
Abstract
Objective
To review the policy and ethical implications of recent research on the molecular genetics of attention deficit hyperactivity disorder (ADHD).
Method
MEDLINE and psyclNFO database searches were used to identify studies on the genetics of ADHD. The implications of replicated candidate genes are discussed.
Results
The findings for most genes have been inconsistent but several studies have implicated the genes in the dopaminergic pathway in the aetiology of ADHD.
Conclusions
The current evidence on the genetics of ADHD is insufficient to justify genetic screening tests but it will provide important clues as to the aetiology of ADHD. Genetic information on susceptibility to ADHD has the potential to be abused and to stigmatize individuals. Researchers and clinicians need to be mindful of these issues in interpreting and disseminating the results of genetic studies of ADHD. Key words: ADHD, ethics, genetics, policy implications.
Attention deficit hyperactivity disorder (ADHD) raises significant controversy because of disagreements over its validity, assessment methodology, and treatment. Factors that contribute to concern include the facts that: (i) ADHD is the most common childhood psychological disorder; (ii) its prevalence is apparently increasing; (iii) the age of diagnosis is decreasing; and (iv) one of the most common forms of treatment involves daily administration of stimulant drugs to children and adolescents for extended periods.
According to epidemiological studies, the prevalence range of ADHD among children is 2.3–19.8%, depending upon diagnostic method [1–3]. The best estimate of prevalence is probably 3–7% [4]. Prescriptions of clonidine and stimulants, both used to treat ADHD, increased between two- and threefold, respectively, between 1991 and 1995 in children aged 2–4 years [5]. In Australia, the consumption rate of prescribed psychostimulants (largely used to treat ADHD) increased by 16% per year between 1984 and 2000 [6].
Clinical diagnosis of ADHD requires a comprehensive assessment using multiple sources of information [4]. This is necessitated by the complexity of the condition, its frequent comorbidity with other psychological disorders, and the fact that no single test produces a conclusive diagnosis [7]. DSM-IV criteria allow for three subtypes of ADHD: predominantly inattentive, predominantly hyperactive-impulsive, and combined. Additionally, approximately two-thirds of patients diagnosed with ADHD display comorbidity with other psychiatric conditions such as oppositional defiant disorder (ODD), conduct disorder (CD) and anxiety or mood disorders [8].
Questions have been raised about the usefulness of the DSM-IV categorical clinical diagnosis for defining ADHD. Some researchers suggest that stratification of ADHD families on the basis of comorbidity, especially the presence or absence of CD or bipolar disorder, may yield more genetically homogeneous groups [9,10]. Other research has suggested that ADHD is best conceptualized as a continuous trait rather than a categorical diagnosis defined by an arbitrary number of symptoms [11]. Additionally, latent-class analyses of ADHD symptoms suggest that DSM-IV criteria may exclude individuals who actually suffer from severe forms of the disorder [12].
The choice of treatment for ADHD is also controversial. Both psychosocial and pharmacological therapies can be used to treat ADHD. Psychosocial interventions include operant and cognitive-behavioural procedures, and often special education and parental management training [13]. Pharmacological treatments usually involve the use of stimulants, although antidepressants, antihypertensives and nicotinic drugs have been researched, trialled, and used [13,14]. The Multimodal Treatment Study for ADHD found that pharmacological therapy alone, or in combination with psychosocial therapy, achieved better results than behavioural treatments alone, while combined therapy was not superior to medication alone [15]. Although critics have argued that current treatments rely too heavily on medication, a recent study found that children with ADHD are more likely to receive psychosocial than pharmacological therapy [16].
Research into genetic influences on ADHD has the potential to resolve some of the controversies about it by increasing our understanding of the causes of the disorder and improving methods of diagnosis and treatment. We review recent research on candidate genes for ADHD and discuss their potential applications in its diagnosis and treatment. We also consider some of the ethical issues that may be raised by the use of genetic information about liability to develop ADHD.
Genetic influences
Twin studies suggest that both genetic and environmental factors influence the development of ADHD. Family and twin studies have found higher concordance rates for monozygotic twins (50–80%) than dizygotic twins (0–33%). Heritability estimates have ranged between 39% and 91% [17–19]. Although both genetic and environmental factors contribute to individual variances in liability for ADHD, this suggests that genetic factors account for a greater proportion of the variance [20]. Some studies have found that children with and without ADHD have similar quality of family environment [21], although this type of evidence has received criticism for methodological reasons [22].
