
Abstract
Objective:
Assisted dying is a contentious and topical issue. Mental disorder is a relevant influence on requests of hastened death. The psychiatry of dying is not a prominent component in the assessment of euthanasia and physician-assisted suicide (PAS) in jurisdictions with liberalised assisted dying laws. The literature on the assessment processes, with particular reference to mental status, involved in euthanasia requests is considered.
Methods:
An experienced palliative medicine specialist and psychiatrist selectively reviewed the recent literature published about the mental health issues involved in euthanasia and PAS.
Results:
Assessments of competency, sustained wish to die prematurely, depressive disorder, demoralisation and ‘unbearable suffering’ in the terminally ill are clinically uncertain and difficult tasks. There is a growing psychiatric and psychological literature on the mental status of the terminally ill. As yet psychiatry does not have the expertise to ‘select’ those whose wish for hastened death is rational, humane and ‘healthy’. Rarely in those societies with liberalised assisted dying laws are psychiatrists involved in the decision-making for individuals requesting early death. This role is fulfilled by non-specialists.
Conclusions:
There remain significant concerns about the accuracy of psychiatric assessment in the terminally ill. Mental processes are more relevant influences on a hastened wish to die than are the physical symptoms of terminal malignant disease. Psychiatric review of persons requesting euthanasia is relevant. It is not obligatory or emphasised in those legislations allowing assisted dying. Psychiatry needs to play a greater role in the assessment processes of euthanasia and PAS.
Introduction
Over recent decades in several jurisdictions, including for a brief period the Northern Territory of Australia, there has been legislation for assisted dying for severe terminal medical illness. Legalised euthanasia and/or physician-assisted suicide (PAS) are currently practised in the Netherlands, Belgium, Estonia, Luxembourg, Albania, Switzerland and the US states of Oregon, Montana and Washington (Field and Curtice, 2009). Assuring mental competency and the exclusion of current psychiatric illness are tasks expected of medical assessors, who are rarely specialist psychiatrists. Ryan (1995) advocated mandatory psychiatric review of persons requesting euthanasia, a view supported by the RANZCP Section of Consultation-Liaison Psychiatry’s Working Group on Euthanasia (1996). This was obligatory in the Northern Territory but is not in the law of the other jurisdictions. Psychiatry needs to play a greater role in the ongoing debates about euthanasia and contribute from the clinical, scientific, and ethical points of view (Naudts et al., 2006).
Euthanasia is the deliberate ending of another person’s life at his or her request. Physician-assisted suicide (PAS) is defined as ‘a doctor intentionally helping a person to commit suicide by providing drugs for self-administration, at the person’s voluntary and competent request’ (Materstvedt et al., 2003). Withholding and withdrawing futile treatments and palliative or terminal sedation are not considered euthanasia (Materstvedt et al., 2003). There are philosophical, religious, medical, financial and political arguments opposing and supporting killing on request. Reports about those countries and states with liberalised assisted dying legislations are becoming available and provide important insights into this practice.
The author has attended an estimated 10,000 terminally ill hospice patients over the last two decades. Clinical practice moulds professional opinion. It is impossible not to be influenced and biased by clinical experience. This article is not a comprehensive review of the literature on assisted dying. It is a selective review of published literature from jurisdictions with assisted dying legislations by a clinician working within a legal system prohibiting euthanasia and PAS, and with an interest in the psychiatric state of the terminally ill.
Over the last 50 years, medicine became scientifically capable of artificially sustaining life. For the first time the very sick have options of living or dying. Assertive oncological treatments, aimed only to prolong life for weeks to months, are allowing cancer patients to live longer. Critical care and emergency medicine are able to salvage persons suffering horrendous injuries and illnesses. The survivors, however, may endure major disabilities including psychiatric disorders. Cancer and AIDS have been converted into chronic illnesses, allowing the accumulation of disease in multiple organs, including the brain. The process of dying is becoming increasingly fraught and difficult. Euthanasia debates do not occur in societies without health services sufficiently affluent to be able to keep persons artificially living (Spence, 2003). The fear of dying ‘badly’ (dysthanasia), rather than a fear of death, is a dominant concern of developed societies. This is a new driver of euthanasia for which modern medicine is responsible. The psychology and psychiatry of dying is becoming increasingly relevant in those individuals whose quality of remaining life is deteriorating and who are experiencing ideations about hastening death.
