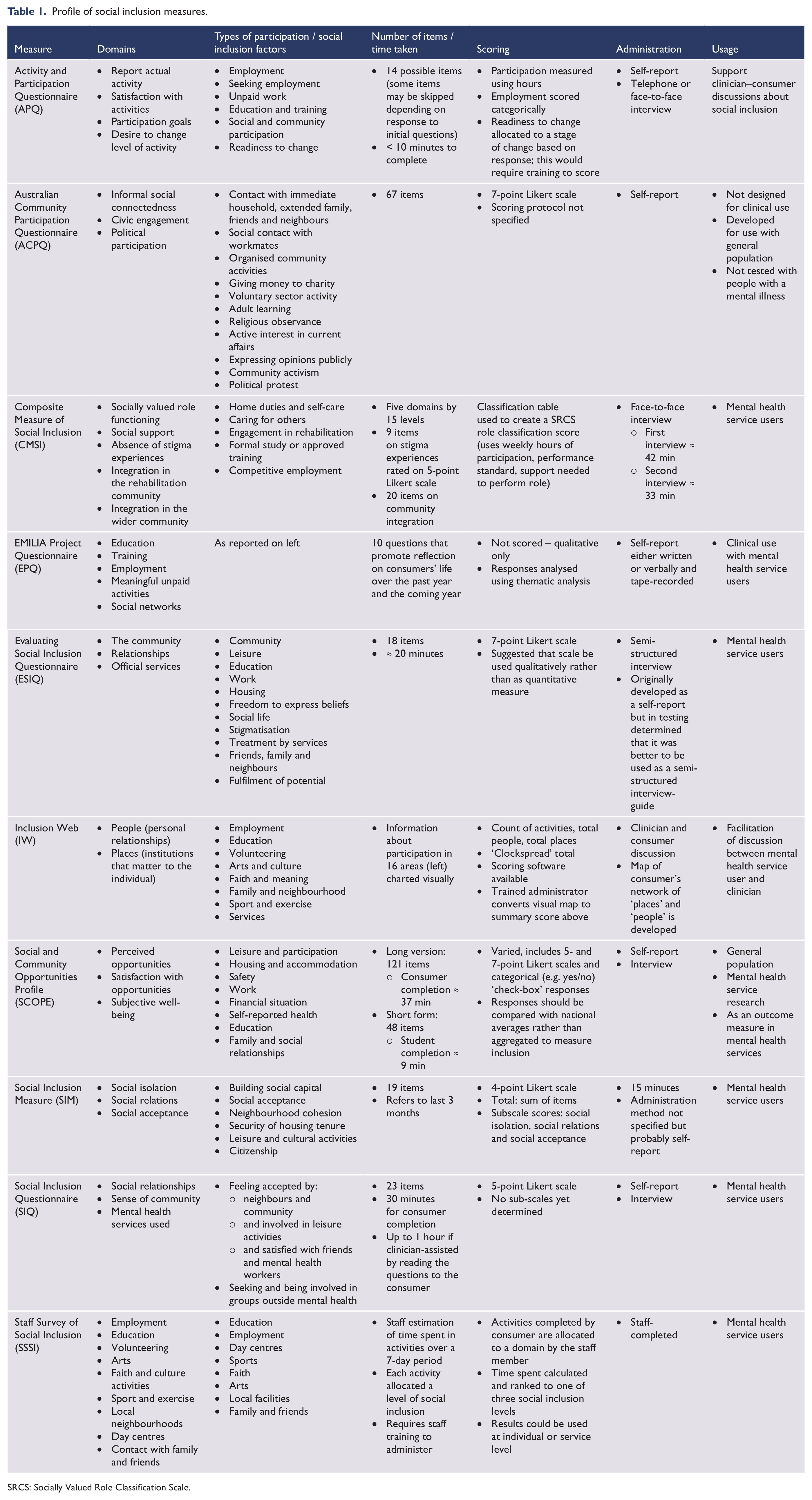
SRCS: Socially Valued Role Classification Scale.
Comparison of measures with criteria 1 to 7
We initially considered the usability of the measures by comparing the attributes of each measure with the first seven criteria. We then considered the psychometric properties of the measures (criterion 8). Comparing each measure with the first seven criteria, we found that:
The ACPQ, SIM and SIQ measure too few (two domains or less) of the domains of interest in the Fourth National Mental Health Plan (Australian Health Ministers, 2009).
