
Abstract
Purple Urine Bag Syndrome (PUBS) is an uncommon but notable clinical phenomenon primarily observed in patients with long-term indwelling catheters. This syndrome is characterized by a striking purple discoloration of the urine collection bag, often indicative of an underlying urinary tract infection (UTI) and associated metabolic processes. PUBS occurs due to the breakdown of indoxyl sulfate, a tryptophan metabolite, by specific bacteria present in the urinary tract. In this report, we present the case of a 73-year-old female with a chronic Foley’s catheter, later developed PUBS, accompanied by symptoms of lower abdominal pain, fever, and reduced urine output. Urine culture identified Klebsiella pneumoniae, a common uropathogen, as the causative organism. This case highlights the clinical presentation, pathophysiology, and management of PUBS in a patient with long-standing catheterization, along with a brief review of existing literature on the condition. Prompt recognition and targeted antibiotic therapy, alongside supportive measures, were essential in managing the infection and alleviating symptoms.
Introduction
Purple Urine Bag Syndrome (PUBS) is an uncommon but notable clinical phenomenon that manifests as a violet or purple discoloration of the urine collection bag in patients with indwelling urinary catheters. 1 First documented in the 1970s, PUBS is typically observed in elderly, bedridden patients, often in conjunction with chronic urinary tract infections. Although the condition is benign, its presence can be alarming and may signal an ongoing infection or imbalance in urinary tract metabolism.2,3
PUBS remains uncommon, affecting an estimated 2% to 9% of long-term catheterized patients but reported infrequently in routine practice. Fewer than 150 cases have been published to date, and only a handful implicate Klebsiella pneumoniae as the sole pathogen in a symptomatic elderly patient. This rarity emphasizes the importance of documenting antimicrobial resistance patterns and clinical features in each new report. The risk factors for PUBS include advanced age, female sex, constipation, alkaline urine pH, and prolonged catheterization. Common causative organisms include Klebsiella pneumoniae, Providencia spp., and Escherichia coli, which produce enzymes that degrade indoxyl sulfate into purple-colored pigments.1,3 Despite the condition’s distinctive presentation, PUBS is frequently overlooked, as it is usually asymptomatic or associated with mild symptoms of urinary tract infection. In this case report, we discuss a case of PUBS in a 73-year-old female with a long-standing Foley’s catheter.
Case Presentation
A 73-year-old female presented to the General Medicine Outpatient Department with concerns regarding a discoloration of her urethral catheter and its collection bag, which she noticed about 15 days ago. She also reported experiencing lower abdominal pain for the past 10 days, fever for 7 days, and a decrease in urine output over the last 5 days.
Her medical history, revealed that she had left hip intertrochanteric fracture, which was treated with proximal femoral nailing. She managed to ambulate for about a month following the surgery but subsequently stopped walking due to increasing pain. For the past 3 years, she has had an indwelling Foley’s catheter. She has no history of diabetes, hypertension, bronchial asthma, pulmonary tuberculosis, coronary artery disease, chronic kidney disease, cerebrovascular events, or allergies to foods or medications. Her personal history includes chronic constipation, but her sleep and appetite remain unaffected. She has no history of smoking or alcohol consumption.
Upon examination, the patient appeared moderately built and nourished, with stable vital signs. A Foley’s catheter was present, and the urine collection bag displayed a distinct purple discoloration, characteristic of purple urine bag syndrome (PUBS) (Figure 1). Systemic examination revealed that her cardiovascular system was normal, with S1 and S2 heart sounds present and no audible murmurs. Neurological assessment indicated a Glasgow Coma Scale score of 15/15, with no focal deficits. Her respiratory system showed bilateral normal vesicular breath sounds. Abdominal examination identified mild tenderness in the hypogastric area, and bowel sounds were present. Laboratory and radiological investigations were performed (Table 1). Biochemical tests revealed that, her serum creatinine was 0.8 mg/dL, and random blood sugar was 128 mg/dL. Her complete blood picture (CBP) indicated a total white cell count of 13 800 cells/μL with neutrophilia, while her hemoglobin was measured at 12 g/dL. An ultrasound of the abdomen and pelvis suggested chronic cystitis.