Legalised PAS and euthanasia
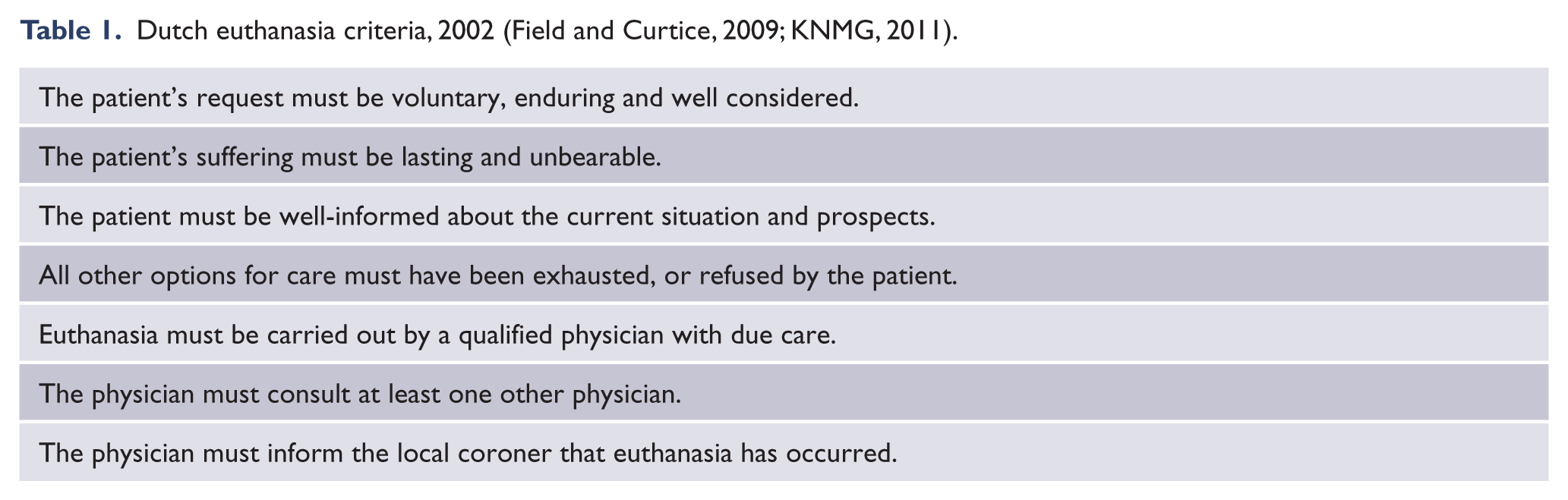
In 1996, for the first time in history, a democratically elected government in the Northern Territory made both euthanasia and PAS legal. The following year the Australian government overturned this territory law. In 9 months, seven patients had made formal use of this law and four died under it. In the Netherlands, euthanasia and PAS have been sanctioned and practised openly since 1991. The Dutch criteria for euthanasia include competency but not the exclusion of mental illness as prerequisites (Table 1) (Field and Curtice, 2009; KNMG, 2011). In 2001, 2.8% of all Dutch deaths were by euthanasia and PAS (van der Heide et al., 2007). This percentage had fallen to 1.8% in 2005 (van der Heide et al., 2007). Of a yearly average of 8400 requests, approximately 2400 are actually carried out (KNMG, 2011). In most cases the estimated shortening of life was rarely more than 1 month (van der Heide et al., 2003). In 1994 the US state of Oregon legalised PAS but not euthanasia. This law was enacted in 1997. Terminally ill persons suffering ‘incurable’ and ‘irreversible’ disease considered to be in the last 6 months of life, who are capable of making a voluntary decision about their health care, understand the information provided, communicate a choice, and not have a mental health condition that impairs judgement, may request PAS. The patient is prescribed a supply of lethal medication (a barbiturate) to be consumed orally. About 50–60 persons/year die of PAS (about 0.2% of all deaths). Between 1998 and 2004 only 326 prescriptions were written, and 208 ended their life this way (36% dying naturally) (Okie, 2005). In 2010, 96 patients were recipients of lethal medication prescriptions and 59 are known to have died ingesting the medications (Oregon Public Health Division, 2010). Similar legislation was passed in Washington in 2008. Since 2010 doctors in Montana are protected from prosecution for helping the terminally ill die, providing the patient is competent. Belgium legalised euthanasia in 2002, but not PAS or any other forms of life-shortening action (Field and Curtice, 2009). Belgium is the only country in which mental suffering from either somatic or mental disorder is explicitly acknowledged in law as a valid basis for euthanasia (Naudts et al., 2006). The mentally ill person must be competent, continuously suffering unbearably, repeatedly express and record a wish to die, and be experiencing a severe and incurable disorder. Euthanasia represented 1.9% of all Flemish deaths in 2007 (Smets et al., 2010). Since 1942 the penal code in Switzerland has not criminalised assisted suicide provided the person who assists is ‘motivated by “unselfish” reasons’ (Field and Curtice, 2009). The Swiss law, when created, did not envisage assisted suicide from a medical perspective (Guillod and Schmidt, 2005). Active euthanasia is illegal. A medical practitioner must assess the patient’s decisional capacity and prescribe the lethal dose. The patient must directly administer the lethal barbiturate to themselves. The person seeking assistance does not have to be terminally ill. They do need to be ‘unbearably suffering’ or ‘unreasonably disabled’, and consistently wish to die. Since 1998 nearly 1000 deaths have occurred under this arrangement including nearly 100 