
Abstract
Introduction
Delusions have been described as phenomena that reflect cognitive processes. Such beliefs are often held despite counter-evidence and rational counter-argument, are often held with great conviction, and are usually not accepted by others living in the social-cultural environment (Gilleen and David, 2005; Langdon and Coltheart, 2000; Miller and Karoni, 1996). In earlier research, delusions were generally not attributed to abnormal reasoning processes (Maher, 1974) and were instead considered to reflect broader pathologies of the mind and brain. However, in more recent research, there is now growing acceptance of the view that inadequacies in reasoning and susceptibilities to information processing biases may also be associated with delusion formation and maintenance (e.g. Garety and Freeman, 1999; McKay et al., 2007; Moritz and Woodward, 2006).
One of the most documented of these is the jumping to conclusions (JTC) bias that involves inadequate or selective consideration of information in making judgments about outcomes or the status of events. The JTC bias is typically considered to have two components. The first relates to what are termed ‘premature decisions’, in which decisions are made based on limited evidence. The second is referred to as ‘over-adjustment’ and involves situations where decisions are radically altered in the face of modest accumulations of disconfirming evidence (Garety et al., 1991). The most commonly employed task to elucidate the JTC bias is the ‘beads task’. First adapted to samples with psychosis by Huq et al. (1988), this task typically consists of two containers each filled with coloured beads. Participants are shown that one jar has, for example, green and red beads in the proportion of 85:15, while the other has the reverse proportion of beads. Participants are instructed that the containers will be removed from sight and that one of the two containers will be selected by the experimenter. Beads will be drawn from this unseen container one at a time and subsequently placed back, upon which another bead is withdrawn. From this sequence of withdrawn beads, participants are asked to decide which container the experimenter had picked, and to make decisions on a bead-per-bead basis. The sequence of beads presented to participants is pre-determined and usually has a fixed order for all participants. For example, participants might be presented with nine red beads (R) and one green bead (G) out of a sequence of 10 beads (i.e. R-R-R-R-G-R-R-R-R-R). The experiment is normally administered in one of two ways: the ‘draws to decision’ procedure, where participants take as many trials as needed to reach a definite decision (i.e. which container the bead sequence is coming from); or the ‘graded estimates’ procedure, where the number of trials is fixed, and for each trial, participants must provide a probability estimate that a particular bead is from one of the two containers (Garety and Freeman, 1999; Moritz and Woodward, 2005).
Careful decision-making is usually withheld until sufficient evidence is obtained. However, participants with delusions typically do not respond in this way. Instead, up to 70% of patients with delusions will often reach a definite decision on which container beads are coming from on the first or second bead (i.e. they make premature decisions). They will also be more likely to over-adjust their hypothesis when faced with potentially disconfirmatory evidence. For example, a person presented with containers consisting of red and green beads (i.e. 90:10 red/green and 10:90 red/green) might witness a long string of red beads and then change his or her opinion when faced with a single green bead (Young and Bentall, 1997; e.g. Garety et al., 1991; Langdon et al., 2008; Moritz and Woodward, 2005; Rodier et al., 2011). These findings have also been replicated using ‘delusion-prone’ samples (e.g. Colbert and Peters, 2002; Van Dael et al., 2006; Warman et al., 2007), providing evidence that the JTC bias may be a precursor to delusion formation.
Although these findings have been accepted as providing evidence of an association between delusion-proneness and suboptimal reasoning strategies, there are a number of concerns that have emerged relating to the interpretation of these findings, particularly in relation to the ‘over-adjustment’ phenomenon. The first concern is that this component of the bias could be considered inconsistent with one of the defining characteristics of delusions; namely, that they are resistant to counter-evidence. The ‘over-adjustment’ effect instead predicts that individuals with delusions are particularly responsive to disconfirmatory evidence. ‘Over-adjustment’ also appears to be an effect limited to the beads task itself, as it contrasts with another set of findings which suggest that individuals with delusions are actually more likely to ignore or downplay the importance of disconfirmatory evidence when compared with healthy controls (i.e. ‘bias against disconfirmatory evidence’, BADE) (Buchy et al., 2007; Woodward et al., 2006). Furthermore, a recent meta-analysis suggested that the ‘over-adjustment’ bias is not always replicated within the literature, and may not even be associated with delusions (Fine et al., 2007).
As a result of these conceptual difficulties, some suspicion has arisen as to whether another factor may account for the over-adjustment effect. One suggestion, for example, is that it may be due to an artefact of the beads task (Balzan et al., in press; Moritz and Woodward, 2005); in particular, the possibility that participants may have misinterpreted or forgotten the basic principle of the task, which was that beads were only coming from one container rather than both. Consequently, participants in these studies may have incorrectly assumed that containers swap throughout the task (e.g. red beads must always come from the mostly red container, while all green beads must come from the mostly green container), or equivalently, that they were expected to consider each bead separately rather than all information in the entire series of beads. Such ‘miscomprehension’ of the task instructions may therefore account for the erratic decision-changing behaviour traditionally labelled as ‘over-adjustment’, as participants may simply be responding to the current bead (i.e. red beads = red container) and not the bead sequence. In sum, miscomprehension rather than delusional ideation may be driving the over-adjustment effect.
