
Abstract
Background
Although venipuncture is minimally invasive, and is the most frequently performed medical procedure, it carries the small risk of causing persistent pain, including nerve damage. Recently, our hospital stopped using 22-gauge needles for venipuncture in outpatients and switched to using only 23- and 25-gauge needles. We investigated the impact of using only the finer needles on the incidence of persistent or neuropathic pain and the prevalence of haemolysis, as well as the impact of haemolysis associated with the needle change on other laboratory data.
Methods
We retrospectively collected and analysed data on venipuncture-associated pain complaints made during the 1-year period prior and 1-year period after the change in needles, as well as the frequency of haemolysis before and after the change. We also focused on 90 cases that showed significant haemolysis after the needle change and compared the serum aspartate aminotransferase, lactate dehydrogenase, and potassium levels before and after the needle change.
Results
The incidence of persistent pain was significantly reduced from 1 in 10,825 venipunctures before the change to 1 in 29,747 venipunctures after the change. Notably, no patients experienced neuropathic pain after the change. However, the prevalence of haemolysis was significantly increased. Additionally, the serum aspartate aminotransferase, lactate dehydrogenase, and potassium levels were significantly elevated in the cases that showed moderate to gross haemolysis after the needle change.
Conclusion
Using finer needles involves both advantages and disadvantages, and careful consideration is needed to determine which type of needle is in the best interests of the patient.
Introduction
Venipuncture to collect blood samples is one of the most frequently performed medical procedures. The obtained blood samples are used for clinical laboratory testing to evaluate the condition of patients, determine differential diagnoses, and help doctors make decisions. Although laboratory tests using blood samples are thus essential in daily clinical practice, venipuncture carries a small, but definite risk of causing serious complications, such as nerve damage.1–3 A retrospective study from our hospital has demonstrated that the incidence of persistent pain after venipuncture for blood sampling is relatively low and that the prognosis is good. 4 However, medical safety requirements are becoming increasingly stringent. We have therefore recently stopped using 22-gauge butterfly needles in our blood sampling division and have switched to using only 23- and 25-gauge needles. Such use of finer needles is expected to reduce the incidence of pain and nerve damage associated with venipuncture but may increase the risk of haemolysis, which is a major source of interference in laboratory testing. In the present study, we investigated the changes in the incidences of persistent pain and neuropathic pain associated with venipuncture and the frequency of haemolysis after switching to the finer needles to examine the advantages and disadvantages of the change. We also investigated the effects of haemolysis associated with the needle change on the laboratory data.
Materials and methods
Incidences of persistent pain and neuropathic pain after venipuncture
In our hospital, blood is drawn from outpatients in the blood sampling division, which is part of the Department of Clinical Laboratory. In the outpatient section, trained clinical laboratory technicians perform the venipunctures. When a patient feels persistent pain after venipuncture, a physician in the Department of Clinical Laboratory examines the patient. If the physician judges that the patient needs more specialized care, the patient is referred to the Department of Orthopaedics, and if a patient is diagnosed with neuropathic pain, specialized treatment of the pain is provided. All patients with persistent pain were included in the present study, and all patients with neuropathic pain were diagnosed by orthopaedic surgeons.
In the outpatient section of the division of blood sampling, 22-, 23-, and 25-gauge butterfly needles were used for venipuncture prior to 21 July 2019. As an attempt to reduce the number of complaints of pain associated with venipuncture, the use of 22-gauge needles was discontinued, and only 23- and 25-gauge needles were used from 22 July 2019. In the present study, we aggregated the numbers of patients showing persistent pain and neuropathic pain 1-year period before (from 22 July 2018, to 21 July 2019) and the 1-year period after (from 22 July 2019 to 21 July 2020) the change was made to stop using the 22-gauge needles.
