
Abstract

Dear Editor,
We wish to share our experience of total and active B12 discordance in non-iatrogenic hypervitaminosis B12. 1 In health, circulating vitamin B12 is bound to haptocorrin, forming holohaptocorrin (80%–96%) or transcobalamin, forming holotranscobalamin (6%–20%). Only vitamin B12 bound to transcobalamin is available to the cells and biologically active, whereas vitamin B12 bound to haptocorrin is biologically inactive. Total B12 assays measure holohaptocorrin and holotranscobalamin, whereas active B12 assays measure only holotranscobalamin.
Hypervitaminosis total B12 has been reported in haematological malignancies, liver disease, metastatic and non-metastatic solid tumours, advanced renal disease, autoimmune conditions and infections2–6 or may be spurious due to immunoassay interference. 7 It has, therefore, been suggested that an unexpected high total B12 should prompt an evaluation for serious disease.5,6
Hypervitaminosis total B12 in haematological and other malignancies is largely due to haptocorrin directly released from myeloid cells or neoplastic cells, respectively, which then binds B12 in the circulation in preference to transcobalamin.5,6,8 Some malignancies, however, may secrete transcobalamin. 3 In severe liver disease, destruction of liver parenchyma releases holohaptocorrin or impairs hepatic uptake of circulating B12, increasing either holohaptocorrin or holotranscobalamin or both.2,4,8 In severe renal disease, reduced clearance increases holotranscobalamin and holohaptocorrin. 5 Autoimmune and infectious conditions increase both bound fractions. 5
Paradoxically, hypervitaminosis total B12 may coexist with functional B12 deficiency.5,6 Utilising an automated active B12 assay, we report on the prevalence and causes of B12 deficiency in patients with hypervitaminosis total B12.
Over 12 months, patients’ serum samples with a high serum total B12 (>1000 pg/mL; reference interval 187–853 pg/mL) were identified and aliquoted surplus serum frozen at −80°C. Medical data were collected from the hospital and primary care electronic medical records. Samples and data from patients prescribed vitamin B12 were discarded. Following anonymisation, samples were analysed for active B12.
Total and active B12 were measured using methods and reagents supplied by Abbott diagnostics on the Abbott ARCHITECT i2000sr analyser (Abbott Diagnostics, Abbott Park, IL, USA). Active B12 deficiency was defined as a serum concentration ≤25 pmol/L (reference interval 25.1–165.0 pmol/L).
Clinical and laboratory data on patients with high total B12 and active B12 deficiency.
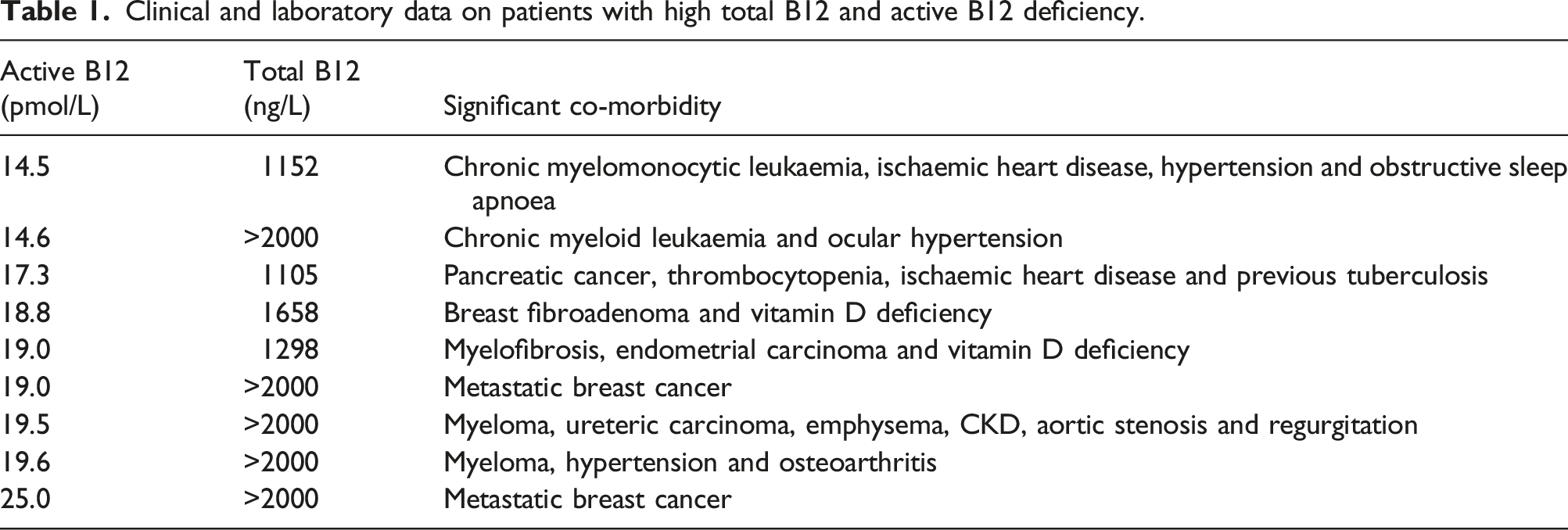
These results support the notion that hypervitaminosis total B12 may coexist with biologically active vitamin B12 deficiency. Apart from breast fibroadenoma, the underlying aetiology of this paradox was malignant disease, particularly haematological cancer. We suggest that active B12 is the preferred automated biomarker for assessing vitamin B12 status in those with malignant disease as total B12 may be misleading.
Footnotes
Data availability statement
All relevant data are included in the letter.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
This work was part of an institutional registered service evaluation (Audit ID 5044).
Guarantor
NL.
Contributorship
JP, HS, RV and MB collected the data. NL wrote the first draft. All authors reviewed, revised and approved the final version of the letter.