
Abstract
Introduction
Purple Urine Bag Syndrome (PUBS) is a rare disorder seen in elderly persons, wherein the urinary bag and the tubing turn in to purple colour. It is usually seen in patients who are on urinary catheters for a long time. It consists of a change in the colour of the urine that turns purple in a very specific context.
Case report
We report the case of a paediatric female patient with Berdon Syndrome with symptoms consistent with urinary tract infection and purple urine discolouration. Urine test revealed leukocyturia and bacteriuria.
Discussion
Several risk factors have been proposed regarding this syndrome. Among them the commonest are female gender, advanced age, kind of diet (increased dietary tryptophan), alkaline urine and diverse situations that leads to urinary retentions which allows bacteria to work on their substrate for a longer time. Although it is a process that is not associated with gravity, recognizing it is important as treatment is simple and can minimize patient and family distress.
Keywords
Introduction
Since historic times, urine has been used as a primary diagnostic tool. Thereby, urine appearance could provide important information related to several medical conditions. There are several causes of altered colouration of urine, both pathological and benign, such as some food, drugs, food dyes, haematuria or urinary tract infections (UTIs). Purple Urine Bag Syndrome (PUBS) is a rare but very striking entity for its clinical presentation. It consists of a change in the colour of the urine that turns purple in a very specific context. 1 Several risk factors have been proposed regarding this syndrome. Among them the commonest are female gender, advanced age, kind of diet (increased dietary tryptophan), alkaline urine and diverse situations that leads to urinary retentions which allows bacteria to work on their substrate for a longer time, such as constipation. 2 Although it is a process that is not associated with gravity, recognizing it is important as treatment is simple and can minimize patient and family distress.
Case report
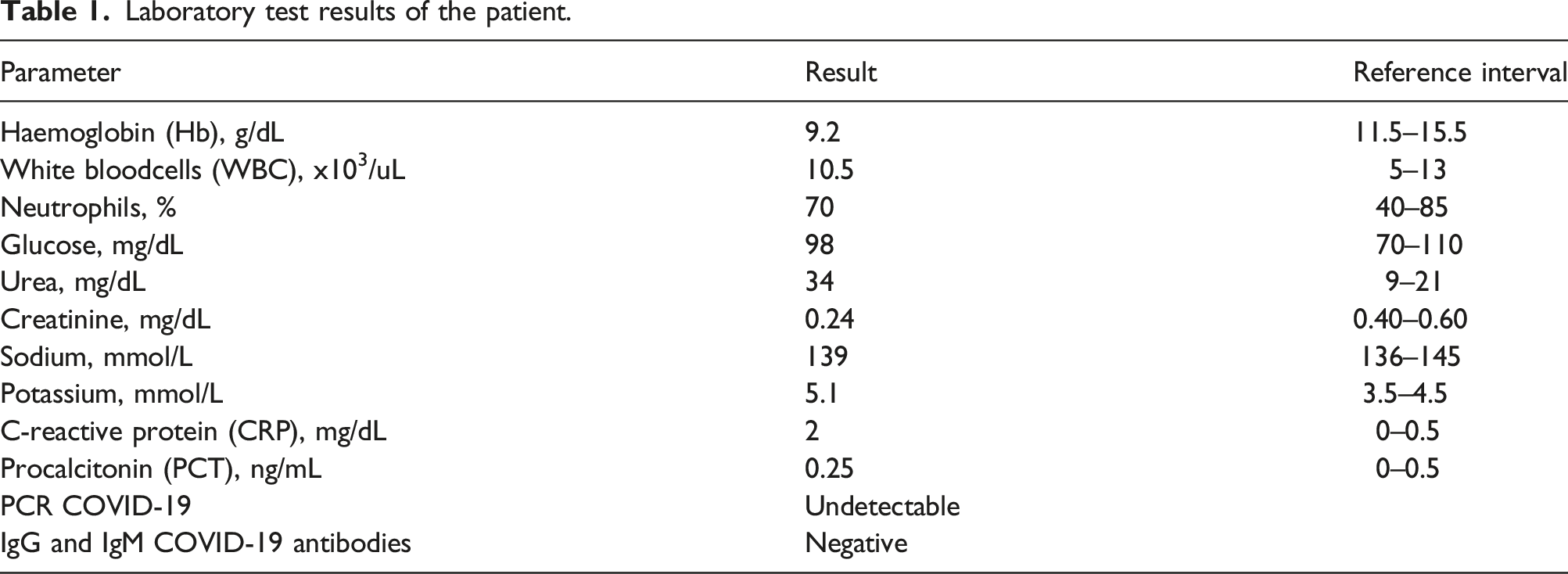
Laboratory test results of the patient.