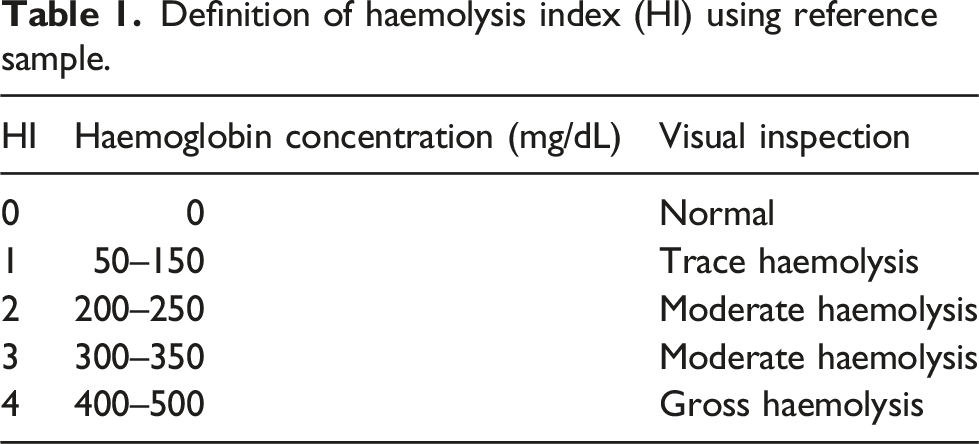
Measurement of the haemolysis index (HI)
Definition of haemolysis index (HI) using reference sample.
Measurement of the serum aspartate aminotransferase level
The serum aspartate aminotransferase (AST) level was evaluated by the method of the International Federation of Clinical Chemistry and Laboratory Medicine using the LABOSPECT 008α. The reference range was 13 to 30 U/L.
Measurement of the serum lactate dehydrogenase level
The serum lactate dehydrogenase (LD) level was evaluated by the method of the International Federation of Clinical Chemistry and Laboratory Medicine using the LABOSPECT 008α. The reference range was 124 to 222 U/L.
Measurement of the serum potassium level
The serum potassium level was evaluated by the ion selective electrode method using the LABOSPECT 008α. The reference range was 3.6 to 4.8 mmol/L.
Collection of patient data to assess the frequency of haemolysis
Data from patients were collected using a diagnostic support system (DSS; Abbott Japan, Tokyo, Japan) linked to the laboratory information system, allowing researchers to extract laboratory datasets based on the specific criteria they indicate. Data were extracted from outpatients only, and patients younger than 18 years of age were excluded from the study. We collected and analysed data from the 1-year period before and the 1-year period after the change was made to stop using the 22-gauge needles. In patients from whom blood was drawn, but no serum was collected, determination of the HI value was not possible; as a result, 28,704 patients and 28,518 patients from the periods before and after the change, respectively, were excluded from the analysis of haemolysis.
Collection of patient data to evaluate the effects of haemolysis associated with the change in the needles on the laboratory data
We used the DSS to identify patients who had an HI of 0 or 1 (normal to trace haemolysis) in the 90 days prior to the needle change and an HI of 2 or greater (moderate to gross haemolysis) by 90 days after the needle change. Only the data of patients over the age of 18 years with an estimated glomerular filtration rate (eGFR) of 45 or greater were included.
Statistical analysis
We performed statistical analyses using EZR version 1.52 statistical software. 5 The risk ratio for the frequency of persistent pain was calculated as follows: ([number of patients with persistent pain after the change]/[number of venipunctures after the change])/([number of patients with persistent pain before the change]/[number of venipunctures before the change]). The risk ratio for the frequency of haemolysis was calculated in the same manner. Fisher’s exact test was used for the analysis of categorical variables, and one-sided P-values were employed. The Wilcoxon’s signed rank sum test was used to compare the data for each laboratory parameter before and after the needle change. Values of p < 0.05 were considered to indicate statistical significance.