British citizens, for the patient does not need to be a Swiss national (Field and Curtice, 2009; Joffe, 2009). Of 1800 Swiss requests for PAS each year, two-thirds are rejected after screening and half of the remaining die by natural causes, leaving about 300 assisted suicides each year (or 0.45% of deaths in Switzerland) (Hurst and Mauron, 2003). In the UK assisting suicide remains illegal, however encouraging suicide may not necessarily be prosecuted if the assistance is ‘minor, reluctant and wholly motivated by compassion’ (Director of Public Prosecutions, 2010). However the Director of Public Prosecutions (DPP) gives no specific assurance as to how it may respond, emphasising the uncertainty still existing regarding assisted suicide in the UK.
Dutch euthanasia criteria, 2002 (Field and Curtice, 2009; KNMG, 2011).
Requests for assisted dying
It is uncertain how frequent the occurrence of unsanctioned doctor-assisted dying is in countries in which euthanasia is illegal. Even anonymously, few clinicians are prepared to reveal an illegal act. Many relatives (and some doctors) presume an analgesic dose several hours before death caused death, rather than easing pain until the imminent natural death occurred. The classical example of this phenomenon is Dr Schur’s ‘voluntary euthanasia’ of the 83-year-old Sigmund Freud, dying of a jaw malignancy (Schur, 1972).
Public opinion polls suggest over 80% support euthanasia legalisation in the UK (Branthwaite, 2005). In most developed countries a majority of the general population appear supportive. There is however a trend that as an individual moves from the street, to oncology outpatients, and to hospice care, their attitude toward liberalising euthanasia mellows. In the Netherlands 7% of all people whose death is expected request euthanasia preceding their death (Onwuteaka-Philipsen et al., 2010). Having initiated the process, 13% then withdraw (Jansen-van der Weide et al., 2005). About 17% of Oregonians are potentially interested in aid in dying, though only 1–2% actually request it (Ganzini et al., 2008) and 36% provided a lethal prescription die naturally (Okie, 2005). In Canadian palliative care patients 63% believed euthanasia should be legalised, yet only 6% would wish to initiate the request (Wilson et al., 2007). The proximity to the death bed contaminates opinion. This may also apply to medical practitioners. Doctors are less often in favour of actively shortening life than are the general public and nurses (Gielen et al., 2008). Specialities such as palliative care, geriatrics and oncology appear more strongly opposed than intensive care physicians and medical students (Gielen et al., 2008; Marini et al., 2006). The UK House of Lords (2005) summarised doctors’ views as ‘The closer their experience of end-of-life patients, the less sure professionals are about the prospect of a change of the law in favour of euthanasia’.
Requests for euthanasia are not uncommon in medical practice. It is reported that 47% of Australian doctors have received at least one request for euthanasia (Stevens and Hassan, 1994). GPs are the recipients of most requests, palliative medicine physicians probably the least. Patients cared for at home are more inclined to request assistance dying than those in hospital, who are more likely to request non-treatment (Cohen et al., 2007).