Discussion
PUBS is a rare entity first described in 1978,
3
after purple urine was found in a patient who had prolonged urinary catheterization. It can be highly concerning and distressing for patients, relatives and clinicians. There are many reasons why elderly people are highly predisposed to the syndrome. Old age is associated with lots of comorbidities, among them dementia, constipation and renal failure can represent independent risk factors for PUBS.
4
In terms of gender, it seems that PUBS affects women predominantly. This is mostly explained as female urethra is particularly prone to colonization by colonic gram negative bacilli, owing to its proximity to the anus, its short length and its termination beneath the labia.
5
Contrariwise, male specific factors such as zinc, a potent antibacterial agent that is secreted by the prostate, may act protectively.
6
The clinical presentation consists of a change in the urine colour, which appears in various shades, between blue, violet and purple. Usually this syndrome comes as a result of UTIs even in the absence of dysuria or fever.
7
The postulated hypothesis regarding etiopathogenesis of PUBS involves a sequence of reactions beginning with dietary intake of tryptophan. This amino acid is transferred in the large intestine in order to be metabolized into indole by gut microbiota in a deamination process. It is rapidly diffused into the portal circulation and is conjugated to produce indoxylsulphate (indican) by the liver. Indican is secreted into urine where, under the influence of bacterial enzymes such as sulphatases and phosphatases, especially in an alkaline environment, indicant is oxidized to two pigments: indirubin (red) and indigo (blue). The mixture of those pigments is responsible for the striking purple colour in the urine
7
(Figure 1). In PUBS pathogenesis, several bacteria have been implicated: Proteus mirabilis, Pseudomonas aeruginosa, Klebsiella pneumoniae, Escherichia coli, Providencia stuartii and rettgeri, Morganella and Citrobacterspp, Enterococci and Group B Streptococci.
8
In our present case, the urine culture report shows the growth of K. oxytoca. These bacteria were found to be the cause of PUBS in 0.6% of the cases, according to a comprehensive review carried out by N. Sabanis et al.
7
Other causes of coloured urine such as treatment with some drugs (amitriptyline, indomethacin and propofol) or exposure to dyes (methylene blue) were investigated and discarded. Flow chart outlining the development of purple urine bag syndrome.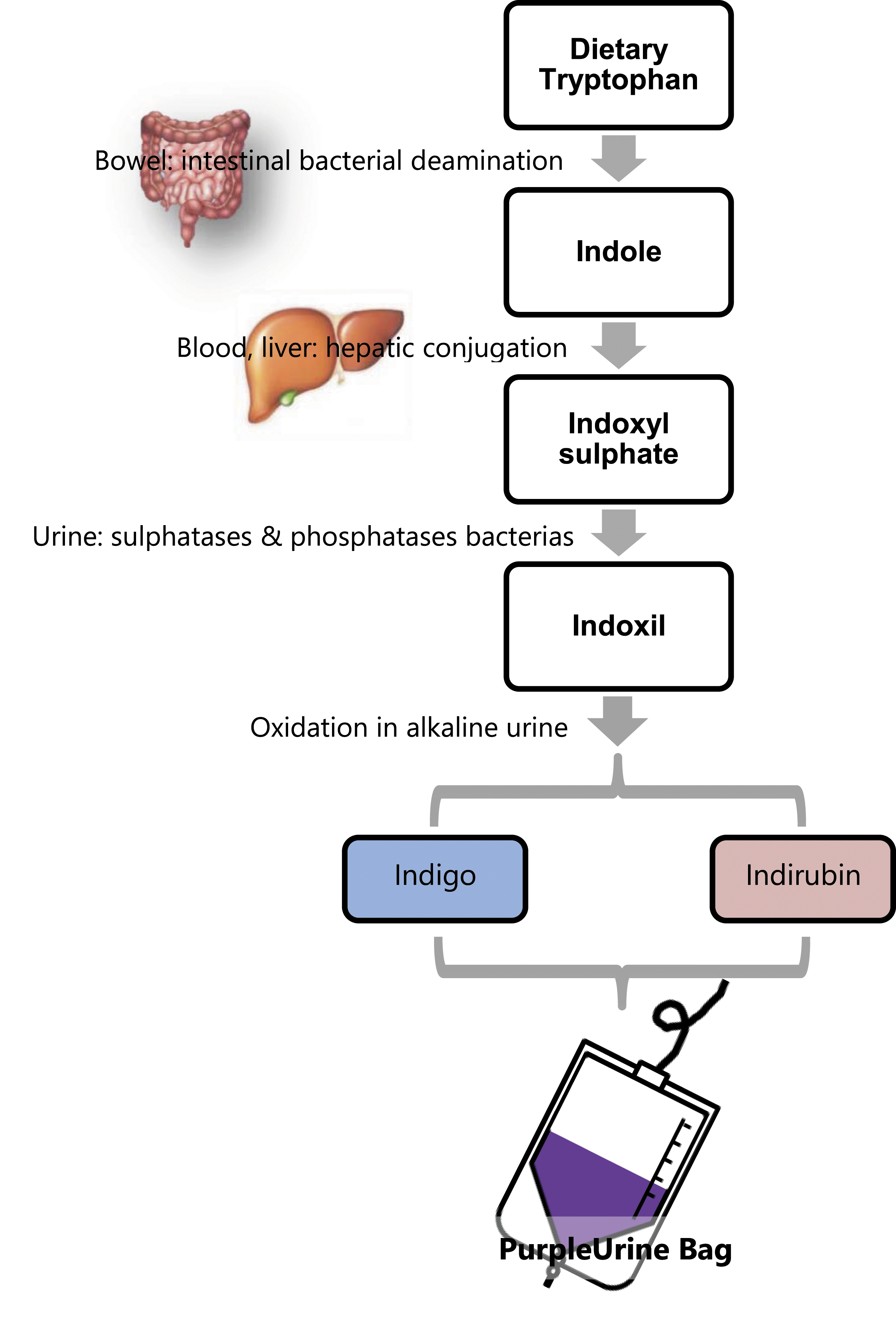
