
Abstract
Background
This study examines the association between the coefficient of variation (%CV) of lithium levels and episode risk and frequency in bipolar patients maintaining serum lithium levels within the therapeutic range.
Methods
We retrospectively reviewed patients with bipolar disorder under care from 2018 to 2022. Inclusion criteria were at least 2 years of follow-up, a minimum of three annual lithium level measurements within the therapeutic range. Patients were categorized based on seizure status. We calculated mean lithium levels, standard deviation (SD), and %CV.
Results
The study included 75 patients (patients with-without episodes, 39–36). Demographic data revealed no significant differences. While mean lithium levels showed no significant disparity between groups, SD and %CV were notably higher in patients with episodes (P < .05). ROC analysis demonstrated AUC values of 0.722 (95% CI: 0.607–0.836 P = .001) for %CV and 0.709 (95% CI: 0.593–0.826; P = .002) for SD. The optimal %CV cutoff was 17.39, with 67% sensitivity and 69% specificity. A weak correlation was found between %CV and the number of episodes (P = .001, r = 0.376). The post-hoc power analysis for this study was 0.78.
Conclusions
Despite acceptable lithium levels, patients with recent episodes exhibited significant lithium level fluctuations. Integrating %CV with real-time lithium measurements during bipolar disorder follow-up may enhance clinical monitoring and seizure prediction.
Introduction
Bipolar disorder is a psychiatric disorder in which episodes of manic and depressive mood recur with different clinical courses from person to person. Its prevalence in the general population ranges from 1% to 3%, but this can increase to 4% to 15% in individuals with a family history of bipolar disorder. 1 In patients diagnosed with bipolar disorder, regular treatment and follow-up are required to reduce the frequency of episodes, manage the psychological and social effects of the disease, and increase the person’s functionality. The primary approach to treatment involves pharmacotherapy, often complemented by psychotherapy. 2 Continuity and follow-up of treatment are important because 70% of patients have a risk of relapse within 5 years despite treatment. Available treatment options include single or combination therapy with lithium, valproic acid, lamotrigine, carbamazepine, antipsychotics, and benzodiazepines. 3 According to current treatment guidelines, the therapeutic range of lithium, which is still the first choice in treating bipolar disorder, should be 0.6–1.5 mmol/L in patient serum. 4 However, this drug has a narrow therapeutic window, with potential side effects like sedation, tremors, weight gain, diarrhoea, nausea, polydipsia, polyuria, cognitive disturbances, hypothyroidism, and diabetes insipidus. Fatal doses can result from uncontrolled use. Hence, serum lithium levels should be monitored every 1–2 weeks following the initiation of the medication and every 3–6 months for regular follow-up. 5 Despite these side effects, lithium effectively reduces the risk of recurrence of mood episodes. 6 Individual characteristics such as age and physical attributes can also influence lithium levels. 7
The coefficient of variation (%CV) is a statistical value that makes it possible to calculate the variability of simple, classified data series with different means, regardless of the unit of measurement used for these numbers and the mean of the numbers. It is obtained by dividing the standard deviation of the data set by its arithmetic mean, then multiplying the result by 100. The %CV is expressed as a percentage, and it does not have a specific unit of measurement. 8
Studies in the literature examine the relationship between patients’ instantaneous serum lithium levels and the risk of an attack.9,10 Regular lithium use protects patients with bipolar disorder from attacks. 11 In clinical observations, patients have been reported to experience manic and/or depressive episodes even if serum lithium levels are in the therapeutic range. 12 We observed that some patients with bipolar disorder had attacks despite serum lithium levels in the therapeutic range. As far as we know, there are studies in the literature related to serum lithium levels, but no study conducts variation analysis. The aim of this study is to assess the fluctuation in lithium levels with the %CV among patients diagnosed with bipolar disorder who experience episodes despite having serum lithium levels within the therapeutic range during follow-up. Additionally, we aim to investigate the correlation between these fluctuations and the risk and frequency of episodes.