Attention deficit hyperactivity disorder shows a complex non-Mendelian pattern of inheritance [23]. It is most likely that ADHD is a polygenic and multifactorial disorder that displays additive inheritance. This would mean that ADHD liability is influenced by a number of gene variants that are present in the general population. Each gene variant is likely to have a small effect upon the risk of developing ADHD. None of these genes is sufficient or necessary to cause the disorder, and the same phenotype may be produced by different combinations of variant genes. An individual only becomes liable to develop the condition when the number of variant genes exceeds a threshold [24]. The combined effects of many variant genes, environmental factors, and their interaction all contribute to ADHD susceptibility [10,20]. This complexity may make it difficult to identify genetic polymorphisms that influence ADHD liability.
Identifying candidate genes
Candidate genes for ADHD are usually selected on the basis of current knowledge of disease physiology, pathology and treatment. Association studies examine whether one allele, or variant, of a candidate gene occurs more often in individuals with ADHD than in some control comparison groups. In case-control studies, researchers compare the frequencies of alleles in patients with ADHD and in unrelated, unaffected controls that have been matched on age, sex and ethnicity [25]. In family-based studies using designs such as the transmission disequilibrium test (TDT) and haplotype relative risk (HRR) method, researchers study which alleles or haplotypes are transmitted from parents to affected offspring [25].
Linkage analyses are used to identify chromosomal regions that may contain genes that influence a complex genetic trait, or to evaluate genes that may be involved in disease aetiology. These studies trace the inheritance of genetic markers in affected relatives to detect an association between an allele and the disease [26,27]. Linkage studies often do not have the power to detect genes that have a small effect on a complex disorder such as ADHD [27].
In the following section we briefly review the findings of the most consistently replicated relationships between candidate genes and ADHD susceptibility. Many genes have been suggested to have involvement in ADHD aetiology, but few associations between ADHD and these genes have been consistently replicated (Table 1). Three reasons may explain the inconsistent findings, namely: false positives due to population stratification; lack of statistical power because of small sample sizes; and ascertainment bias with some studies using clinical diagnosis while others utilize questionnaire measures of symptoms [28].
Genes that have been investigated in relation to attention deficit hyperactivity disorder
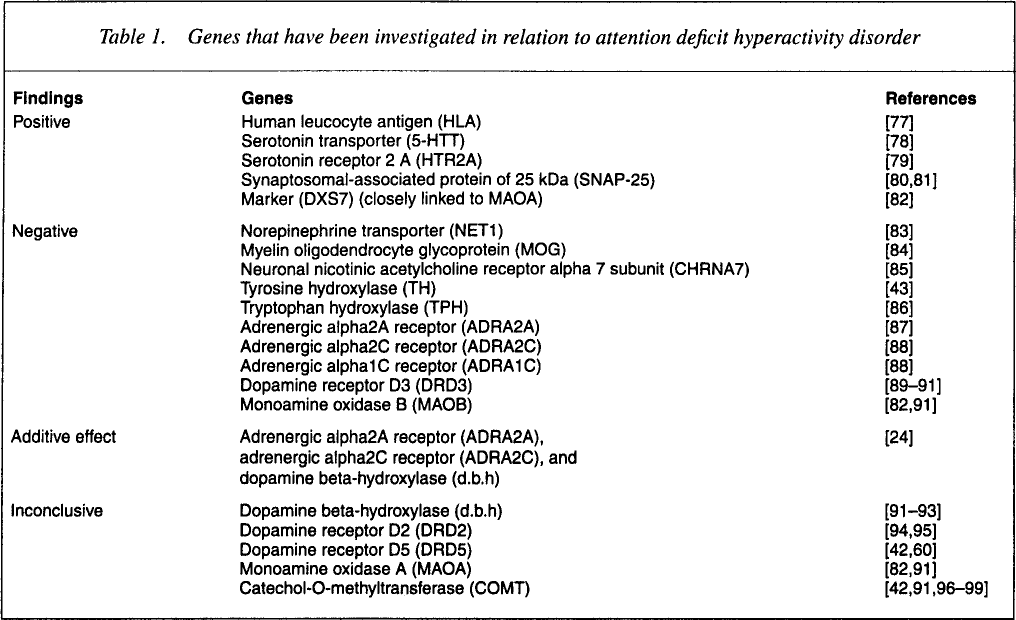
Studies of genes involved in the dopaminergic pathway have yielded the strongest associations with ADHD, so we focus on these. Interest in these genes has been stimulated by pharmacological and neuroimaging studies. Methylphenidate and amphetamines, which are widely used to treat ADHD, increase catecholamine transmission, specifically transmission of dopamine (DA) and norepinephrine (NE) [29,30]. Additionally, in children with ADHD and adults with histories of ADHD, neuroimaging studies have found reduced metabolism or volume of brain regions containing high levels of catecholamines. These findings suggest that the dysregulation of catecholaminergic circuits is involved in the aetiology of ADHD [29,31].