Acceptable criteria
It might be reasonable to presume that those requesting a hastened death would be frail and suffering severe (cancer) pain or other unpleasant symptoms. In the Netherlands cancer is the most common diagnosis (74%) of the requesters, 7% have cardiovascular disease, and 5% severe pulmonary disease. However relatively more patients (20%) with motor neurone disease (MND) die due to euthanasia or PAS compared with patients with cancer (5%) or heart failure (0.5%) (Maessen et al., 2010). In 2000/01, 2.9% of the requests for PAS were for psychiatric disease and 4.5% for ‘weary of life’ (Rurup et al., 2005). The major specific reasons for the requests were fear of pain (37%), deteriorating physical status (31%), hopelessness (22%), and dyspnoea (15%) (Marcoux et al., 2005). The most important concerns were non-physical (Marquet et al., 2003). Usually the concerns were multifactorial and included fears of dependence, loss of autonomy, loss of dignity, being a burden on others, and social isolation (Marquet et al., 2003). Loss of control appeared to be a core influencing factor. The personal and social factors were more relevant in encouraging the request than the physical and psychiatric ones (Rietjens et al., 2009). The characteristics of the ‘weary’ patients were old age (average 81 years), ‘reasonable’ health, aloneness, social isolation, and ‘through or tired of living and physically deteriorating’ (Rurup et al., 2005). These discontented citizens request ‘suicide-by-doctor’. In only 20–30% of those who request euthanasia is it performed, though none in the psychiatric group and 1% in the ‘weary’ group (Rurup et al., 2005). Thirty-nine per cent had died before the request could be granted and 38% did not meet the necessary criteria to allow euthanasia (Onwuteaka-Philipsen et al., 2010).
The Oregonian data suggest that patients do not request PAS because of unrelieved physical symptoms, or inadequacy of palliative care services (most are simultaneously enrolled in hospice programmes), and neither are they depressed or socially vulnerable (Ganzini and Back, 2003). They request assisted suicide for psychological and existential reasons: they value control, dread dependence on others, are ready to die, and assess current quality of life as poor (Ganzini and Back, 2003). The most important reasons for their requests concerned loss of control, wishing to die at home, loss of dignity and independence, concerns about future pain, poor quality of life and self-care ability (Ganzini et al., 2009). Significantly the requests did not relate to distressing physical symptoms, financial concerns or poor social support. The concerns were about future worries of declining welfare. The majority who request PAS are in their seventh decade, well educated, middle-class, white, married, with cancer diagnoses, and complaining of loss of enjoyment and quality of life. The poor, the ill-educated, the uninsured and those without access to palliative care are not those who request PAS. In Oregon approximately one in two PAS requests are declined, usually because the patient does not suffer cancer (Ganzini et al., 2000).
Contrary to what may have been predicted (and is perhaps assumed by the general public), people request assisted dying, if they have the legal opportunity to do so, because of psychosocial, and not physical, symptoms.
Psychiatry in PAS jurisdictions
A critical component of the legal requirements introduced for assisted dying is that of the role of the medical profession. Doctors are asked to assess the patient and opine upon prognosis and mental status. In the terminally ill these are not simple and straightforward clinical determinations.
In the Northern Territory the patient under the law had to be certified to be of sound mind and making the decision freely, voluntarily, and after due consideration (Field and Curtice, 2009). A psychiatrist was required to examine the patient and confirm that they were not suffering from a ‘treatable’ clinical depression. Four of the seven patients considered (two died before the law came into effect, one after its repeal) had some symptoms of depression. One, despite current depressive symptoms and a probable sub-therapeutic dose of antidepressant, was considered to be ‘depressed consistent with her medical condition’. The other three to die were considered competent and not depressed. The psychiatric assessment was mandatory, raising concerns regarding cooperation, honesty and trust issues (Kissane et al., 1998). Indeed one patient assessed withheld relevant history. No ongoing assessment or psychiatric treatment was offered or proposed.