Foley’s catheter and the urine collection bag displayed a distinct purple discoloration, characteristic of purple urine bag syndrome (PUBS).
Urine Routine Examination (Physical and Biochemical).

Routine urine examination revealed amber-colored, slightly cloudy urine with a specific gravity of 1.015 and a pH of 6.5. Biochemical analysis of the urine showed mild proteinuria (50 mg/dL), no glucose or ketones, urobilinogen at 3.0 mg/dL, and negative results for bile pigments and ascorbic acid. Microscopic examination detected 11 to 20 pus cells per high-power field (HPF) and 0 to 2 epithelial cells per HPF. Urine culture identified Klebsiella pneumoniae with a significant colony count of >10⁵ CFU/mL. Antibiotic susceptibility testing showed that the bacteria were sensitive to Amoxicillin-clavulanic acid, Piperacillin, Tazobactam, cefotaxime, and Amikacin but resistant to Ceftazidime, Ciprofloxacin, and Nitrofurantoin.
Based on the clinical and laboratory findings, a diagnosis of purple urine bag syndrome secondary to a chronic urinary tract infection caused by Klebsiella pneumoniae was made. The patient initially received piperacillin–tazobactam 4.5 g intravenously every 8 hours, adjusted for renal function, followed by oral amoxicillin–clavulanic acid 625 mg every 8 hours after clinical improvement and culture-directed step-down therapy. Oral vitamin C was prescribed to acidify the urine and potentially reduce bacterial growth. Additionally, her Foley’s catheter and urine collection bag were replaced with silicone versions to minimize recurrence of the syndrome.
Discussion
Purple Urine Bag Syndrome (PUBS) is a rare clinical phenomenon that manifests as a striking purple discoloration of urine in patients with indwelling urinary catheters. This condition is primarily associated with urinary tract infections (UTIs) caused by specific bacteria, notably Klebsiella pneumoniae, Proteus mirabilis, and Pseudomonas aeruginosa, which possess the enzymatic capability to metabolize indole derivatives into pigments that react with the plastic of the catheter and urine bag, resulting in the characteristic purple hue. 4 The pathophysiology of PUBS involves the conversion of tryptophan to indole, which is subsequently oxidized to indoxyl sulfate (Figure 2). In the presence of alkaline urine, this compound is hydrolyzed by bacterial enzymes, leading to the formation of indigo (blue pigment) and indirubin (red pigment). 5 When these pigments come into contact with the plastic materials of the catheter and urine collection bag, they produce the distinctive purple coloration observed in PUBS.4,5 Despite divergent biochemical traits (lactose fermentation, oxidase status, H₂S production), Klebsiella, Proteus, Pseudomonas, and E. coli all express indoxyl sulfatase/phosphatase, enabling conversion of indoxyl sulfate into indigo and indirubin pigments under alkaline urinary conditions.4,5 Other causes of urine discoloration include drug pigments (phenazopyridine, rifampicin), dietary factors (beet ingestion), metabolic disorders (porphyrins in porphyria), and chemical exposures. PUBS is distinguished by purple bag discoloration with underlying amber fluid.2,5

Pathophysiology of Purple Urine Bag Syndrome (PUBS).