This possibility of miscomprehension was first proposed by Moritz and Woodward (2005) and was defined by a participant selecting the opposite container to the one which was expected (e.g. judging beads were coming from the container with 90% green beads–10% red beads, when the sequence of 10 beads only contained one green bead and nine red beads). The results of this study indicated that 52% of the schizophrenia sample and 23% of the healthy controls made illogical responses congruent with the miscomprehension style of responding. Moreover, participants exhibiting a JTC bias were significantly more likely to apparently fail to comprehend the task.
Speechley et al. (2010) further explored this issue by attempting to reduce the risk of participants not comprehending the task. This was done by devising a presumably more realistic ‘fish/lakes’ stimuli set rather than the typical abstract beads/containers set. Additionally, four of the six series of tasks incorporated 10 fish of the same colour (‘uniform’ condition) rather than the usual alternating pattern of coloured beads/fish (‘alternate’ condition), which may have helped participants understand that only one lake was being drawn from and not both lakes (i.e. one colour implies one lake). Finally, the task included two 10-point rating scales (very unlikely to very likely) for each of the two ‘lakes’, as it was argued that a single rating scale results in a loss of information, such that it is impossible to know whether a movement in one direction (e.g. a downward rating adjustment) for one option is accompanied by a simultaneous and reciprocal rating in the opposite direction for the other option. The results were therefore able to show how people reacted to both ‘matching lakes’ (i.e. a lake with a higher ratio of fish the same colour as the current fish) and ‘non-matching lakes’ (i.e. a lake with a low ratio of fish the same colour as the current fish).
One aspect of the results showed that participants appeared to be considering each fish separately rather than using all information in the entire series of beads and using Bayesian reasoning strategies (see Speechley et al., 2010; Figure 6). Other aspects of the results showed that, within the ‘uniform colour’ condition, where miscomprehension could effectively be ruled out, participants with active delusions still rated ‘matching lakes’ significantly higher earlier in the sequence than all non-delusion groups, thereby validating the ‘premature decisions’ effect. However, there were no differences between delusional and non-delusional groups for ‘non-matching lakes’, whether the trials of fish were of ‘uniform’ colour or were ‘alternating’. Accordingly, the authors concluded that JTC-premature decisions are better thought of as a hypersalience of positive matches between the evidence and hypothesis, as the non-matching lakes were not rated any lower by the delusional participants compared to controls. This finding also suggests that the ‘JTC-over-adjustment’ findings are not over-reactions to disconfirming evidence in the ‘alternating’ condition. Rather, the ‘over-adjustment’ may represent a hypersalience of positive matches between the evidence and hypothesis when instructions are misunderstood (i.e. containers/lakes are ‘swapping’).
However, neither of these studies provided any direct qualitative evidence to suggest that ‘miscomprehension’ was actually occurring during the task. Moreover, ‘miscomprehension’ was removed only from the ‘uniform sequence’ condition in the above study, yet to fully determine any influence it has over ‘over-adjustment’, it would also need to be removed from an ‘alternating sequence’ condition. Indeed, if miscomprehension is driving JTC-over-adjustment, the absence of miscomprehension should lead to significant reductions in levels of this phenomenon.
In an attempt to gather qualitative evidence of miscomprehension, a recent replication of the Moritz and Woodward (2005) study asked 92 non-clinical participants (identified as either delusion-prone or non-delusion-prone, as determined by the Peters et al. Delusions Inventory; Peters et al., 1999) to justify their response upon presentation of the ‘disconfirmatory bead’ in the sequence (Balzan et al., in press). It was hoped that this would determine if miscomprehending participants actually thought the containers had been swapped at this point in the sequence. Overall, 25% of the sample demonstrated a JTC bias, and just over half made illogical responses consistent with a failure to comprehend the task. Importantly, qualitative evidence of miscomprehension revealed that these ‘illogical responses’ were being driven by a misunderstanding of task instructions (i.e. non-comprehending participants thought the containers had swapped at the contrasting bead colour). The lack of a clinical sample within this study, however, limits the interpretability of these results. Moreover, to-date, no studies have successfully removed miscomprehension from an ‘alternating sequence’.
To determine the validity of the ‘over-adjustment’ component, therefore, miscomprehension would need to be removed from an ‘alternating’ sequence, and this would need to be confirmed by qualitative evidence that containers were not perceived to be exchanged during the presentation of disconfirming evidence. These issues were addressed in the present study which utilised two versions of the traditional beads task and three participant groups: (1) a clinical schizophrenia group, (2) a non-clinical delusion-prone group, and (3) a group of healthy controls. The first task was an unaltered replication of the task used in the Moritz and Woodward (2005) study. The second version was modified such that participants were explicitly instructed that ‘beads always come from the same container’ and that ‘containers do not swap at any point’. Participants were also instructed that it is more logical, considering the available evidence, to down-rate confidence for a particular container in the face of ‘disconfirming evidence’ rather than jump between containers.