Materials and methods
The study has been approved by Adiyaman University Institutional Clinical Research Ethics Committee (Approval No: 2022/9-6) and conducted following the Helsinki Declaration. The diagnosis of bipolar disorder was made according to the Fifth Edition of the Diagnostic and Statistical Manual of Mental Disorders (DSM-5). 13 The clinical notes and laboratory results of bipolar disorder patients who presented to the psychiatry clinic between 2018 and 2022 were retrospectively reviewed in the hospital information system. Patients who were followed for at least 2 years, had at least three blood lithium levels per year, and had lithium levels within the therapeutic range (0.6–1.5 mmol/L) during their follow-up were included in the study. Patients with additional organic diseases, such as psychiatric or renal conditions, which could influence blood lithium levels, as well as those with fewer than three blood lithium results per year, and those without regular follow-up, were excluded from the evaluation. The patients included in the study were evaluated into two groups, based on their examination notes: those who experienced an episode in the last 2 years of follow-up and those who remained without episode for 2 years. Manic episode considered as a distinct period of abnormally and persistently elevated, expansive, or irritable mood, lasting at least 1 week and be present most of the day, nearly every day. During the period of mood disturbance, three (or more) of the following symptoms have persisted (four if the mood is only irritable) and have been present to a significant degree: Inflated self-esteem or grandiosity, decreased need for sleep, increased talkativeness, racing thoughts, distractibility, increase in goal-directed activity or psychomotor agitation, excessive involvement in pleasurable activities that have a high potential for painful consequences. And for the diagnosis of depressive episode, a patient must experience five or more of the following symptoms, which must persist most of the day, daily, for at least 2 weeks in a row: depressed mood, loss of interest or pleasure in all/almost all activities, significant weight loss or decrease or increase in appetite, sleep disturbance, fatigue or loss of energy, feelings of worthlessness or guilty, recurrent thoughts of death or suicidal ideation-attempts, diminished ability to think or concentrate or indecisiveness, severe psychomotor changes (agitation or retardation). 13 At our center’s Mental Health and Diseases Clinic, blood lithium levels are checked at 3–6 month intervals in bipolar disorder patients in remission. Patients have 5 cc of venous blood drawn 12 h after the nighttime lithium dose. Venous blood samples are obtained using the antecubital vein. The samples are analysed using the spectrophotometric method on the Abbott Architect c16000 analyser (Abbott Diagnostics Inc., Lake Forest, IL, USA), and the results for patients are uploaded to the patient record system within a maximum of 3 days. According to this device, the reference range for lithium is 0.6–1.5 mmol/L.