The occurrence of PUBS is often seen in elderly patients, particularly those with long-term catheterization, chronic constipation, and underlying comorbidities. 6 Factors such as alkaline urine, which can result from urinary tract infections, further predispose patients to this syndrome. 7 Microscopy revealed 11 to 20 pus cells/HPF, 0 to 2 epithelial cells/HPF, and no crystals. While triple-phosphate or uric acid crystals may accompany alkaline urine in some PUBS cases, our patient’s sediment was crystal free. While PUBS is generally considered benign and asymptomatic, it can serve as an important clinical indicator of underlying urinary tract infections, which may require prompt evaluation and management. 8 The presence of PUBS should prompt healthcare providers to investigate for potential urinary tract infections, as the syndrome may be a sign of significant bacterial colonization within the urinary system.6,8
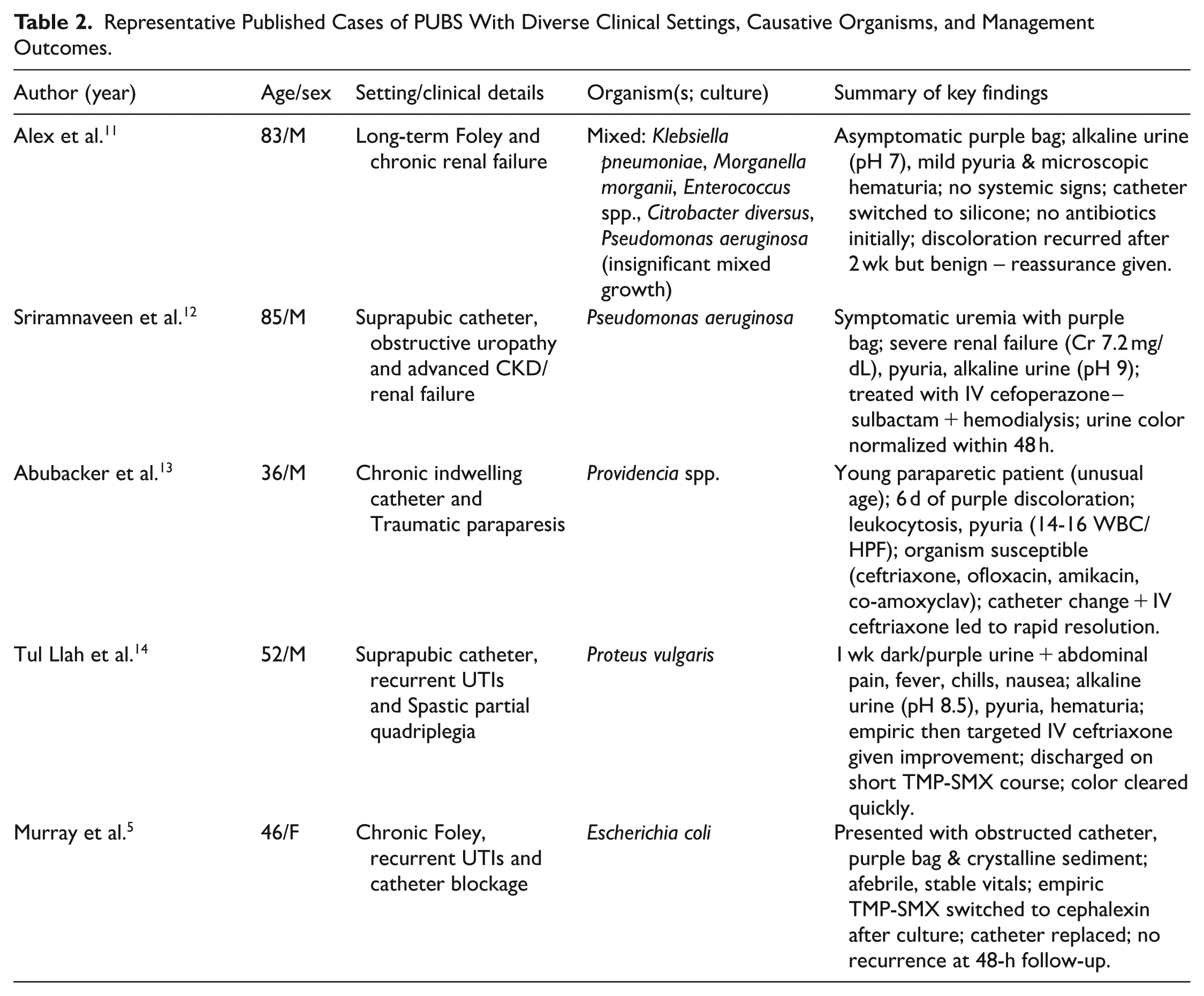
Several studies have documented the relationship between PUBS and urinary tract infections (Table 2). For instance, Keer et al. reported cases of PUBS in elderly men with UTIs, highlighting the role of indoxyl phosphatase and sulfatase enzymes produced by specific bacteria. 7 Similarly, Agbor et al. described PUBS in an elderly female patient, emphasizing the importance of recognizing this syndrome as a potential marker for urinary tract infections. 9 Moreover, a systematic review by Llenas-García et al. consolidated various cases of PUBS, reinforcing the association between this syndrome and bacterial infections in catheterized patients. 8 Another systematic review by Yang et al. (116 analyzed cases, 1991-2016) show PUBS predominantly affects elderly patients (mean age ~76; 84.5 % ⩾ 65 years) with a female preponderance (≈60%) and alkaline urine in 93% of cases. Mortality was low overall (6.8%) and declined to 4.3% in 2011 to 2016, despite progressively higher reported leukocyte counts, suggesting improved early recognition and antimicrobial management. 10 These epidemiologic trends reinforce the need for vigilant frontline detection and prompt, targeted therapy rather than dismissing PUBS as purely benign.10-14
Representative Published Cases of PUBS With Diverse Clinical Settings, Causative Organisms, and Management Outcomes.