Based on previous evidence, it was hypothesised that the schizophrenia and delusion-prone groups would show higher levels of ‘premature decisions’ and ‘over-adjustment’ relative to controls, and if these phenomena represent a genuine characteristic of decision-making in these populations, the effect should persist following clearer instructions during the second task. Conversely, it was hypothesised that, if miscomprehension is indeed a major explanation for ‘over-adjustment’, then one would observe significant decreases in responding consistent with this effect in the second task, where comprehension is expected to improve.
Methods
Participants
A total of 75 participants were recruited, consisting of 50 non-clinical participants (23 males; 27 females), who were further divided into delusion-prone and non-delusion-prone groups as determined by the PDI-21 (Peters et al., 2004) and 25 clinical participants (15 males and 10 females; 23 outpatients and two inpatients) with a diagnosis of schizophrenia and a history of delusions. The diagnosis of schizophrenia was confirmed with the Mini-International Neuropsychiatric Interview (MINI), and the Positive and Negative Symptoms Scale (PANSS; Kay et al., 1987) was employed to determine the severity of current positive symptoms. Both of these instruments were assessed by a trained and experienced research nurse. All clinical participants were being treated with atypical antipsychotic medications at the time of testing.
Non-clinical participants were drawn from hospital staff and the general population via advertisement and word-of-mouth. These participants were screened with the MINI to rule out brain damage and mental illness as confounding factors.
All participants were fluent in English and were able to complete both tasks. Premorbid intelligence estimates were made with the NART (Nelson and Willison, 1991), and working memory was assessed with the Wechsler Adult Intelligence Scale–Revised Digits Forward and Backward subtests (Wechsler, 1997). All attempts were made to ensure clinical and non-clinical groups were matched on social and educational grounds, and socio-economic status was estimated using the Hollingshead Two-Factor Index of Social Position (Hollingshead, 1957) using highest parental occupation and education level. Scores for these measures and all other demographic information for each group are summarised in Table 1. As indicated in Table 1, the three samples were generally well matched in relation to their age, educational attainment and scores on standardised measures of cognitive and intellectual functioning.
Socio-demographic and psychopathological characteristics of participants.
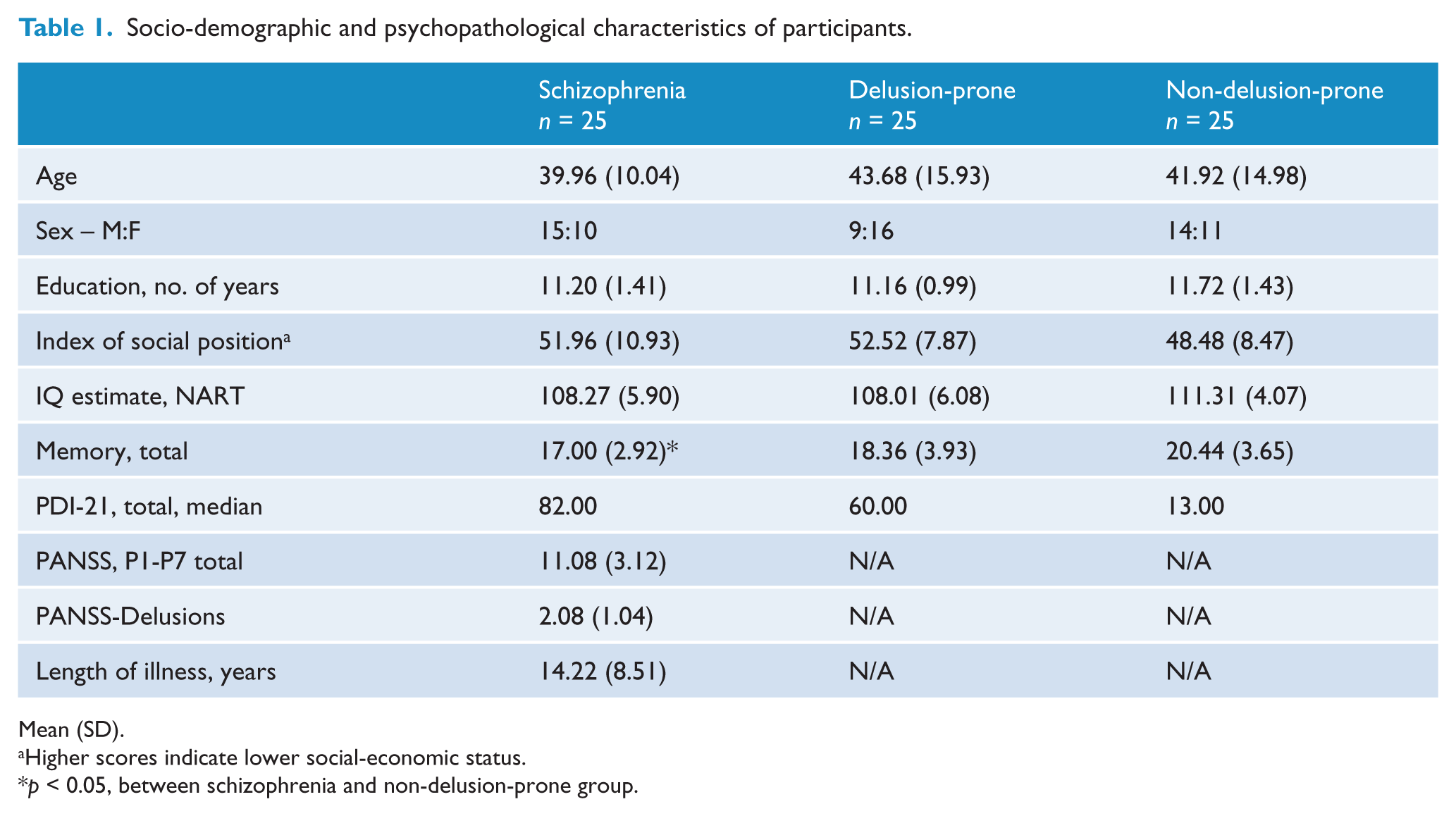
Mean (SD).
Higher scores indicate lower social-economic status.
p < 0.05, between schizophrenia and non-delusion-prone group.
Materials and procedure
Participants were presented with two computerised versions of the beads task, both adapted from the Moritz and Woodward (2005) ‘graded estimates’ procedure. In Task 1, participants were presented with a picture of two containers full of red and green beads (90% red [R] and 10% green [G] for Container A, and vice-versa for Container B). They were told that the computer would randomly select beads from the same container for the duration of the task (i.e. only one container). The sequence of 10 beads was, however, predetermined, and was presented in the following order: R-R-R-R-G-R-R-R-R-R.