In the Netherlands physicians ask for a psychiatric evaluation for patients requesting PAS in only 3% of cases (Ganzini and Lee, 1997). However if a psychiatrist or psychologist has already been involved in a patient’s terminal care it was twice as likely that a request for euthanasia be made (likewise for palliative medicine involvement) (Onwuteaka-Philipsen et al., 2010). This may merely be an indication of case complexity. Since the law change in 2002 the person does not need to be competent when ‘euthanased’. An advance request can be made, which remains valid despite altering health status. In 2005, 20% of cases of euthanasia and PAS went unreported and 0.4% of all deaths were the results of the ending of life without any explicit request by the patient (van der Heide et al., 2007). The Dutch medical fraternity believe that a person can have a death wish and not be clinically depressed (Maessen et al., 2010). To date most requests for those suffering mood disorders have been declined as there were still psychiatric treatment options remaining (Field and Curtice, 2009). Objective criteria assessing suffering are neither available nor indeed possible. How the suffering is determined to be ‘unbearable’ rests upon the impression of the assessing doctor for there is no formal definition of this term (Dees et al., 2010). Ultimately the decision to enact PAS rests on how the doctor considers the patient’s suffering. It could be argued that it is not patients exerting autonomy, but doctors exercising power.
In Oregon if the primary physician believes a psychiatric disorder is present, the patient must be referred to a psychiatrist or psychologist. The limited ability by primary care physicians to detect psychiatric disorder is well recognised. Only 6% of Oregon psychiatrists were confident that on a single consultation they could determine if mental disorder was influencing the request (Ganzini and Lee, 1997). In 2010 only one of the 65 persons who died of PAS had been referred for formal psychiatric or psychological evaluation (Oregon Public Health Division, 2010). Depression (in Oregon) may or may not invalidate a voluntary request, and treatment of depression only improves the desire for life-sustaining therapy in a minority (Ganzini and Lee, 1997; Ganzini et al., 1994). The key task for psychiatry in Belgium is the assessment of capacity. Normally the treating doctor will assess competency, except in those whom the doctor thinks will not die in the foreseeable future (Naudts et al., 2006). A mandatory psychiatric referral then occurs. These are generally those patients with mental illness (and without a terminal illness). Mental disorder does not necessarily imply incompetence and there are no established criteria for determining whether a patient is competent to choose death by suicide.
The current provision of psychiatric assessment, as legislated in these jurisdictions, would appear to be inadequate to perform the difficult tasks expected. Not only is psychiatry rarely consulted, the limited knowledge of the psychiatry of terminal illness raises the probability that the legal expectation of psychiatry is not achievable.
The psychiatry of dying
The prevalence of psychological distress and psychiatric illness in the dying is significant (Macleod, 2011). Affectations of the brain and mind influence judgement and decision making. Most terminally ill people are at times fearful and anxious. Serious emotional turmoil is commonly associated with incapacity (David et al., 2010). At least 15% of terminally ill cancer patients are experiencing major depression (Hotopf et al., 2002), though this prevalence falls as death approaches (Macleod, 2011). A similar number are dysthymic, dysphoric and demoralised (Kissane and Kelly, 2000). Depression in the terminally ill is a complex and difficult diagnosis to make and depressed and demoralised patients are not necessarily competent (Kissane and Kelly, 2000). Delirium is a common, if not inevitable, syndrome during the final phase of a malignant illness. In the terminal phase of life up to 80% become delirious (Lawler et al., 2000).
Assessing capacity in those requesting PAS is difficult as the cognitive capabilities required to decide on rational suicide are contestable. In the Netherlands consent is not invariably given prior to assisted death. Euthanasia without an explicit request from the patient amounted to 0.7% of all deaths in the Netherlands in 2001, and 0.4% in 2005 (van der Heide et al., 2007). There had been discussion about the act, or a previous wish of the patient for the act, in 60% of these patients, as compared to 26% in 2001. Discussions with relatives had occurred in 80% and with colleagues in 65% of these cases, 10% of whom were unconscious at the time of the decision and 14% incompetent owing to young age. Termination of life without request is more common in Belgium, with 1.8% dying without an explicit request (a weighted prevalence) in 2007 (Chambaere et al., 2010). In a sample of 208 deaths under the euthanasia law, representing 12% of the deaths during 2007 in Flanders, 32% were administered life-ending drugs without their explicit request (Chambaere et al., 2010). The decisions to terminate the lives of these elderly, hospitalised patients in comatosed or demented states, who had previously indicated a wish for life not to be needlessly prolonged, were made by medical staff in agreement with the family, usually following a sudden decline in the patient’s health, leaving them unable to communicate.