The ACPQ, IW and SSSI focus on the objective components of social inclusion and do not pay sufficient heed to the subjective experiences of the consumer.
The CMSI, IW and ESIQ are administered as face-to-face interviews, rather than through self-report, limiting their usability in public mental health.
The qualitative nature of the EPQ means that although it may be useful at the individual level and may promote discussion between the service provider and the consumer, it is unlikely to generate information that can be aggregated across consumers for the purposes of monitoring broader changes in social inclusion.
The long version of the SCOPE is too long at 121 items, although the shorter, 48-item version may still be of use; the CMSI is also too long, taking approximately 40 minutes to complete the structured interview.
More than half of the measures have undergone scrutiny from the point of view of their acceptability to users (the APQ-6, CMSI, ESIQ, SCOPE, SIM, SIQ and SSSI). In the main, this has occurred in the context of their development and has sometimes resulted in modifications to questions or response sets. In all cases, feedback from users about these measures has been positive (Dorer et al., 2009; Huxley et al., 2012; Lloyd et al., 2008; Marino-Francis and Worrall-Davies, 2010; Secker et al., 2009; Stewart et al., 2010; Stickley and Shaw, 2006). The ACPQ has not been tested with mental health service users and is designed for the general population, and the acceptability of the EPQ and the IW is also not outlined in the literature.
Only the APQ-6, the ACPQ and the CMSI have undergone development and testing within Australia.
Considering comparison of the candidate measures with the first six criteria together, the APQ-6 and the SCOPE–short form are the only measures to meet all six criteria. The APQ-6, however, does not measure the domain of housing (included in criterion 1), but does have the advantage of having been developed and tested for use in the Australian context (criterion 7), while the SCOPE was developed and tested in the UK.