After each trial, participants were asked to select from one of the following seven options (by pressing keys 1–7 on the keyboard): 1 = beads are definitely from Container A; 2 = beads very likely from Container A; 3 = beads probably from Container A; 4 = No estimate possible yet; 5 = beads probably from Container B; 6 = beads very likely from Container B; 7 = beads definitely from Container B. This rating scale was displayed for the duration of the experiment, as was the explicit instruction that estimates/decisions should be carried out when considering each bead drawn in turn. To ensure participants remembered the proportion of beads in each container, pictures of the containers also remained displayed for the duration of the task. Participants were then shown a demonstration of a trial, and were given the opportunity to clarify any questions before the task begun. Participants were said to have demonstrated a JTC bias if they gave a definite rating (i.e. 1 or 7) when presented with the first bead that was drawn.
Task 2 followed a similar procedure using blue and yellow beads with a 90:10 ratio, and a bead sequence of nine yellow beads and one blue bead in the middle of the sequence (i.e. implicating the yellow container). However, this task included extra instructions which were intended to make it clearer that containers did not swap during the task, even if participants had thought containers swapped during the first task. To solidify this concept, participants were reminded that, in addition to changing containers completely upon presentation of a contrasting bead colour, they also had the option of changing their confidence within the same container (e.g. from ‘very likely’ to ‘probably’). Participants were also informed that they were free to change their minds about which container the bead sequence was coming from (e.g. A to B), but that this should be done only if presented with sufficient evidence to warrant this (e.g. a string of yellow beads followed by a larger string of blue beads). This intervention was expected to improve levels of comprehension.
Measures
The various measures that were employed in the study included:
(a) JTC-premature decisions – a participant was identified as displaying this aspect of the JTC bias if they made a definite decision after only one bead.
(b) JTC-over-adjustment – represented the amount of change in the judgement-ratings between trials with potentially disconfirmatory evidence (i.e. when beads changed from red to green/vice-versa in Task 1 and from yellow to blue/vice-versa for Task 2).
(c) Miscomprehension – or ‘extreme over-adjustment’, was defined as selecting the opposite container to the one which was being suggested; that is, if participants made an estimate that beads were coming from Container B (i.e. ratings 5–7), where the sequence was clearly indicating Container A (Moritz and Woodward, 2005).
(d) Qualitative measure of miscomprehension – to confirm that ‘miscomprehension’ was a valid measure, participants were informed that should they alter their confidence ratings and/or change containers throughout the task; they were to state aloud why they had done so. Responses consistent with the notion that containers were swapping or had swapped at the contrasting bead were recorded.