The accuracy of the figures on euthanasia is complicated by how palliative sedation is defined. Palliative sedation refers to the intentional clinical practice of suppressing consciousness to control refractory symptoms (delirium, pain, dyspnoea, nausea, acute haemorrhage) during the last days or hours of life, in a manner that is ethically acceptable to the patient, family and healthcare providers. When there is no other medical means of relieving an unendurable symptom, sedation may be the humane clinical option. Palliative sedation is not euthanasia; the intent is to relieve suffering, not to kill. In Belgium since 2001 the rate of using continuous and deep sedation until death increased from 8.2% of all deaths in 2001 to 14.5% in 2007 in one study (Bilsen et al., 2009) and fell from 7% in 1999/2000 to 1–2% since 2001 in another (Broeckaert et al., 2011). In the study by Chambaere et al. (2010), opioids were used for sedation in 83% of the cases (often as the sole agent). This suggests a very broad definition of palliative sedation. There is solid evidence that the dose of opioid and its rate of increase do not influence survival at the end of life (Good et al., 2005), and indeed indications are that the duration of life is actually prolonged by palliative sedation. Appropriate opioid, neuroleptic and benzodiazepine prescribing does not constitute the use of ‘life-ending drugs’. Barbiturate administration, however, does. Palliative sedation and the doctrine of double effect are issues potentially able to be manipulated by advocates and/or critics of assisted dying. In the Netherlands in 2001, 5.6% of deaths involved the practice of ‘continuous deep sedation’, and in 2005 this figure was 7.1% (van der Heide et al., 2007). In palliative care settings worldwide about 25% of dying patients receive palliative sedation (Macleod, 2011).
It is claimed that there is no evidence from the Netherlands or Oregon to justify concerns about the negative impact of assisted dying legislation on potentially vulnerable groups, such as older, uninsured, ethnic minorities, minors and disabled people (Norwood et al., 2009). The only group identified to have a heightened risk were people with AIDS (Battin et al., 2007). While in the Netherlands it is more likely to talk about euthanasia than to die a euthanasia death (Norwood et al., 2009), as yet there is no compelling information from countries allowing assisted death that competency and consent issues are rigorously adhered to.
High desire to die is present in up to 17% of the palliative care population (Nissim et al., 2009). In severely ill patients, the will to live fluctuates (Cochinov et al., 1995). The will to live is determined more strongly by psychological variables until the last few days, when it is supplanted by physical variables such as pain and dyspnoea (Cochinov et al., 1999). In terminally ill cancer patients, psychological distress rather than pain and functional status is the most influential factor determining the desire for hastened death (Mystakidou et al., 2005). The strongest factors are hopelessness, depression and anxiety (Mystakidou et al., 2005). The wish to die is not stable, especially if mental health problems are evident (Ganzini et al., 2000). Major depression was diagnosed in 59% of hospice patients who persistently desired a hastened death, but in only 8% of those who did not (Cochinov et al., 1995).
In Oregon it is estimated that about 20% of those requesting aid for dying are depressed (Ganzini et al., 2000, 2008), an expected incidence. Concerned that the professionals and family members involved with Oregon patients who pursued assisted dying did not believe depression had influenced their choice, and that in 2007 none of those who died of PAS had been seen by a psychiatrist or psychologist, investigators studied the prevalence of depression and anxiety in terminally ill people requesting aid in dying (Ganzini et al., 2008). Although the investigators struggled to recruit subjects, of 58 Oregonians 15 met the criteria for depression (HADS and Beck, SCID-I), six of whom being of the opinion that their depression influenced their preference for PAS. By the end of the study 42 had died, of whom 18 had been prescribed a lethal dose, and nine had died by this method. Three (17%) of these 18 decedents had met the criteria for depression, though one had been successfully treated for depression before her death. It would appear that some cases of depression are missed or overlooked in the medical assessments. Elevated prevalence of depression has been determined in Swiss people seeking assistance to die. The largest right-to-die organisation in Switzerland (Exit) found 27% of those requesting assisted suicide were ‘depressed’ according to their volunteer assistants (Bosshard et al., 2008), and 36% of hospitalised palliative care patients demanding death were depressed (Moynier-Vantieghem et al., 2010). However in neither of these studies was depression diagnosed according to accepted research criteria.