Comparison of measures with criterion 8: psychometric properties
Table 2 summarises existing information about the psychometric properties of each measure that has undergone some form of psychometric testing. Most of the measures have undergone some psychometric testing, albeit not extensively. The exceptions are the ESIQ, the SSSI and the EPQ. The EPQ, as noted above, elicits only qualitative information and is therefore not amenable to psychometric testing.
Psychometric properties of remaining social inclusion measures.
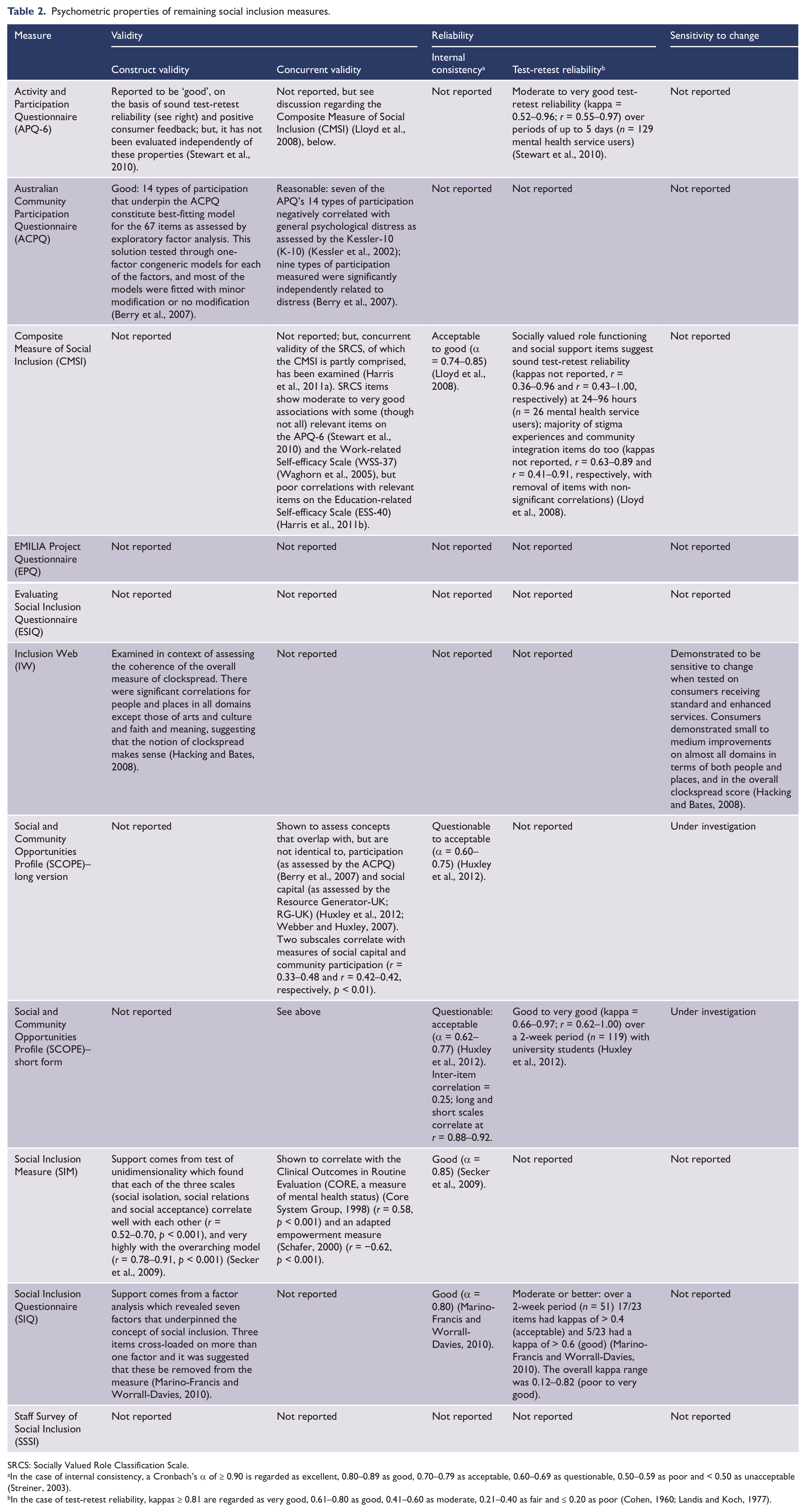
SRCS: Socially Valued Role Classification Scale.
In the case of internal consistency, a Cronbach’s α of ≥ 0.90 is regarded as excellent, 0.80–0.89 as good, 0.70–0.79 as acceptable, 0.60–0.69 as questionable, 0.50–0.59 as poor and < 0.50 as unacceptable (Streiner, 2003).
In the case of test-retest reliability, kappas ≥ 0.81 are regarded as very good, 0.61–0.80 as good, 0.41–0.60 as moderate, 0.21–0.40 as fair and ≤ 0.20 as poor (Cohen, 1960; Landis and Koch, 1977).
Collectively, those which have been tested have displayed a largely sound performance in terms of some or all of the following: construct validity, concurrent validity, internal consistency and test-retest reliability. The least tested property is sensitivity to change; this has only been explored for the IW, which was shown to be capable of identifying incremental improvements in social inclusion in a sample of mental health service users (Hacking and Bates, 2008). It is important to note that while some psychometric properties of the CMSI as a complete measure are noted in Table 3, the Socially Valued Role Classification Scale (SRCS), which comprises a large portion of the CMSI, has also undergone independent psychometric testing (Waghorn et al., 2007). This testing provides further evidence for the construct validity, test-retest reliability and sensitivity to change of some scales of the CMSI, though not of the measure as a whole.
Summary of attributes of social inclusion measures.