Results
The results are divided into two main sections. The first examines the influence of delusional ideation (i.e. schizophrenia; delusion-prone; non-delusion-prone groups) on ‘JTC-premature decisions’, ‘JTC-over-adjustment’ and miscomprehension during Task 1. The impact miscomprehension itself had on both components of the JTC bias is also assessed for Task 1. The second section examines the effectiveness of the Task 2 intervention at reducing the JTC bias and/or miscomprehension while also testing for group differences in JTC bias components.
Qualitative data were analysed by examining the explanations provided by participants displaying evidence of miscomprehension. As anticipated, this analysis showed that all of these participants incorrectly assumed that containers ‘swapped’ when the contrasting bead was displayed (for both tasks). In contrast, no such statements were reported by comprehending participants.
Task 1 – Pre-intervention
(a) Delusional ideation: JTC-premature decisions
As indicated in Table 2, ‘JTC-premature decisions’ (i.e. a definite rating after only one bead) was relatively high for the schizophrenia group, with nearly 70% of this group responding in this way, compared to 32% and 12% of the delusion-prone and non-delusion-prone groups, respectively. A chi-squared analysis confirmed that there was a significant association between group membership and this phenomenon (χ2 (2, N = 75) = 17.21, p < 0.001). Further 2 × 2 analyses confirmed associations between the schizophrenia and delusion-prone group (χ2 (1, N = 50) = 6.48, p < 0.05) and the schizophrenia and non-delusion-prone group (χ2 (1, N = 50) = 16.33, p < 0.001). On the other hand, there was no significant association between group and premature decision-making when the delusion-prone and non-delusion prone groups were compared (χ2 (1, N = 50) = 2.91, p > 0.05).
JTC-premature decisions (n), JTC-over-adjustment, and miscomprehension (n) by delusional ideation for Task 1 and Task 2.
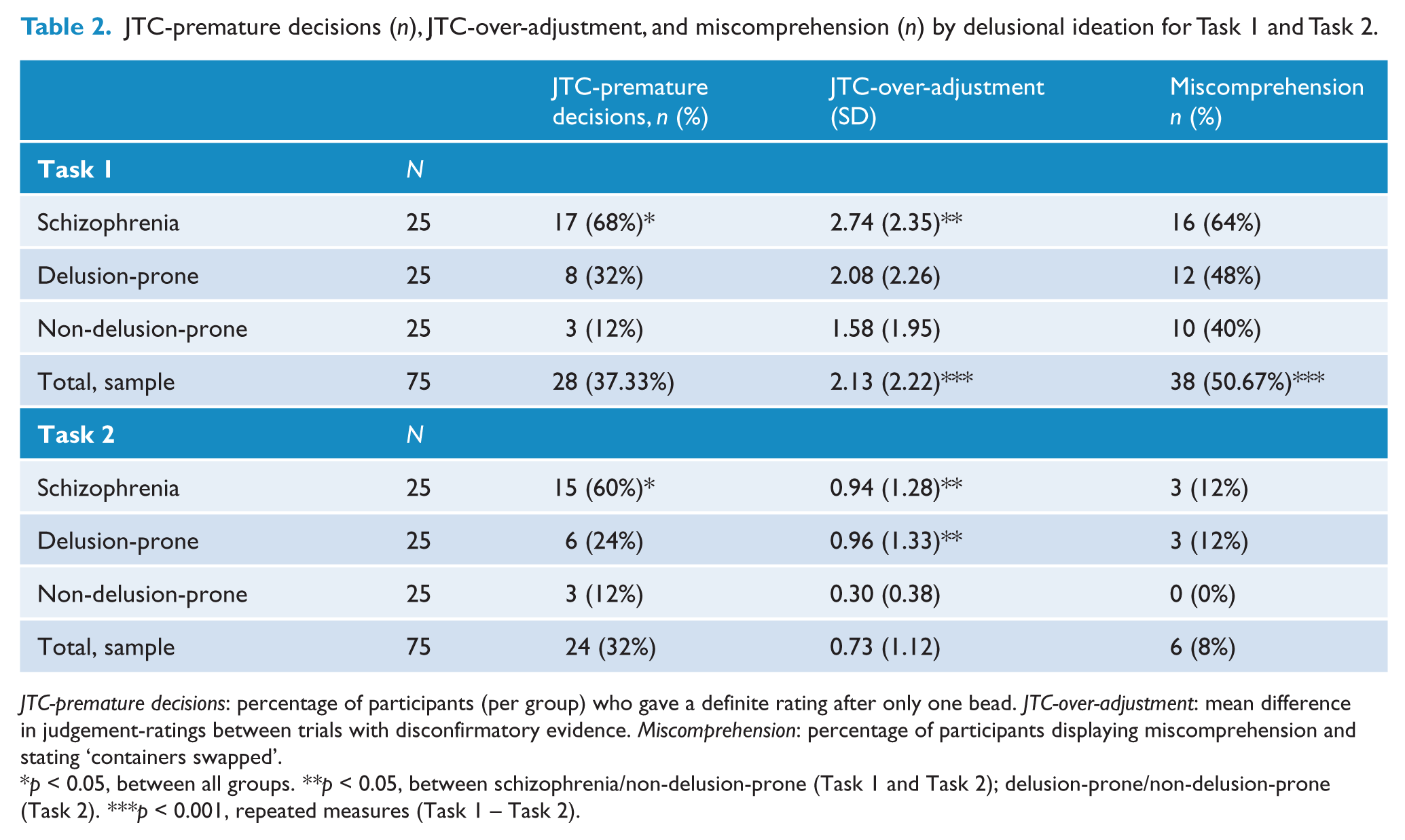
JTC-premature decisions: percentage of participants (per group) who gave a definite rating after only one bead. JTC-over-adjustment: mean difference in judgement-ratings between trials with disconfirmatory evidence. Miscomprehension: percentage of participants displaying miscomprehension and stating ‘containers swapped’.