Those Oregonians who received substantive intervention such as control of pain, hospice referral, psychosocial and antidepressant medication, were more likely to change their mind about PAS. They also had less advanced disease. Eleven per cent had a change of mind after an antidepressant trial. Those whose decision altered were more ambivalent and unstable with regard to the initial request, not as hopeless, and had a few treatment options still available (Ganzini et al., 2000). In Oregon, no PAS patient has contacted emergency services after consuming the lethal medication, though this would need to be done within 25 minutes (Okie, 2005). In the Netherlands 13% had a change of mind (Jansen-van der Weide et al., 2005). This was less likely in the terminal phase and more likely if there were mental health problems. Instability of attitude concerning PAS, generally toward rejection of an earlier supportive view, occurred in 8–26% of non-terminally ill hospitalised elderly American patients, particularly if depression lifted (Blank et al., 2001). A study of depressed geriatric patients’ preference for life-sustaining therapy found that 25% showed an increased desire for such therapy after treatment for their depression (Ganzini et al., 1994). In AIDS patients with desire for hastened death, 27% of whom had major depressive illness, those who responded well to antidepressant treatment after 2 months dramatically reduced their wish for an early death (Breitbart et al., 2010). The 37% of patients whose depression did not respond had no major alteration in their desire to die early. Depression does not inevitably account for desire for death but there is a possibility that treatment of depression may alter significantly the incidence of PAS requests. Existential variables may have a stronger effect on the desire to die than psychological and psychiatric ones (Cochinov et al., 2005). The desire for death may be driven by the intolerable future rather than the intolerable present (Sullivan, 2005). Spiritual well-being (a sense of meaning and peace) is an important modifier of the desire to die, and even if depressed, it is protective (McClain-Jacobson et al., 2004). The percentages of patients changing their view about PAS, perhaps 10–15%, whilst small, would be considered to be an unacceptably high operating mortality in surgical practice. Of additional concern is the clinical impression that by offering further treatment options (such as chemotherapy for the cancer patient), the patient’s view about euthanasia may alter. This underlines the fickleness of hastened death ideation.
Suicidal thoughts occur in as many as 45% of terminally ill patients, though these are usually fleeting and often associated with feelings of loss of control and anxiety about the future (Bloch, 2000). The frequency of completed suicide in the cancer population is about twice that in the general population (Misono et al., 2008), with the highest risk in the months after diagnosis (Crocetti et al., 1998). Suicide is the cause of death in less than 1% of the cancer population and the risk is very low in the terminal phase (Nissim et al., 2009; Ripamonti et al., 1999). ‘Psychological autopsy’ studies suggest that 80% of persons with cancer who committed suicide were clinically depressed, about the same as for those suicides without cancer (Henrikson et al., 1995). Relatively few terminally ill patients kill themselves, yet some wish to be killed by their doctor. Finlay (2003) suggests that suicide and euthanasia are driven by fundamentally different needs, the former by depressive illness, the latter by a desperate way to gain the last vestige of control over a situation. Historically society has viewed suicide as a mortal sin, a criminal offence, a mental illness, and since the 1970s Western society has started to consider suicide as a calculable category of risk (McManus, 2005). Identifying and attending to these risk factors, thereby preventing suicide, has become a major public health issue. To dissuade the general community from committing suicide, and yet allow it in specific instances, risks complicating suicide prevention education.
Conversations about dying, death and suicide are important components of the practices of palliative medicine and psychiatry. For some ‘euthanasia talks’ (the negotiations around the request and the process) are in themselves apparently therapeutic. Euthanasia practice in the Netherlands typically involves extensive deliberations with the patient, the majority of which do not end in a euthanasia death (Norwood et al., 2009). Paradoxically, these discussions tend to affirm social bonds, social life and life. This is consistent with the findings that advance care planning can positively enhance rather than diminish patients’ hope (Davison and Simpson, 2006). The provision of a ‘lethal bullet’ may result psychologically in an enhancement of the patient’s control over their desperate predicament, an improvement of their esteem and a reinvigorated wish to live until nature determines otherwise. Referring to Oregonians who decide not to ingest the prescribed barbiturate, Quill (2005) commented that: ‘Perhaps the knowledge that they could end their life if they so desired makes them feel less trapped – therefore freer to keep going’. It may be that a planned and orchestrated death, and the avoidance of an uncomfortable death-bed vigil, may facilitate less traumatic grief reactions for family and friends (Swarte et al., 2003). However most working in palliative care observe the helping and healing dynamics of families during those final days, but there is no doubt that some individuals and families may prefer ordered and sanitised death.
