
Abstract

To the Editor
A 47-year-old man underwent a right hemicolectomy for a right lower quadrant mass and received a diagnosis of diffuse large B-cell lymphoma. A month later, he was referred to the psychiatry department because of cognitive fluctuation, abrupt onset of confusion, persecutory ideas and visual hallucinations following a second cycle of chemotherapy with the rituximab-CHOP (cyclophosphamide, doxorubicin, vincristine, prednisone) regimen. He was treated with haloperidol, after which his mental status improved. After a month, he developed a depressed mood, psychomotor retardation, generalized fatigue and insomnia. Upon a second psychiatric referral, he was treated with escitalopram for depression. After a total of four cycles of chemotherapy, he presented with chronic nausea, oral pain and sustained depression, which limited his oral intake. From that time on, he received prolonged parenteral nutrition for 2 months. On the 20th day of parenteral nutrition, the patient was referred again to the psychiatric department because of aggravated depressed mood, appetite loss, anergia and poor spontaneous speech. Five days later, the patient developed lethargy and confusion.
To evaluate his confusion, he underwent a brain MRI, which revealed bilateral medial thalamic high-signal lesions on T2-weighted images (Figure 1). Although a full neurological examination was not performed due to the patient’s somnolent condition, a diagnosis of Wernicke’s encephalopathy (WE) was made. However, even with 100 mg/day of thiamine (vitamin B1) intravenously for 5 days, the patient’s mental status did not improve. One month later, he developed pneumonia and died.
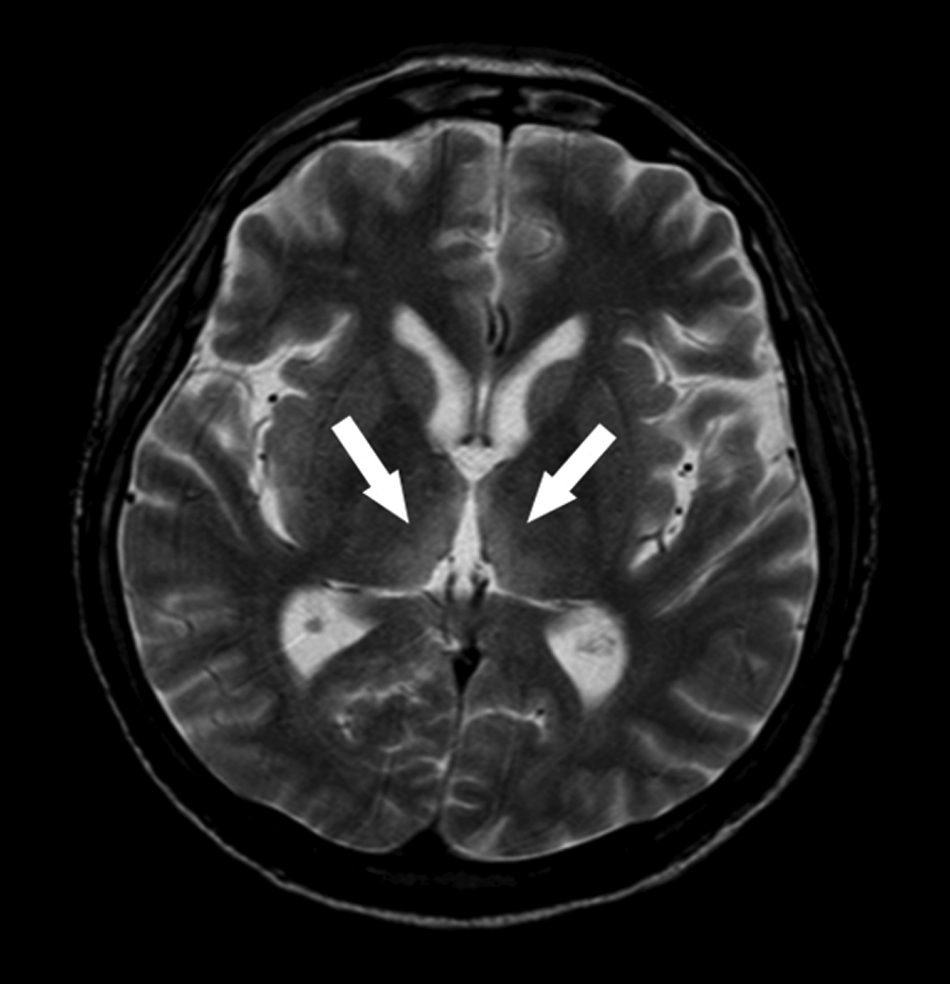
Axial brain MRI with T2-weighted image showing hyperintensity in the bilateral medial thalami.
WE is a neurological condition with a high mortality rate that results from thiamine deficiency. Early recognition and accurate diagnosis of WE is essential, but the classic symptoms of confusion, ataxia and ophthalmoplegia rarely occur concurrently, and thus have made early clinical diagnosis challenging.
Many critically ill cancer patients have multiple coexistent reasons for confusion (Kuo et al., 2009) and have a high risk of developing WE. In terminally ill cancer patients, clinicians must remain aware of the possibility of thiamine deficiency when patients with poor nutritional status present with unexplained delirium. If there is any doubt, intravenous thiamine administration even before definitive diagnosis (Onishi et al., 2004) is recommended to prevent the progression of this otherwise fatal disorder.
Although it was difficult for us to make a diagnosis of WE in our case due to the patient’s general weakness, the diagnosis was confirmed via a brain MRI. Classical reported MRI findings in WE are bilateral, symmetrical lesions around gray matter tissue of the mammillary bodies, anterior and medial nuclei of the thalamus, periventricular gray matter, and inferior and superior colliculi characterized by hyperintense signals on T2-weighted and fluid-attenuated inversion recovery (FLAIR) images (Sullivan and Pfefferbaum, 2009).
In conclusion, this report suggests that clinicians should have a high level of suspicion for WE in terminally ill cancer patients with confusion and consider a brain MRI for early accurate diagnosis and prompt treatment (Santos Andrade et al., 2010).