The study data were analysed using Statistical Package for Social Sciences (SPSS) for 23.0 Windows software programs, and a significance level of 0.05 was considered. The mean, standard deviation (SD), and CV% of the 2-year lithium results for each patient included in the study were calculated. The formula ‘(SD/mean) × 100’ was used for %CV. The Kolmogorov–Smirnov test assessed the deviation from a normal distribution. Quantitative variables were summarized as median (interquartile range [IQR]) for non-parametric data. Non-parametric continuous data were analysed by Mann–Whitney’s U tests. Spearman’s Rank test did the analysis of correlation. Receiver-operating characteristics (ROC) analysis was performed to estimate the sensitivities and specificities of %CV to evaluate attack risk. A statistical post-hoc power analysis was done by G-power 3.1.9.2 software program. 14
Results
The demographic data of the patients and the mean, SD, and %CV values for the 2-year lithium results are as follows.
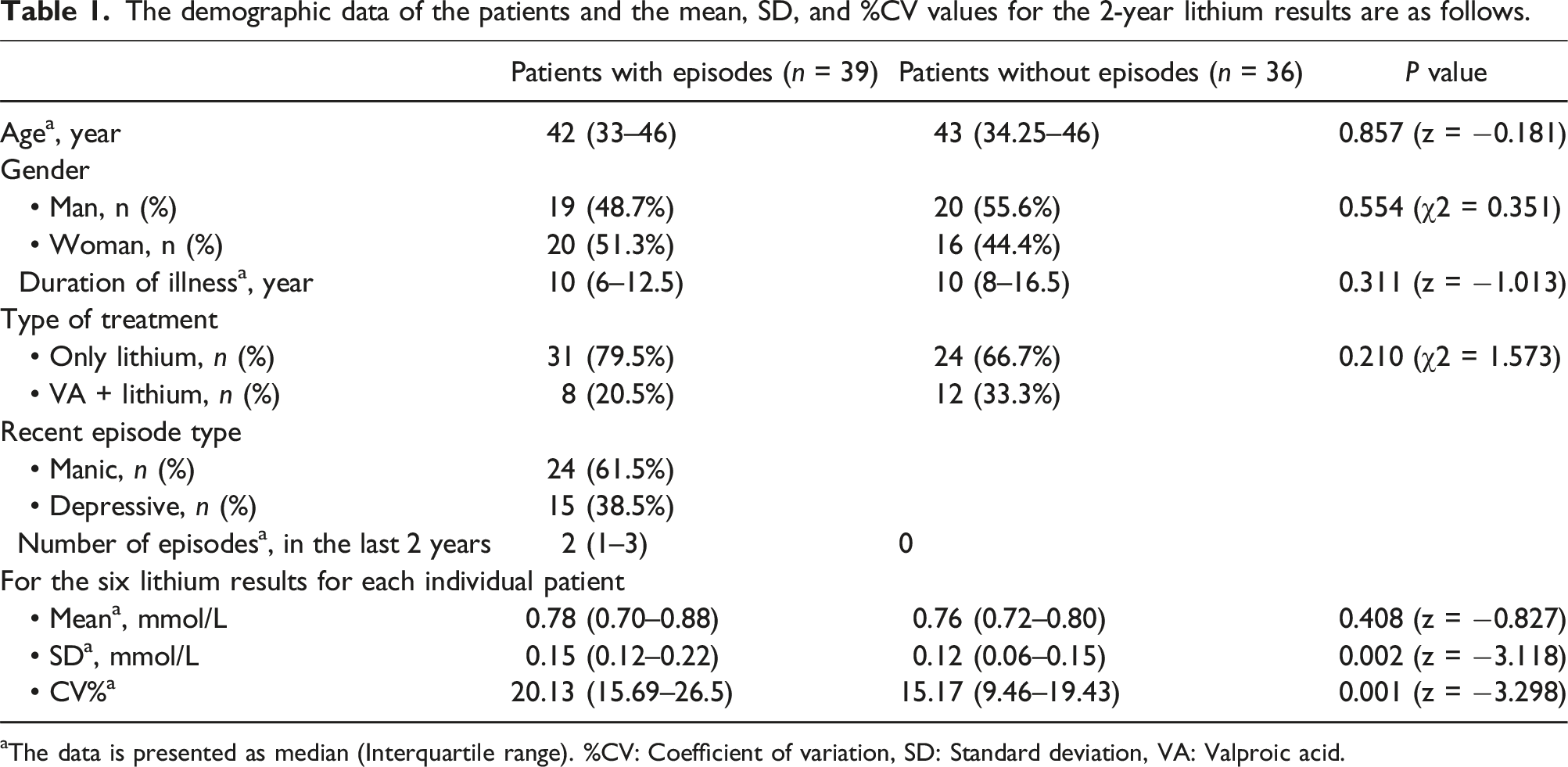
aThe data is presented as median (Interquartile range). %CV: Coefficient of variation, SD: Standard deviation, VA: Valproic acid.
The mean and SD values of the last six lithium results within the previous 2 years for patients in both groups, as well as the %CV values calculated using these two parameters, are provided in Table 1. Among these both groups with therapeutic range lithium values in follow-up, no significant difference was detected between the mean lithium levels. In contrast, the SD and %CV values were significantly higher in the patients with episodes (P < .05). In the subgroup analysis, where we grouped the patients with episodes group based on the last attack type, there was no statistically significant difference between those with the previous attack being manic and those with the latest attack being depressive in terms of mean, SD, and %CV values.
In the ROC analysis conducted to determine the superiority of SD and %CV in predicting the attack, the area under the ROC curve was found to be 0.709 (95% CI 0.593–0.826; P = .002) for SD and 0.722 (95% CI 0.607–0.836; P = .001) for %CV. According to the calculation based on the Youden index, the optimal value of %CV in predicting the attack was 17.39 or higher, with a sensitivity of 67% and specificity of 69%.
A statistically significant but weak correlation was found in the correlation analysis between the number of attacks patients experienced in the last 2 years and the %CV values of their lithium levels in the previous 2 years (P = .001, r = 0.376).
In the post-hoc power analysis using the G-power program, the effect size was 0.70 and found to be medium-large. With α = 0.05 and 0.70 effect size, the post-hoc analyses revealed that the statistical power for this study was 0.78.