Assisting dying
Doctors may buckle with the psychological issues associated with their dying patient. The fatigued, hopeless and despairing doctor confronted by a patient requesting assisted suicide may more easily acquiesce or subtly encourage the act. Clinicians burdened with the care of the very sick, who are frustrated by therapeutic impotency, struggling to communicate effectively, and seduced by the apparent rationality of the request, may become, like their patient, supportive and implicit in quickening death (Kelly et al., 2003).
Killing patients is a role most doctors appear neither to wish nor want. It may be, not surprisingly, distressing for the practitioner. In the 1990s 75% of Dutch doctors expressed feelings of discomfort following euthanasia, 58% following assisted suicide, and 34% following life ending without an explicit consent (Haverkate et al., 2001): ‘Many physicians who had practiced euthanasia (in the Netherlands) mentioned that they would be most reluctant to do so again’ (van der Maas et al., 1991). In Oregon doctors attending persons requesting PAS report being intimidated by patients to assist, and of being powerless to influence the decision-making process (Stevens, 2006). In the USA 53% of physicians who reported participating in euthanasia or PAS were comforted from having helped the patient, 24% regretted being involved and 16% reported that the emotional burden of performing euthanasia or PAS had adversely affected their medical practice (Emanuel et al., 1998). Oregon doctors who had participated, particularly those involved in the early years, acknowledged the difficulties it aroused emotionally. They consider themselves insufficiently prepared, fearful of making errors, and being personally damaged by the experience (Dobscha et al., 2004). It appears that the personal and professional experience of therapeutically killing is discouraging doctors from accepting these patients onto their books and they are withdrawing from the process. For their own self-protection some doctors in the Netherlands apparently attempt to avoid involvement in euthanasia cases (Stevens, 2006).
Euthanasia and psychiatry
Relatively rarely do patients request assisted dying in jurisdictions in which it is legal. If they do so the clinical problems initiating the request are psychosocial and existential rather than medical. There are psychiatric concerns about euthanasia and PAS, yet psychiatry is infrequently consulted and involved in the decision-making processes. Literature from countries and states with liberalised assisted dying laws and the palliative medicine literature are indicative of some specific areas of concerns regarding the mental status of those requesting hastened dying. The oscillations of the wish to die of the terminally ill, the difficulties of diagnosing major depression toward the end of life, the effect of depression and demoralisation on euthanasia requests, and of what constitutes fitness to commit on rational suicide are significant and as yet unresolved clinical issues. Concerns of a ‘slippery slope’ remain, for competency determinations appear not to be strictly adhered to in some jurisdictions. Subjective medical impressions of suffering need to be supplanted by solid objective evidence-based literature and clinical guidelines. Medical practitioners of euthanasia and PAS appear reluctant and increasingly unenthusiastic participants in the processes. ‘Euthanasia talks’ may be therapeutic but medicinal killing, despite the informative experiences of jurisdictions in which it has been legalised, remains a controversial practice.
Every doctor has attended patients whose quality of life is poor and where no effective treatments are known or available. Psychiatrists are familiar with resistant affective disorders, chronic unremitting psychoses, and intractable anorexia nervosa. If legal liberalisation occurs the obvious evolution of pro-euthanasia advocacy is towards addressing those with intractable mental disorders and those weary with life in general. Psychiatry should be forewarned.
The euthanasia debate will not vanish from modern society. Society and politics will ultimately determine the legality of assisted dying in any community. As yet psychiatry does not have the expertise or the will to ‘select’ those whose wish for a premature death is rational, humane and ‘healthy’. Whether the profession will ever achieve this knowledge is uncertain. But until this is obtained doubts and concerns about assisted dying within psychiatry (and medicine) will persist.
Footnotes
Funding
This research received no specific grant from any funding agency in the public, commercial or not-for-profit sectors.
Declaration of interest
The authors report no conflicts of interest. The authors alone are responsible for the content and writing of the paper.