Results
Incidences of persistent pain and neuropathic pain
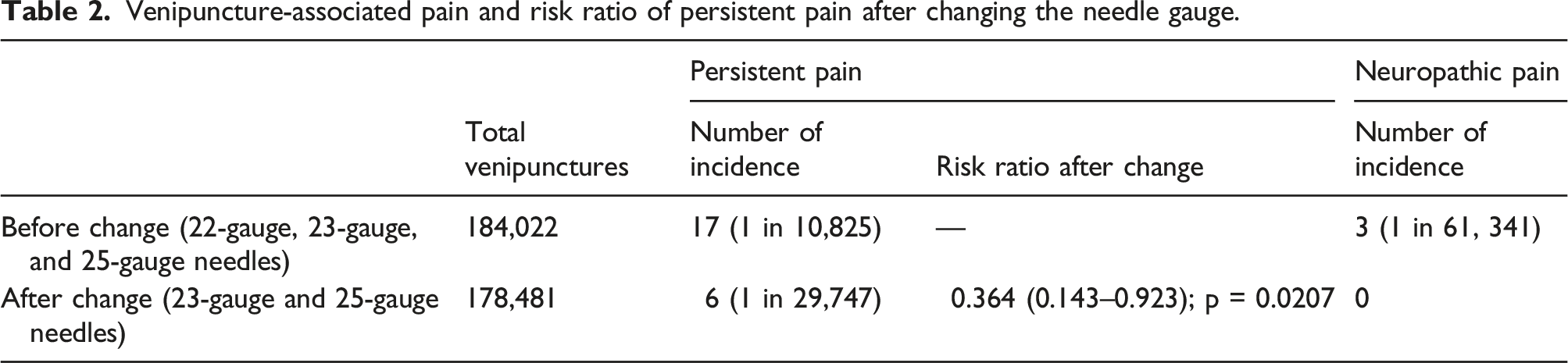
Venipuncture-associated pain and risk ratio of persistent pain after changing the needle gauge.
Frequency of haemolysis
Prevalence of haemolysis before and after the change in needle gauge and risk ratios after the change.

HI: haemolysis index.
Effects of haemolysis associated with the needle change on the laboratory data
The DSS selected 90 patients who had an HI of 0 or 1 (normal to trace haemolysis) within 3 months prior to the change and an HI ≥ 2 (moderate to gross haemolysis) within 3 months after the change. The median age of these 90 patients was 64.5 years (range, 21 to 90 years), and 42 of them were male. The median interval between the venipunctures before and after the change was 84 days (range, 21 to 154 days).
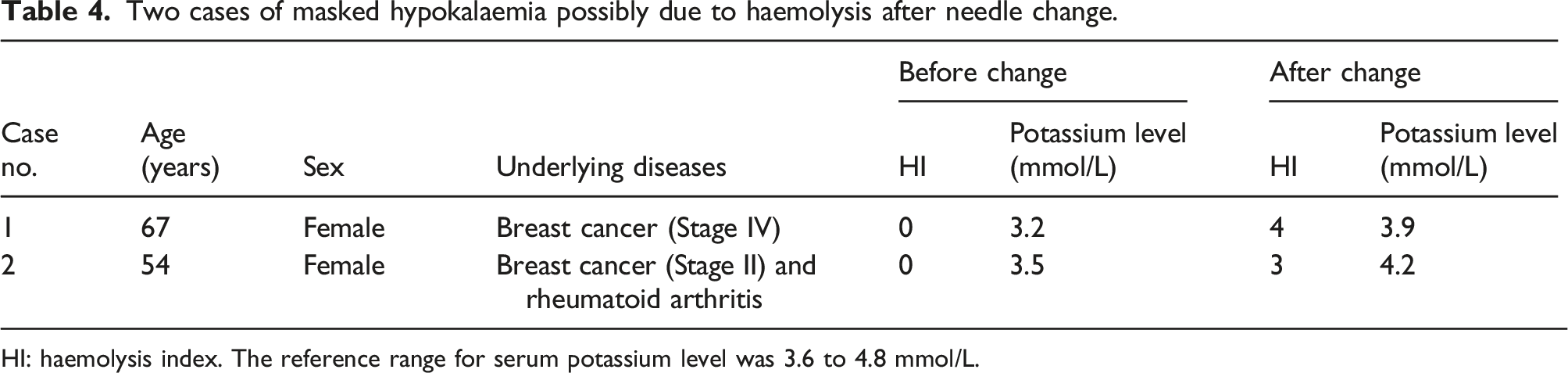
The effects of haemolysis occurring before and after the change in these 90 patients were examined. As shown in Figure 1, the serum AST, LD, and potassium levels all increased significantly after the change. Additionally, two patients had low serum potassium levels (3.2 and 3.5 mmol/L) before the needle change, but the levels were within the reference range after the change (Table 4). Hypokalaemia may have been masked by haemolysis after the needle change in these two cases. Focused analysis of the laboratory data from 90 cases that showed significant haemolysis after the needle change. The box and whisker diagrams show the medians and interquartile ranges. The points represent outliers. Significant increases were seen in the serum aspartate aminotransferase levels (a), lactate dehydrogenase levels (b), and potassium levels (c) after the change; these increases may have resulted from the increased haemolysis. Two cases of masked hypokalaemia possibly due to haemolysis after needle change. HI: haemolysis index. The reference range for serum potassium level was 3.6 to 4.8 mmol/L.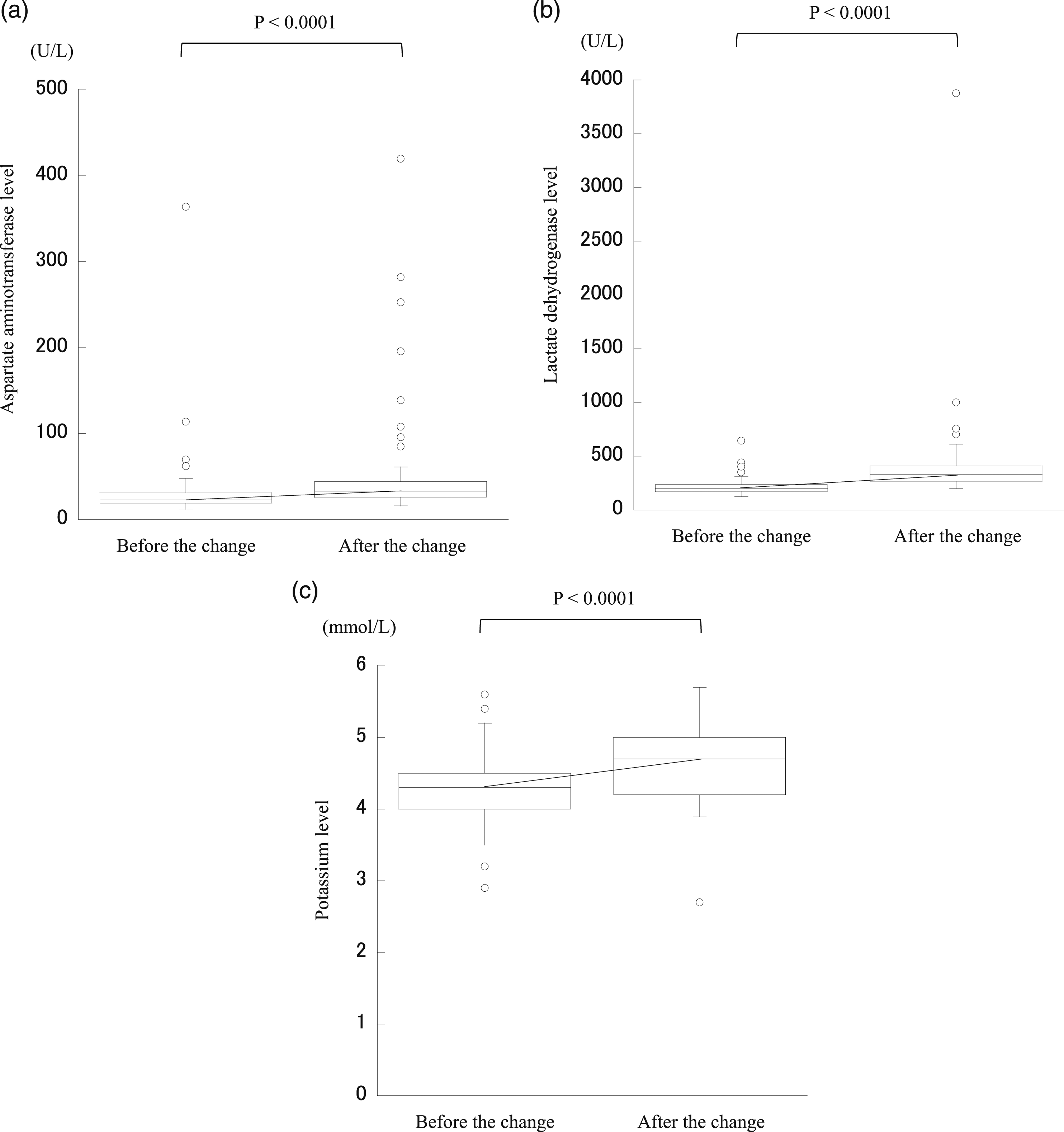