Figure 1 was generated to demonstrate the application of %CV. In Figure 1, line graphs depict six lithium results over the past 2 years for three bipolar patients who experienced an episode despite having therapeutic lithium levels and three control bipolar patients who maintained therapeutic lithium levels and remained episode-free for 2 years. While %CV values were found to be high in the patients with episodes group (%CV values respectively: Patient 1, Patient 2, Patient 3; 28.5, 37.5, 29.3), it was observed that %CV values were lower in the patients without episode group due to lithium levels being within normal limits and within a narrower range in the last 2 years (%CV values respectively: Control 1, Control 2, Control 3; 4.82, 7.07, 7.10). Two-year lithium levels of patients (three from the control group and three from the patient group).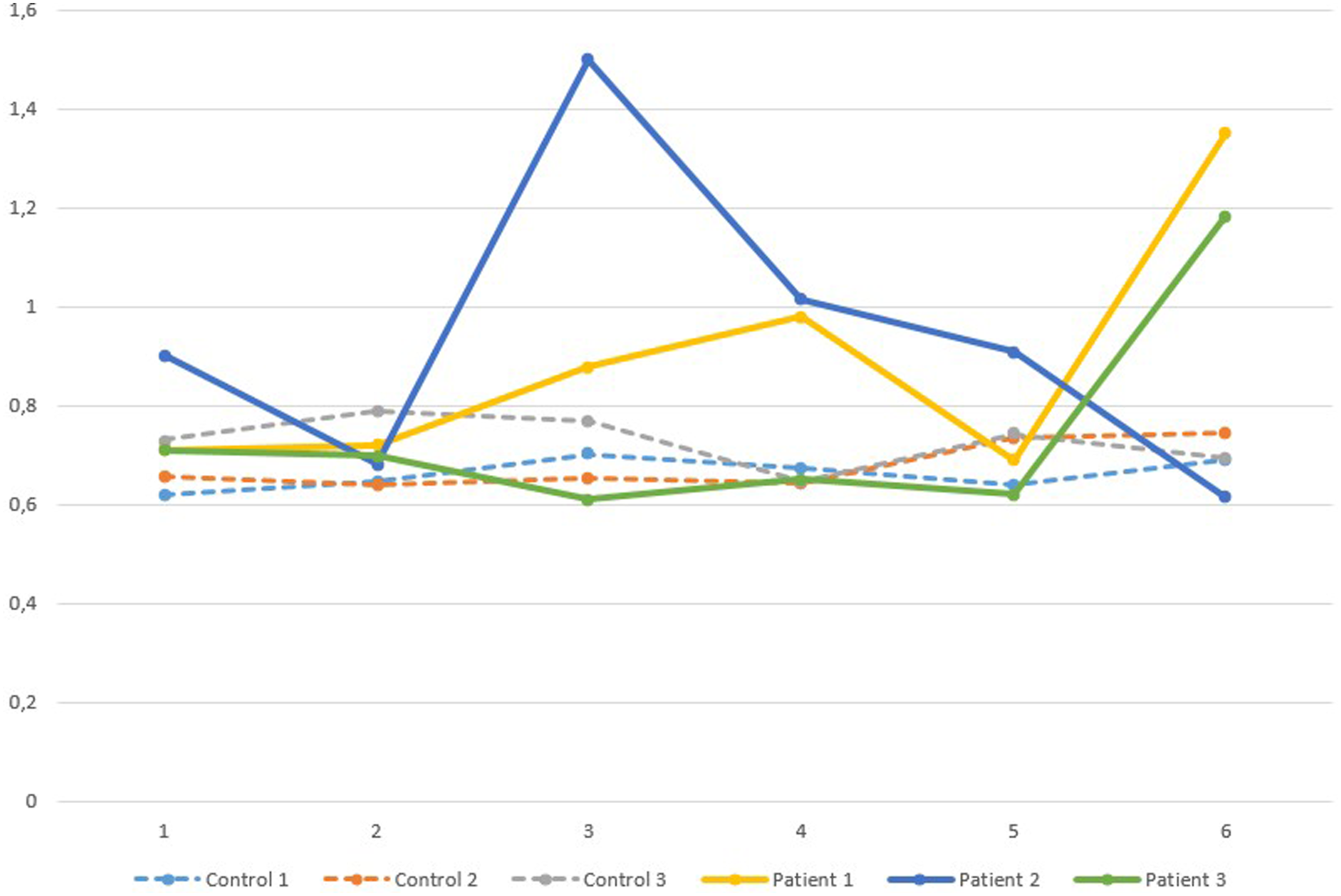
Discussion
We observed that %48 of bipolar disorder patients using lithium, both those who experienced manic/depressive episodes and those who did not, were female. Although the course and clinical characteristics of bipolar disorder may vary between women and men, there is no evidence to suggest that gender influences the response to mood stabilizers in treatment. 15 We also did not detect any differences in terms of gender between bipolar disorder patients who experienced episodes and those who did not. The mean age of the patients was 43 (33–46), and we did not find any difference in mean age between the two groups. However, bipolar disorder is typically seen in younger people. 16 While age can significantly affect mood-stabilizing medications’ protective effects, we believe patients tend to be more motivated for regular blood tests, follow-up, and treatment compliance as age advances.17,18 Therefore, we observed that patients with lithium levels checked at least three times a year in the last 2 years were older.