p < 0.05, between all groups. **p < 0.05, between schizophrenia/non-delusion-prone (Task 1 and Task 2); delusion-prone/non-delusion-prone (Task 2). ***p < 0.001, repeated measures (Task 1 – Task 2).
(b) Delusional ideation: JTC-over-adjustment and miscomprehension
[Note: an anonymous reviewer suggested that these data could also have been combined in a 3 (group) × 2 (task) ANOVA with repeated measures on task for JTC-over-adjustment to test for a possible interaction effect. However, the results from this analysis did not yield a significant interaction for group x task (F(2, 72) = 0.88, p > 0.05).]
In line with previous findings, a planned comparisons t-test between schizophrenia and non-delusion-prone groups revealed that over-adjustment was significantly higher within the schizophrenia sample (t(48) = 1.90, p < 0.05 (1-tailed)). Schizophrenia/delusion-prone and delusion-prone/non-delusion-prone planned comparisons did not yield significant differences (t(48) = 1.01, p > 0.05 (1-tailed); t(48) = 0.84, p > 0.05 (1-tailed)). Furthermore, there was no significant association between group membership and miscomprehension (χ2 (2, N = 75) = 2.99, p > 0.05), although there was a trend for the schizophrenia and delusion-prone groups to exhibit higher proportions of miscomprehension (Table 2). These findings are not, however, necessarily inconsistent with the view that the JTC-over-adjustment effect is influenced by miscomprehension. In fact, they are consistent with the view that although all groups display high levels of miscomprehension, patients with schizophrenia display higher levels of ‘over-adjustment’ due to a hypersalience of evidence-hypothesis matches. That is, when it is assumed that ‘containers have swapped’, the same evidence-hypothesis hypersalience that caused the initial ‘premature decision’ (e.g. red bead = red container) now leads to a ‘premature decision’ in the other container (i.e. green bead = green container). This issue is explored in more detail below.
(c) Task comprehension: JTC-premature decisions
Table 3 indicates that participants who miscomprehended the task were more likely to make ‘premature decisions’ as compared with comprehending participants (52.6% and 21.6%, respectively): χ2 (1, N = 75) = 7.71, p < 0.05. In fact, over 70% of those who displayed this component of the bias misunderstood the instruction that containers do not swap.
JTC-premature decisions (%) and JTC-over-estimation by miscomprehension for Task 1.
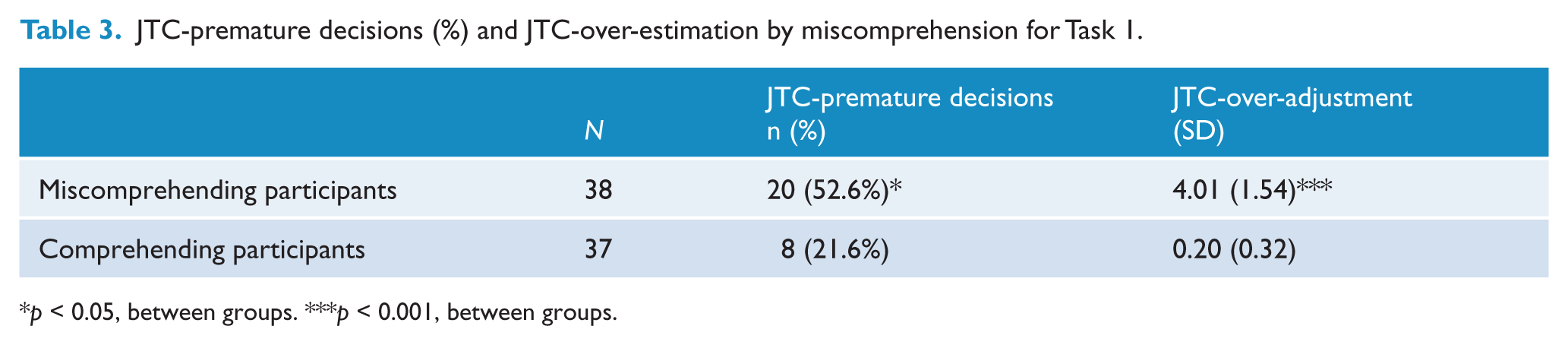
p < 0.05, between groups. ***p < 0.001, between groups.