Dopamine receptor D4
Dopamine receptor D4 (DRD4) has been the focus of an intense amount of research on ADHD. DRD4 is one of five receptors that mediate the postsynaptic actions of DA. Exon 3 of DRD4 contains a 48-bp variable number of tandem repeats (VNTR) polymorphism. Different alleles of the VNTR alter the binding of ligands to the D4 receptor molecule [32]. The 7-repeat allele (DRD4*7R) of this polymorphism has also been associated with the trait of novelty-seeking [33,34]. This association and evidence on the role of DRD4 in the dopaminergic system make DRD4 a good candidate gene for ADHD.
The association between the DRD4*7R allele and ADHD has not been consistently replicated and different studies have found associations with different subtypes of the disorder. LaHoste et al. [35] first identified an association between DRD4*7R and the DSM-IV ADHD combined subtype. This same group confirmed the association, albeit with a refined phenotype [36]. Rowe et al. [37] provided further support for a role for DRD*7R in ADHD, but their results showed that DRD4*7R was more frequent in children with the inattentive subtype of ADHD than in control children. A recent study examined a different DRD4 polymorphism, a 120-bp repeat element upstream of the 5′–transcription initiation site. The 2-repeat allele was found to be associated with ADHD, especially the inattentive subtype [38]. This finding could be important as 5’ regions may affect transcriptional regulation of the gene.
Some research has suggested that the presence of the DRD4*7R allele may predict ADHD status, but the diagnostic value of DRD4*7 is unclear. The research of Rowe et al. [37] suggested that siblings with a higher number of DRD4*7R alleles display more inattentive symptoms than siblings with fewer DRD4*7R alleles, but these results were not statistically significant. Faraone et al. [39] also found evidence of a dose effect: within families the number of DRD4*7R alleles predicted the diagnosis of ADHD. In contrast, Manor et al. [40] found that individuals with the DRD4*7R allele performed better on a test of variables of attention than individuals with the 2-repeat allele. Using reaction time on a neuropsychological test, Swanson et al. [41] found, contrary to expectations, that children with ADHD and DRD4*7R had normal speed and variability of response, whereas children with ADHD but without DRD4*7R showed slow and variable response. A study by Tahir et al. [42] detected an increased transmission of the DRD4*7R allele to ADHD probands, but an inverse relationship between the allele and measures of clinical severity. However, the authors suggested that this finding may have been the result of sample selection bias.
Other studies have failed to find any association between DRD4*7R and ADHD. Using a twin-study design and a questionnaire assessment of ADHD symptoms, Payton et al. [43] reported a nonsignificant association between DRD4*7R transmission and ADHD. Using a case-control design, and behavioural and brain anatomic MRI measures, Castellanos et al. [44] did not find significant differences between children with ADHD and controls. The sample sizes of these two studies were smaller than most studies that have found a relationship. Barr et al. [45] examined the polymorphisms in the 5’ untranslated region of the DRD4 locus but failed to find a significant association with ADHD. Todd et al. [46] examined the relationship between both the exon 3 and the 5’ repeat elements, and DSM-IV and latent-class-derived ADHD subtypes. They did not find an association between either polymorphism and any ADHD subtypes, except for the 3-repeat allele of the exon 3 polymorphism and a novel talkative/impulsive latent-class-defined subtype.
Different study designs have also found different relationships between ADHD and DRD4*7R. Smalley et al. [47] found that DRD4*7R was preferentially transmitted from parents to their ADHD children, but did not find evidence of linkage between DRD4 and ADHD. In a family-based study by Holmes et al. [28], a higher frequency of the DRD4*7R allele was found in ADHD probands and their parents, when compared to matched controls. However, these results were nonsignificant, prompting the researchers to suggest that the association between DRD4*7R and ADHD in population-based studies could be spurious. A similar conclusion was reached by Mill et al. [48] who found a significant association between DRD4*7R and ADHD in a population-based case-control design, but failed to find differences in family-based studies. They attributed the results to population stratification.