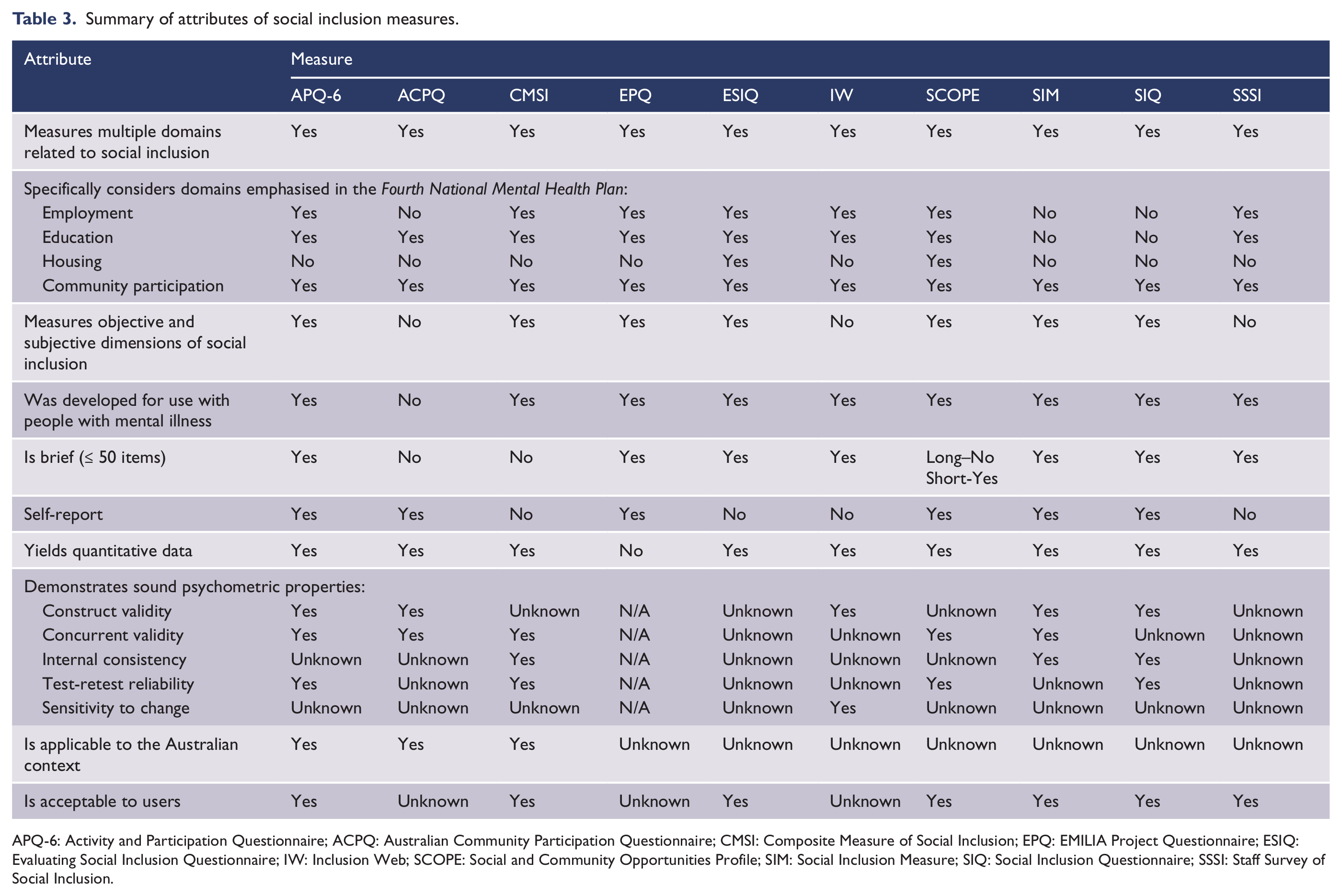
APQ-6: Activity and Participation Questionnaire; ACPQ: Australian Community Participation Questionnaire; CMSI: Composite Measure of Social Inclusion; EPQ: EMILIA Project Questionnaire; ESIQ: Evaluating Social Inclusion Questionnaire; IW: Inclusion Web; SCOPE: Social and Community Opportunities Profile; SIM: Social Inclusion Measure; SIQ: Social Inclusion Questionnaire; SSSI: Staff Survey of Social Inclusion.
Table 3 distils the above information about each measure and indicates whether the measure meets each criteria.
While no measure meets all eight of the criteria, both the APQ-6 and SCOPE–short form meet the majority of the criteria. Neither of these measures yet demonstrates all desirable attributes, partly because their psychometric properties require further testing, but also because the APQ-6 does not consider the domain of housing and because the SCOPE–short form has yet to be tested for Australian use. Furthermore, the authors recommend that the scores on the SCOPE–short form are best used to compare with national averages, rather than aggregated for use as a measure of social inclusion, meaning that Australian norms would need to be established.