In this study, we did not observe any difference in mean lithium levels between the groups with and without episode among individuals diagnosed with bipolar disorder and using lithium. However, we observed that individuals who experienced episodes had higher SD and %CV values regarding lithium levels. A meta-analysis study conducted with 1406 individuals reported that serum lithium levels between 0.4 and 0.8 mmol/L significantly protected bipolar patients from major mood episodes. 19 However, in a prospective study where bipolar disorder patients receiving lithium monotherapy were observed for 2.5 years, it was found that patients’ mood symptoms worsened while under treatment. During the 2.5-year follow-up period, it was noted that intervention was necessary for manic or mixed mood symptoms in 27 patients, and 22 patients required treatment for depressive symptoms. It was found that the mean blood lithium levels before the recurrence of manic or mixed symptoms were lower than before the recurrence of depressive symptoms (0.53+/−0.13 vs 0.66+/−0.21 mmol/l, P = .01). In conclusion, Kleindienst et al. suggested that manic or mixed recurrences can occur at lower lithium levels, whereas depressive episodes tend to occur at higher levels. 10 Severus et al. also observed that patients within the accepted therapeutic range while using lithium experienced attacks. 20 They noted that lithium levels in the lower range of the therapeutic spectrum may be sufficient to prevent depressive episodes, but higher lithium levels than this range may be needed for protection against manic/mixed episodes. Our study found that lithium levels within the therapeutic range and experiencing an attack did not significantly differ based on whether the last attack type was manic or depressive. It is believed that this situation may be related to the small number of cases in the study.
In the ROC analysis conducted to determine the superiority of SD and %CV in predicting attacks, we observed that the variation coefficient had a sensitivity of 68% and specificity of 67% in predicting attack risk. We observed that it may not be sufficient as a predictor. However, we believe that it can still alert clinicians to the occurrence of episodes, as observed in patient follow-up, as shown in Figure 1. %CV is superior to SD, especially in evaluating variability of simple in two groups with different mean values. In our study, although the mean values of the two groups were very close, CV was revealed to be a superior predictor in showing variability. If the means of the two groups were markedly different, CV might be expected to be an even better predictor.
Among the study’s limitations, we can mention the retrospective nature of the evaluation, which prevented the optimization of other factors that could have contributed to the patients’ episodes. Another limitation is the potential impact of drug intake and variations in blood sampling. 21 While our patients are informed about this concern, the timing of blood collection and drug intake may vary, particularly among outpatients. Variations in %CV values could be influenced by the pharmacokinetics activity of the drug. Additionally, some patients were using valproic acid alongside lithium, and the relatively small sample size is our other limitations.
In conclusion, the coefficient of variation can be used as a parameter indicating that even in bipolar disorder patients with lithium levels within the therapeutic range, there is a high fluctuation in lithium levels over time. The high %CV values indicating lithium fluctuation may be one of the reasons behind the episodes observed in patients with lithium levels within the therapeutic range. Although weak, the observed correlation between the frequency of occasional attacks and the %CV values of lithium results supports this. During outpatient follow-ups, evaluating the patient’s laboratory results, including instant lithium levels, %CV value, can benefit the patient’s clinical assessment. We believe supporting this hypothesis with a more extensive patient series would be appropriate.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
Not applicable.
Guarantor
SBO.
Contributorship
Conceptualization [SBO, ŞS]; Data curation [SBO, ŞS]; Formal analysis [SBO, ŞS]; Investigation [SBO, ŞS]; Methodology [SBO, ŞS]; Project administration [SBO, ŞS]; Supervision [BHA, İGÇ]; Roles/Writing - original draft [SBO, ŞS, SY]; and Writing - review & editing [SBO, ŞS, SY, BHA, İGÇ].