Although the findings from individual studies are inconsistent, two recent meta-analyses suggest that DRD4*7R is associated with ADHD. Faraone et al. [49] who analyzed the results of case-control and family-based studies found a small but statistically significant association between DRD4*7R and ADHD. The authors did not find any evidence that the association was accounted for by any single study or publication bias [49]. A more recent meta-analysis by Maher et al. [50] of family-based studies produced similar results to Faraone et al. [49] in finding a modest association between DRD4*7R and ADHD. Thus DRD4 may have a modest influence on ADHD development.
Solute carrier family 6, member 3
Solute carrier family 6, member 3 (SLC6A3), also known as the dopamine transporter, has been investigated as a candidate susceptibility gene for ADHD. SLC6A3 is a strong candidate for involvement in ADHD because it is believed to facilitate DA reuptake into the presynaptic terminals and it is also the site of action of methylphenidate and dextroamphetamine, which are used to treat ADHD [51]. Cook et al. [52] found an association between the 10-repeat allele of a VNTR polymorphism at the SLC6A3 locus and DSM-III-R-diagnosed ADHD and undifferentiated attention-deficit disorder. This finding was confirmed by Gill et al. [53]. A subsequent study by Waldman et al. [54], using DSM-IV criteria, found that the SLC6A3 10-repeat allele was associated with the number of hyperactive-impulsive symptoms but not with inattentive symptoms. As was found for the DRD4*7R allele, siblings with more copies of the 10-repeat allele displayed more symptoms than their siblings who had fewer 10-repeat alleles [54].
Other studies on SLC6A3 have not produced such significant findings. In a nonclinical sample of twins concordant for ADHD symptom scores, Payton et al. [43] found a nonsignificant trend for increased frequency of the 10-repeat allele. Barr et al. [55] examined the VNTR as well as two additional SLC6A3 polymorphisms but did not find biased transmission of any polymorphisms. Holmes et al. [28] did not find any association between SLC6A3 and ADHD, despite a sample size that had up to 80% power to detect a previously reported association. A study using brain imaging failed to find association between the 10-repeat allele and amphetamine-induced DA release or dopamine transporter density [56]. Todd et al. [46] examined the association between the 10-repeat SLC6A3 allele and ADHD, using both DSM-IV diagnoses and subtypes derived by latent-class analysis. They did not find an association between any of the VNTR alleles and any of the ADHD subtypes.
Swanson et al. [57] examined the allele frequency of the 10-repeat allele reported by family based studies of SLC6A3 and found that the allele was present at a higher frequency in the ADHD samples than in controls. The authors did not find a significant association between ADHD and the allele in their own sample, although they suggested that this lack of association may have been a result of the small sample size of their study [57]. A subsequent meta-analysis of family-based studies of SLC6A3 by Maher et al. [50] did not find an association between the gene and ADHD but the authors noted that this was mainly due to the inclusion of a large sample study that was negative [58]. The inconsistent findings from SLC6A3 studies may reflect the gene's small contribution to overall ADHD liability, or the fact that it may be involved in only certain ADHD subtypes.
Dopamine receptor D5
The dopamine receptor D5 (DRD5) has not been subject to as much research as DRD4 or SLC6A3, but is nonetheless a promising candidate gene for ADHD liability. Like DRD4, DRD5 is involved in mediating the postsynaptic actions of DA. Daly et al. [59] first identified an association between ADHD and the 148 bp allele of a dinucleotide repeat in the DRD5 gene. Tahir et al. [42] provided support for this finding, identifying a trend for both linkage and association between ADHD and the 148 bp allele. Payton et al. [43] identified a trend for preferential transmission of the 148 bp allele to ADHD probands, but these results did not reach significance. A fourth study investigating this polymorphism found biased transmission of the 136 bp and 146 bp alleles of the DRD5 polymorphism, but not the 148 bp allele [60]. A recent meta-analysis of these studies confirmed the association between DRD5 and ADHD [50]. Additionally, two studies have found evidence of positive linkage between the DRD5 locus and ADHD [61,62].