Discussion
In the present study, we retrospectively analysed cases of venipuncture and found that discontinuing the use of 22-gauge needles reduced the incidences of persistent pain and neuropathic pain but increased the frequency of haemolysis, indicating that there are both advantages and disadvantages to changing to finer needles for venipuncture.
Kato et al. previously performed an observational study on blood sampling at our hospital and reported that the incidence of persistent pain was 1 in 4,418 venipunctures, while that of neuropathic pain was 1 in 30,923 venipunctures. 4 In accordance with the report by Kato et al., we have avoided performing venipunctures from the basilic or median cubital vein and used the cephalic vein as often as possible since 2013. Consequently, the incidences of persistent pain and neuropathic pain decreased to 1 in 10,825 and 1 in 61,341 venipunctures, respectively, before the use of 22-gauge needles was discontinued. After the needle change, the incidence of persistent pain further decreased to 1 in 29,747 venipunctures, and no case of neuropathic pain was encountered (Table 2). Tsukuda et al. recently conducted an observational study of venipuncture data from more than one million patients collected over a 10-year period and reported that the frequency of neuropathic pain with the use of 21-, 23-, and 25-gauge needles was 1 in 67,000, 6 which is almost the same as the frequency we found with the use of 22-, 23-, and 25-gauge needles before the change. For insulin injections and arterial blood sampling and collection, the needle size has been reported to affect the pain felt by patients.7,8 Taken together, these findings indicate that the selection of a radial site for venipuncture and the use of a finer needle are likely to reduce the risk of persistent pain and nerve injury.