(d) Task comprehension: JTC-over-adjustment
As shown in Table 3, miscomprehending participants in Task 1 were significantly more likely to over-adjust their responses in the face of potentially disconfirmatory evidence, t(73) = 14.74, p < 0.001. Thus, there was evidence that over- adjustment as well as premature decision-making may be influenced by miscomprehension of the task.
Task 2 – Post-intervention
As indicated above, the aim of the second part of the study was to examine whether the inclusion of an intervention, designed to improve comprehension, would influence the levels of the JTC bias.
(a) JTC-over-adjustment and miscomprehension
A Wilcoxon signed-rank test showed that the inclusion of extra instructions highlighting the fact that containers do not swap at any time during the task significantly reduced the levels of task miscomprehension (Z = −5.66, p < 0.001). A paired samples t-test further revealed significant decreases in the amount of ‘over-adjustment’ from Task 1 to Task 2: t(74) = 6.40, p < 0.001 (Table 2).
(b) JTC-premature decisions
The observed decrease in premature decision-making due to the intervention was not, however, found to be statistically significant (Wilcoxon signed-rank test, Z = −1.16, p > 0.05), which suggests that this phenomenon still remains despite the provision of additional information.
(c) Delusional ideation: JTC-premature decisions
As in Task 1, a significant association was found between group membership and premature decision-making (χ2 (2, N = 75) = 14.34, p < 0.001). Once again, participants with schizophrenia were more likely to display this component of the JTC bias than the other two groups (delusion-prone: χ2 (1, N = 50) = 6.65, p < 0.05; non-delusion-prone: χ2 (1, N = 50) = 12.50, p < 0.001), despite the intervention. No statistically significant association was found between group membership and premature decision-making when the analysis was confined to the two non-clinical groups (χ2 (1, N = 50) = 1.22, p > 0.05).
(d) Delusional ideation: JTC-over-adjustment and miscomprehension
As with Task 1, the planned comparisons for Task 2 showed significant group differences between the schizophrenia and non-delusion-prone groups (t(48) = 2.39, p < 0.05 (1-tailed)) and the delusion-prone and non-delusion-prone groups (t(48) = 2.40, p < 0.05 (1-tailed)). It is worth noting, however, that the ‘over-adjustment’ levels for the schizophrenia group during Task 2 were much lower than even the non-delusion-prone group during Task 1. No differences in ‘over-adjustment’ were found between the schizophrenia and delusion-prone group (t(48) < 1), or between groups in the likelihood of miscomprehending the task (χ2 (2, N = 75) = 3.26, p > 0.05).
Discussion
The aim of the present study was to determine the validity of the miscomprehension construct, and to examine the extent to which people’s susceptibility to the ‘over-adjustment’ component of the JTC bias are influenced by miscomprehension of the task. The results indeed lend support to the notion that miscomprehension is a valid construct and that it appears to be driving the JTC-over-adjustment effect. From qualitative evidence it was clear that all miscomprehending participants (across both tasks) had believed that the containers had been swapped during the course of the task. Levels of miscomprehension were high, even amongst healthy controls, questioning the continued use of the task in its unmodified form.
Moreover, as hypothesised, the intervention was shown to be effective at reducing levels of miscomprehension during Task 2, despite the fact that this task consisted of an ‘alternating’ sequence. In Task 2, the level of ‘over-adjustment’ dropped significantly, which suggests that, in the absence of miscomprehension (or the notion that containers are swapping), participants no longer ‘over-correct’ their judgements in response to the ‘disconfirmatory evidence’. Although the schizophrenia group did exhibit significantly higher levels of ‘over-adjustment’ relative to the non-delusion-prone group during Task 1, this does not imply patients with schizophrenia over-react to disconfirming evidence in the ‘alternating’ condition, as has been previously suggested.
As the present findings confirm the validity of miscomprehension, the ‘hypersalience of evidence-hypothesis matches’ account put forward by Speechley et al. (2010) may offer a better explanation of the effect. When instructions are misunderstood at the contrasting bead (i.e. containers ‘swapping’), it would appear that patients with schizophrenia are particularly hypersalient to the apparent ‘match’ between the ‘new bead’ (i.e. the ‘evidence’) and the notion that they are now coming from the ‘other container’ (i.e. the ‘hypothesis’), such that ‘a green bead must imply the green container’. As will be explained in more detail below, this account of the JTC bias may also represent the cognitive mechanism underlying the ‘premature decisions’ phenomenon. Furthermore, the finding that both the schizophrenia and delusion-prone groups exhibited significantly higher levels of ‘over-adjustment’ at Task 2, should not be taken as evidence of ‘over-adjustment’ in the absence of miscomprehension. The levels of ‘over-adjustment’ were substantially lower at Task 2 (i.e. the schizophrenia group had levels lower at Task 2 than those exhibited by the non-delusion-group during Task 1), which can be explained by the significant improvement in task comprehension. The significant proportional differences observed here do not so much represent ‘over-adjustment’ per se, but rather ‘modest adjustment’, which itself may be a reflection of ‘modest miscomprehension’, which prevailed for a minority of the schizophrenia and delusion-prone groups (Table 2).