Discussion
Interpreting the findings
Our review identified 10 candidate individual-level social inclusion measures. This number is fairly small, particularly considering the vast array of measures that exist for assessing clinical changes. The paucity of measures may reflect the fact that social inclusion has only come on to the agenda for mental health system reform relatively recently. The focus on social inclusion is now gaining momentum because there is acknowledgement that elements of social inclusion, like community participation, underpin good mental health. However, the absence of an agreed definition of social inclusion may still be curtailing the development of relevant measures to some extent, as may the lack of consensus about which life domains are essential to social inclusion (Morgan et al., 2007).
It is noticeable that the available measures have undergone fairly limited psychometric assessment. Some have not been scrutinised at all, and others have undergone testing with respect to one or two properties only. Again, this may in part be due to the fact that the measures are relatively new, so the window of opportunity for testing them is fairly restricted. The lack of clarity about the overarching construct(s) that each measure purports to assess may also have had an impact here (Priebe, 2007). Either way, further psychometric testing of all measures is required.
Our examination identified two measures that show the most potential for further testing in their current form: the APQ-6 and the SCOPE–short form. The APQ-6 has been trialled in the Australian environment. New South Wales is currently well advanced in the process of implementing it as a discretionary component of their local Mental Health Outcomes and Assessment Tool (MH-OAT) collection, and other jurisdictions have expressed interest in the possibility of the APQ-6 being used on a similar basis within their services. The limitation of the APQ-6 is that it does not measure housing, so it would require modification for the purpose under consideration here. The SCOPE–short form assesses the full gamut of social inclusion domains emphasised in the Fourth National Mental Health Plan (Australian Health Ministers, 2009), but might require modification for the Australian context and would certainly need to be tested here. As it is intended for comparison with national norms rather than for use independently as a measure of social inclusion, Australian norms would need to be established.
The current discussion of social inclusion measures acts as a starting point only in identifying a social inclusion measure for routine use. The two that have been identified are not perfect and could not be rolled out without further developmental work. The next steps in this process could involve head-to-head comparisons of the two measures. Further alternatives could be to examine sub-sections of other, longer measures that might be extracted for use for the current purpose, and/or to use some measures as self-report that have not yet been tested using this mode of administration. Such alterations to an existing measure would also require further testing to determine the psychometric properties and usability of the shorter measure.
Consideration should be given to nuances in the domains of social inclusion that the selected measure should assess. Consideration should also be given to how the data generated by a routine measure might be used. For example, if part of the assessment of performance against the indicators of the Fourth National Mental Health Plan (Australian Health Ministers, 2009) were to involve comparison of the degree of social inclusion of people with mental illness and the general population, then the APQ-6 might be given preference over the other measures on the grounds that its objective questions are designed to map directly to the Australian census. Depending on the outcomes of this evaluation process, one or more of the measures might be presented to stakeholders for consultation, perhaps in a modified form.
Limitations
This discussion of social inclusion measures is based only on published literature outlining the development and/or testing of a social inclusion measure. It was beyond the scope of this review to contact directly all corresponding authors responsible for development of the measures to determine if they have any further published work relating to that measure. This might be an important additional step in any future review.
This discussion also only considers the named measures in their existing format and with their recommended mode of administration. Some measures might be suitable for adaptation for the current purpose by using self-report in place of interviews and by selecting the most relevant components of longer measures. While these alterations would then require further testing, it might be an efficient way of developing a suitable standard measure for national use.
This is an initial scope of the current literature relating to social inclusion measures published in the literature and not a systematic review. For this reason, the review was largely conducted by a single researcher and there was no meta-analysis or critical review of the testing procedures used to establish the measures’ credentials. Any decisions regarding use of these measures resulting from this review should keep these limitations in mind.
Conclusion
Social inclusion is too important not to measure properly. As an initial scoping of available candidate measures, this discussion provides a springboard for selecting an appropriate measure for use in public sector mental health services. In their current format, the findings suggests two primary candidates, but neither of these is quite fit-for-purpose in its current form. Further exploration will reveal whether one of these is suitable, whether other measures might be adapted for the current purpose or whether a new, specifically designed measure needs to be developed.
Footnotes
Funding
This work was funded by the Australian Government Department of Health and Ageing.
Declaration of interest
The authors report no conflicts of interest. The authors alone are responsible for the content and writing of the paper.