Management of PUBS typically involves addressing the underlying urinary tract infection through appropriate antibiotic therapy and catheter care. Our Klebsiella isolate demonstrated resistance to ceftazidime, ciprofloxacin, and nitrofurantoin – agents commonly used in UTIs, yet remained susceptible to β-lactam/β-lactamase inhibitors. This highlights evolving resistance in catheterized patients and supports early culture-driven de-escalation to preserve effective therapies. 15 In cases where the patient is asymptomatic, treatment may focus on improving catheter hygiene and managing risk factors such as constipation. 16 However, in symptomatic cases, timely antibiotic intervention is crucial to prevent complications associated with urinary tract infections, including sepsis and renal impairment.15,16
Despite its detailed clinical presentation and management, this case report has limitations inherent to its format. As a single case report, the findings are not generalizable to the broader population of catheterized patients with UTIs. We are unable to establish a direct causal link between Klebsiella pneumoniae and the PUBS phenomenon based on a single patient observation. Furthermore, the lack of detailed urine pH monitoring over the course of the infection limits our ability to fully correlate urine alkalinity, a known risk factor, with the clinical manifestation and resolution of PUBS.
Conclusion
In conclusion, while PUBS may appear as a benign and visually striking phenomenon, it is essential for healthcare providers to recognize its potential implications as a marker for urinary tract infections in catheterized patients. Awareness of PUBS can facilitate timely diagnosis and management of underlying infections, ultimately improving patient outcomes. Empowering nurses, long-term care staff, and family caregivers to recognize early purple discoloration, obtain cultures, replace the catheter, and facilitate timely, evidence-based antibiotic selection enables stewardship through rapid de-escalation. Future research should focus on further elucidating the mechanisms behind PUBS and developing evidence-based guidelines for its management in clinical practice.
Footnotes
Ethical Considerations
No ethical approval was required for case reports as per our university guidelines, informed consent from patient/guardian is enough and the same was obtained.
Informed Consent
Written Informed consent was obtained from the patient for the research and the publication.
Authors Contributions
Botuku S. – Idea, conceptualization, supervision, writing draft, approved final draft.
Garre S.M.K. – conceptualization, Supervision, writing draft and revision of draft, approved final draft.
Muppavarapu R.S. – resources, visualization, writing draft and revision of draft, approved final draft.
Yedida N. & Gundraju S. – resources, writing draft and revision of draft, approved final draft.
Suvvari T.K. & Singh T. – conceptualization, resources, Project administration, writing draft and revision of draft, approved final draft.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.