Megacystis Microcolon Intestinal Hypoperistalsis Syndrome (MMIHS), also known as Berdon syndrome, is a rare congenital disorder of gastrointestinal and urinary tract motility. 9 According to current literature (in the period 1976–2018), 450 patients with MMIHS were reported. 9 MMIHS is characterized by microcolon, intestinal hypoperistalsis, dilated small bowel loops and constipation, urinary retention, giant bladder (megacystis) and hydronephrosis. Most cases are sporadic, with a small number of familial cases with reported consanguinity, suggesting possible autosomal recessive inheritance. 10 It is usually diagnosed prenatally or affected infants present shortly after birth with symptoms of bowel and bladder obstruction. It has been found that the incidence is more common in females than males.9,11 It has been suggested by some authors that the female predominance in MMIHS may be due to a more severe form of the condition in males resulting in intrauterine death. 11 In the familial cases, there were no reported male intrauterine deaths and genders were represented across neonatal deaths, later deaths and survivors in proportion to the reported gender distribution. However, this data may not capture early intrauterine deaths of severely afflicted males. MMIHS represents the most severe form of functional intestinal obstruction and is most often a fatal diagnosis. Berdon syndrome usually results in death within the first year, with an average life expectancy of only 3.6 months. Nevertheless, some reviews published over the last few years found significant improvement in overall survival rates of MMIHS patients, going so far as to describe a 24 years old as the oldest survivor so life expectancy has been increased. 12 The main goals of treatment are providing a bladder-emptying strategy to prevent renal failure and to provide adequate nutrition to overcome gastrointestinal hypomotility. Consequently, the vast majority of Berdon patients eventually require parenteral nutrition. Multiorgan visceral or intestinal transplants have been found to be the only definitive treatment for MMIHS patients.
In this present case, the patient had showed many of the risk factors associated with PUBS (female gender, alkaline urine and constipation) linked to conditions derived from Berdon syndrome such as reduced urinary motility, which enhances longer time contact of bacteria with their substrate, and the use of HPN. Although the composition of HPN can be varied, it uses to be rich in amino acids, with tryptophan being one of the essential amino acids in humans. To our knowledge this is the first case reported of a patient diagnosed with megacystis and purple urine. It should be taken into account that the patient did not have a urinary catheter at the time of urine collection, so it is not possible to refer as bag syndrome.
1. Purple urine management 2. Urine value as a diagnostic tool 3. Berdon syndrome
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
Full ethical approval for this study was given by the Research Ethics Committee of the Principality of Asturias (Spain) and it was considered that the study was exempt from informed consent (cod CEImPA 2022.016).
Guarantor
MOR.
Contributorship
MOR and MMR researched literature and conceived the study. JDM is the patient’s physician. MOR and MMR wrote the first draft of the manuscript. BPG and JDM reviewed the manuscript. All authors edited the manuscript and approved the final version.