Multigenic and genome scan approaches
The hypothesized polygenic nature of ADHD has prompted some researchers to study multiple candidate genes for ADHD [51,63]. Comings et al. [63] examined the association between ADHD and 20 genes, including those from dopamine, serotonin, and adrenergic pathways. They found that noradrenergic genes accounted for three times as much variance of ADHD score as dopamine genes, which only accounted for 2.3% [63]. A subsequent study added 22 hormone, neuropeptide, and neurotransmitter genes to the original set of 20 [51]. The noradrenergic genes still had the strongest association with ADHD. The total percent of variance accounted for by the 20 genes in the first study was 11.6, but 22 genes in the new study accounted for 21.7% of the total variance in ADHD scores. These two studies also suggested that ADHD, ODD and CD share common genetic influences.
Fisher et al. [61] used a genome-wide scan method to identify loci involved in ADHD, but they did not find any chromosomal regions that exceeded the genome-wide significance threshold. This finding is consistent with the assumption that the pattern of inheritance in ADHD is polygenic. Several regions with more moderate effects on ADHD susceptibility were identified, but 29 of 36 candidate genes for ADHD, including SLC6A3 and DRD4, did not contribute to genetic susceptibility. It was argued that SLC6A3 and DRD4 probably have very minor effects. In contrast, a region containing DRD5, serotonin transporter, and dopamine D1 receptor-interacting protein, had positive linkage. Two regions identified in this study, 2q24 and 16p13, coincide with regions implicated in autism. A subsequent study performed similar analyses and also identified 16p13 as a highly significant susceptibility locus for ADHD [64].
Summary
These studies support the hypothesis that the dopaminergic pathway is involved in the aetiology of ADHD but the relationship between the dopamine genes and ADHD is not well understood. Further investigation is needed to discover whether particular alleles are only involved in liability to certain subtypes of ADHD and whether these alleles are associated with true susceptibility alleles. The conflicting results of these studies and the small associations with identified susceptibility alleles are consistent with the hypothesis that ADHD is a polygenic disorder in which individual susceptibility alleles will only make a minor contribution to risk of the disorder.
Applications
Diagnosis
Although current knowledge of genetic susceptibility to ADHD is inadequate for use in testing, genetic tests may eventually be used to assist clinicians in determining a more precise diagnosis for patients. The research suggests that ADHD is a genetically heterogeneous disorder, so one reason for testing for susceptibility alleles may be to identify subtypes of ADHD that have differing prognoses. Genetic studies have confirmed that ADHD is often comorbid with other childhood psychiatric disorders and shares a genetic liability with CD and ODD [18,65]. This may have implications for diagnosis of ADHD, CD and ODD.
Studies of multiple candidate genes by Comings et al. [24,51,63] have provided strong evidence that ADHD is a polygenic disorder in which genetic risk is distributed in a continuous, rather than discrete, fashion. Comings et al. [63] have suggested that in the future multigene tests may have diagnostic applications with the testing of multiple susceptibility genes on DNA chips.
Treatment
Genetic information may assist in making decisions about pharmacological interventions for ADHD. Individuals with ADHD vary in their response to psychostimulants [66], and some studies suggest that response to methylphenidate has a genetic component. Winsberg et al. [67] for example, found that homozygosity for the SLC6A3 10-repeat allele was associated with non-response. This finding was replicated by Roman et al. [68]. There is also evidence to support the involvement of DRD4 and DRD5 in methylphenidate response. Tahir et al. [42] found that by excluding methylphenidate nonresponders from their sample of ADHD subjects, they obtained more significant association between the two dopamine receptors and ADHD. Studies of this type may lead to the use of genetic tests to determine the most effective treatment for ADHD patients [66].
More controversially, genetic information on ADHD susceptibility may be used for the early identification of persons who are at increased risk of ADHD, to whom preventive interventions could be applied [52,63]. Genetic screening strategies for behavioural traits such as alcoholism and depression have been discussed [69,70], and it is possible that similar proposals could be made for ADHD. This proposal would raise ethical implications, which are discussed later.