Although errors can occur in any phase of laboratory testing, the preanalytical phase is the main source of errors.9–12 Among problems during the preanalytical phase, in vitro haemolysis is the most frequent and serious one that can compromise the reliability of various test results.11–15 Lippi et al. surveyed the frequency of haemolysis at different blood collection divisions within a single hospital and found that the frequency varied greatly between divisions. 16 Cadamuro et al. showed that the frequency of haemolysis decreased significantly when phlebotomy duties were transferred from 70 untrained physicians to 874 trained nurses, indicating the importance of phlebotomy training. 17 Burns et al. analysed various factors related to blood collection and the methods that resulted in the least haemolysis and revealed that a 20-gauge needle was less likely to cause haemolysis than a 22-gauge needle. 18 Lippi et al. also compared 21-, 23-, and 25-gauge needles and showed that 23-gauge needles, when used correctly, did not significantly affect various laboratory parameters related to haemolysis when compared to 21-gauge needles, whereas 25-gauge needles resulted in greater variability in the potassium level than 23-gauge needles. 19 As described above, in vitro haemolysis is influenced by various factors, but regarding the bore size of needles, a finer needle is more likely to result in haemolysis. The present study showed that the use of 23- and 25-gauge needles significantly increased the frequency of haemolysis when compared to the use of 22-, 23-, and 25-gauge needles in a large sample size. Of particular note, the frequency of severe haemolysis tended to be higher when only 23- and 25-gauge needles were used (Table 3).