JTC-over-adjustment has been considered a valid construct and a factor in the development and maintenance of delusions since it was first reported in Garety et al. (1991). The present findings, which equate the construct to a misinterpretation of the beads task’s instructional set, challenge this view. The JTC-over-adjustment finding was not originally expected; participants with delusions were instead hypothesised to downplay the importance of the disconfirmatory evidence (Garety et al., 1991) in line with the definition of delusions that they are maintained with great conviction despite counterevidence or counterargument. It would seem that in light of the present findings, this discrepancy between the ‘over-adjustment’ effect and a defining characteristic of delusions is now consistent. Moreover, the findings are consistent with the BADE literature (e.g. Woodward et al., 2006), which states that disconfirmatory evidence is ignored or its importance is downplayed in individuals with active delusions and those who are identified as delusion-prone.
Although the findings challenge the interpretation of the JTC-over-adjustment construct, they nonetheless lend further support to the validity of the ‘premature decisions’ component. JTC-premature decisions were significantly higher in the schizophrenia group and there was a non- significant trend of higher levels of the construct within the delusion-prone group compared to non-delusion-prone participants, consistent with the theory that the construct may play a role in the development and maintenance of delusions across the psychosis continuum (Van Os, 2003). Furthermore, despite a significant relationship between miscomprehension and ‘premature decisions’ during Task 1, which has been interpreted as a confound in previous studies (Balzan et al., in press; Moritz and Woodward, 2005), levels of ‘premature decisions’ remained stable across groups in Task 2, where miscomprehension was effectively removed. This offers further evidence that significant differences in levels of JTC-premature decisions can be demonstrated between groups differing in delusional ideation in the absence of miscomprehension (Speechley et al., 2010). Finally, as has already been highlighted, these findings are also consistent with the interpretation that ‘premature decisions’ may represent a hypersalience of hypothesis (e.g. ‘beads coming from red container’) to evidence (‘red bead’) matches. Such hypersalience in turn generates higher confidence, and the ‘premature decisions’ phenomenon is observed.
Although the current study included a number of features to investigate the issue of miscomprehension in different ways (group comparisons and an intervention task), it is important to be mindful of some of the study’s limitations. First, owing to the nature of the study, it was not feasible to counterbalance the order of tasks, so that it is unclear how much of the change in responding across tasks was due to practice effects as opposed to a genuine decrease in JTC responding. A replication of the study could, for example, include a control group to determine whether a repeat of the task leads to changes in performance. Practice effects would not, however, explain why premature decision-making continued to persist in the schizophrenia group whereas the over-correction effect strongly declined following the introduction of additional instructions. Moreover, typical beads task studies have included multiple versions of the task without any indication that either ‘premature decisions’ or ‘over-adjustment’ improve in subsequent tasks. Rather, they appear to remain stable, thereby limiting the influence that ‘practice effects’ potentially had on these findings.
Second, in line with more recent studies (e.g. Speechley et al., 2010), a replication would benefit from collecting a larger sample of highly delusional participants within a schizophrenia sample to disambiguate the contributing effect of active delusions or the schizophrenia diagnosis itself. Moreover, PDI scores for the delusion-prone sample were not as high as other studies (e.g. Warman et al., 2007), which may have contributed to the non-significant differences in ‘premature decisions’ within the non-clinical sample, despite a trend for the delusion-prone subsample to demonstrate higher levels of ‘premature decisions’. A more targeted ‘delusion-prone’ sample could be collected in future research (e.g. spiritualist churches, conspiracy theory groups). Such research should also attempt to gather more evidence for the ‘hypersalience of positive matches between the evidence and hypothesis’ and BADE constructs. Such studies could include ‘confirmation bias’ tasks where the importance of confirmatory and disconfirmatory evidence is simultaneously rated; participants with delusions would be expected to pay particular attention to confirmatory ‘matches’ whilst downplaying disconfirmatory evidence.
In conclusion, the present study has demonstrated the confounding nature of miscomprehension in the beads task, and confirmed the presence of the JTC bias in schizophrenia. The findings question the validity of the JTC-over-adjustment construct, and further question the use of an unmodified version of the beads task in future research. In sum, the present study highlights the importance for experimenters in this area to check that participants actually understand the task before proceeding to ‘jump to conclusions’ about the potential influence a bias may have on the formation and/or maintenance of delusions.
Footnotes
Acknowledgements
The authors wish to thank Bev Hisee for her tireless efforts at recruiting clinical participants for this study.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Declaration of interest
The authors report no conflicts of interest. The authors alone are responsible for the content and writing of the paper.