Ethical implications of predictive genetic testing
The probabilistic nature of genetic information
Any tests for susceptibility genes for a polygenic condition like ADHD will only provide a probability of developing the disorder. They cannot predict whether the individual will develop the disorder. The multifactorial nature of ADHD also means that environmental risk factors need to be taken into account in assessing the risk of developing the disorder. It is also likely with a polygenic disorder like ADHD that most individuals in the general population will carry one or more susceptibility alleles. Only a small percentage of individuals will carry enough susceptibility alleles to predict a high risk of developing the disorder. Consequently, the number of individuals that would need to be tested to identify those people at risk is likely to make proposals for population-wide genetic screening very costly. Additionally, there is the potential for false-positive predictions that could lead to misdiagnosis and stigmatization.
The use of genetic tests for ADHD susceptibility is likely to be more useful in clinical populations where they may assist diagnosis and the selection of appropriate treatments. As with current diagnostic methods that use multiple sources of information [31], a genetic test is unlikely to be the sole basis of a clinician's diagnosis. It is more likely to be used to refine prognosis or clarify a diagnosis in an individual with a diagnosed clinical disorder [71].
Genetic testing of minors
Any of the potential uses of genetic testing described above requires the testing of minors, which could be problematic for a number of reasons. First, most children with ADHD are diagnosed before the age of 7 years, and therefore the child's parents or guardians would have to provide consent for any genetic test on behalf of the child. This raises issues about the rights of parents to make decisions for their children that may have important health implications [72]. Second, the primary goal of the test should be to promote the welfare of the child [71]. For a child displaying ADHD symptoms, a genetic test for ADHD could offer immediate medical benefits, in terms of better treatment outcomes [73]. A genetic test would be more doubtfully used in prenatal screening, or in making decisions about adoptions. In such cases, the test would offer no immediate benefit in facilitating medical or reproductive decisions and any such use would need to be carefully evaluated [73].
Third, a genetic test has potential to do harm. A positive result may lead to stigmatization of the child in question [72,73]. Parents and others may lower their expectations for the child's education, personal relationships, or employment, which may mean that a child with an increased risk of ADHD is not encouraged to reach his or her full potential [74]. Due to a child's inability to understand complex genetic information, guilt, self-blame, or a feeling of unworthiness may be fostered or reinforced [74]. Despite the fact that a genetic test may reduce uncertainty and facilitate openness within the family, it could also have negative impacts on family dynamics [71]. The child with ADHD may be overindulged, rejected, or treated as a scapegoat who reminds a parent of his or her own undesirable traits [73].
These issues may receive less emphasis in situations where ADHD has already been diagnosed or is suspected. In such cases a genetic test is likely to confirm what is already known, or may assist in treatment. We believe that the importance of these issues should make us very cautious about accepting any proposals that may be made to test for ADHD susceptibility alleles in the general population.
Confidentiality and privacy
The confidentiality of genetic information relating to ADHD susceptibility needs to be ensured, especially where it relates to minors. In the case of ADHD, it may be necessary to disclose test results to the guardians of the minor child and the clinician. However, other parties, such as schools or insurance companies, may also gain access to this information [73] if, as has been reported, parents use the diagnosis to gain additional educational services for the child [75]. The unnecessary disclosure of genetic information may lead to harmful labelling in the classroom [76]. Additionally, a polygenic test result could provide information that is used to make inferences about risks of other disorders in the individual (because of linkages with other genes) or disorders in other family members (because of the familial nature of genetic information).
Conclusions
Attention deficit hyperactivity disorder can have a major impact on young patients, their families, and society. Genetic research has identified a number of genes that may increase the risks of developing ADHD. Studies of single candidate genes have been inconsistent for a variety of reasons that may be circumvented in future research. Due to limited knowledge on specific locations of polymorphisms in the target genes, it is unclear whether the polymorphisms studied to date are truly susceptibility genes or associated with other genetic loci that contribute to the disorder.
If genetic studies produce replicable candidate genes, their results have the potential to improve the diagnosis, treatment, and understanding of ADHD. Before the information from genetic studies can be fully incorporated into psychiatric treatment for ADHD, the ethical issues raised by its use must be addressed. In order to ensure that the information is used correctly, policies need to be implemented to ensure that children with ADHD do not suffer the adverse effects of discrimination or stigmatization by educational institutions, insurance companies, prospective employers, or their own families.
Footnotes
Acknowledgements
This research was partially funded by the Cooperative Research Centre for the Discovery of Genes for Common Human Diseases through their Undergraduate Research Opportunities Program and the Vice Chancellor's Strategic Research Fund at the University of Queensland.