Haemolysis is known to affect various laboratory data. Our analysis focusing on 90 cases showed that the serum AST, LD, and potassium levels were significantly affected by haemolysis, similar to previous reports.20,21 In our hospital’s electronic medical records, a warning about haemolysis is included for each of the AST, LD, and potassium values in cases with an HI ≥ 2. However, in the 90 cases, blood was never drawn again despite haemolysis. If haemolysis caused the AST, LD, and potassium levels to be higher than the reference ranges, physicians would notice. However, they cannot notice it if hypokalaemia is masked by haemolysis. Practically, among the 90 cases we focused on, two cases had low serum potassium levels before the needle change, but the levels were within the reference range after the needle change (Table 4). In these two cases, the hypokalaemia before the needle change was considered to be mild, 22 and a review of the medical records did not reveal any clear symptoms that were caused by hypokalaemia. However, our results indicate the possibility that severe hypokalaemia may be overlooked in cases with intense haemolysis.
Mansour et al. reviewed 12 articles and reported that the increase in serum potassium concentration per 100 mg/dL of serum haemoglobin due to haemolysis ranged from 0.21 mEq/L to 0.50 mEq/L (median, 0.31 mEq/L). 23 Based on the results in Table 1, we estimated that the serum haemoglobin concentration would increase by about 100 mg/dL for every 1-unit increase in the HI. Therefore, an increase in the HI of 1 would result in an increase in the serum potassium concentration by about 0.31 mEq/L. Although it is unknown exactly how many episodes of hypokalaemia were missed among the 2,476 cases with an HI ≥ 2 during the 2 years examined in this study, it is possible that a significant number of them may have been masked by haemolysis.
There are limitations to the present study. The first is that it was retrospective in nature. Second, there is a limitation to the method used for validating the effects of haemolysis on the laboratory data. For strict evaluations, laboratory data should be obtained from paired serum samples taken from each patient at the same timepoints using the thicker and finer needles. However, this is not feasible in clinical practice. As an alternative to paired sampling, we used data from cases that showed significant haemolysis after the needle change and compared the data from before and after the change.
Conclusion
In summary, discontinuing the use of 22-gauge needles clearly reduced the risk of persistent pain and neuropathic pain. However, the frequency of haemolysis increased. It is very difficult to decide whether the advantage of reduced persistent pain, including neuropathic pain, or the disadvantage of increased haemolysis is more important. Our hospital has not resumed the use of 22-gauge needles because we want to reduce the risk of iatrogenic injury in patients as much as possible and to reduce the psychological burden on the clinical laboratory technologists, who perform the venipunctures. Nonetheless, the increase in haemolysis is an issue that cannot be ignored, and it is necessary to continue to accumulate evidence on the preanalytical errors that haemolysis may cause and to provide more knowledge to physicians on the matter. It is especially important to remember that hypokalaemia may be overlooked due to haemolysis. It should be noted that, recently, needles with a smaller outer diameter, but the same inner bore size, have been developed, and the use of these needles has been shown to reduce pain during venipuncture without increasing haemolysis.24,25 It may be preferable to use such needles in the future.
Footnotes
Acknowledgements
This study was conducted as part of a collaboration with Abbott Japan, Inc.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: The Division of Laboratory Medicine, Department of Pathology and Microbiology, Nihon University School of Medicine, annually received research funding of 300,000 yen from Abbott Japan, Inc.
Ethical approval
The Ethics Committee of Nihon University Itabashi Hospital approved the present study (no. RK-190212-5).
Guarantor
TN.
Contributorship
HU, HT, and TN designed the study. HU and HT collected the data. YF, HS, RA, and NT were instrumental in the implementation and maintenance of the DSS system. HU performed the review of medical records and the statistical analysis. HU and TN drafted the manuscript. All authors revised the manuscript and approved the final version of the article.