
Abstract

Dear Editor,
Establishing an accurate reference interval (RI) is crucial for the diagnosis of thyroid disorders. CLSI and IFCC guidelines for RI determination stipulate various requirements, i.e., a truly healthy subject sample that must include a minimum of 120 values. 1 It can therefore be challenging for individual laboratories to develop their own RIs for thyroid hormones. We describe the alternative approach for determining a RI for Free Thyroxine (fT4) by using an indirect method for computing reference ranges. The procedure is relatively simple and employs data collected in the same pre-analytical condition and from the same population for which the limits will be used. Although indirect methods do not follow the guidelines for the production of RI, they could be utilized to confirm a previously adopted RI. Moreover, they could be useful in the evaluation and comparison of data stratified in relation to different biological parameters, such as sex and age.
From the laboratory information system of the Laboratory Medicine Department of the Mestre Hospital, 102,102 records with both fT4 and thyroid-stimulating hormone (TSH) requests were selected, for the period December 2016 to December 2019.
Results from the following patient groups were excluded: inpatients, samples from patients in retirement homes, pre-admission and day hospital patients (15,501 records). Next, results from the following were further excluded: those with TSH outside the existing TSH RI 2 (15,469 records), those of patients with more than one fT4 determination within the period of observation (43,320) and those of patients less than 18 years old (1671). Lastly, the outliers were eliminated according to the iterative 4 SD rule (140 records). A total of 26,001 patients were finally evaluated.
fT4, fT3 and TSH were respectively determined by Access Free T4, Access Free T3 and Access TSH (3rd IS) chemiluminescence two steps assays, performed using the automated DxI platform (Beckman Coulter, Inc., Brea, CA, USA), according to the manufacturer’s instructions.
Battacharya analysis was performed using the ‘Bellview Bhattacharya analysis’ (https://sourceforge.net/projects/bellview/). 3 Other statistical analyses were performed with MedCalc © Software, Version 7.4.2.0 (MedCalc Software, Mariakerke, Belgium).
The descriptive statistics of the 26,001 selected cases, subdivided by sex and age are shown (Table 1). Males showed significantly higher fT4 concentrations than females (Kruskal-Wallis test P < 0.001).
fT4 Concentrations in the overall population and by gender and age.
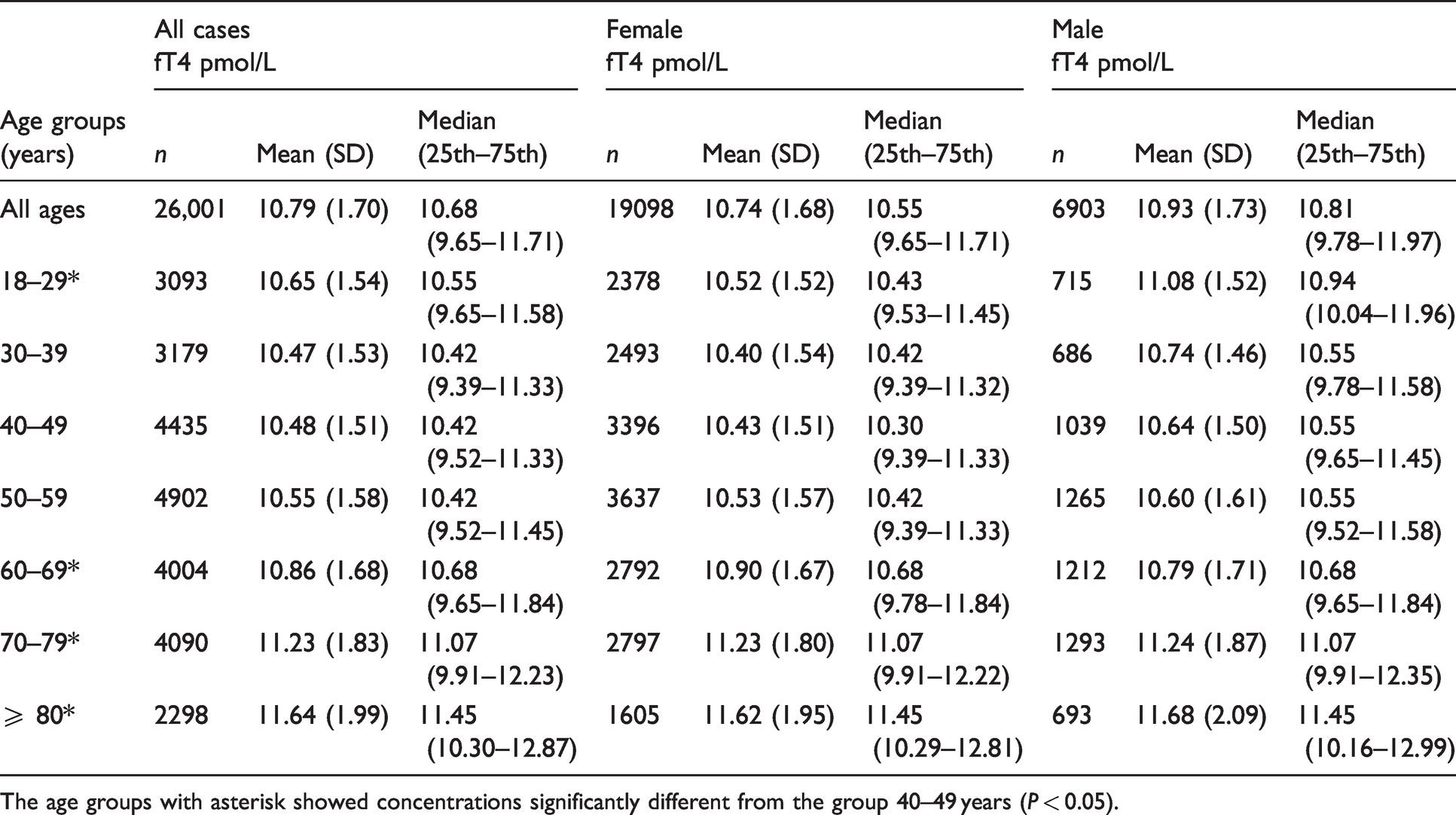
The age groups with asterisk showed concentrations significantly different from the group 40–49 years (P < 0.05).
The fT4 RI obtained by Bhattacharya analysis was 7.93–14.69 pmol/L, very similar to that stated by the manufacturer (7.86–14.41 pmol/L). Although there was a statistically significant difference in concentration between the sexes, this was small and the RIs were virtually superimposable (7.97–14.65 and 7.88–14.74 pmol/L, respectively).
fT4 concentrations were unchanged in age groups up to 60 years but increased after this age for both females and males (Table 1). We speculate that this might be in part linked to the reduced conversion of T4 to T3 in older age. 4 Indeed, the ratio fT3/fT4, measured in the 6958 cases in which fT3 were requested, progressively decreases with age (data not shown).
Other papers have addressed the evaluation of the RIs for thyroid hormones with the Access analytical method. These studies have determined fT4 RIs for the Access platform using a direct approach, i.e., the recruitment of healthy subjects.5–7 The percentage of differences found between the highest and lowest value reported in the various published studies were almost 6% for the high reference limit and almost 10% for the low reference limit, probably due to the different geographical areas studied.
A previous indirect determination of the fT4 RI was undertaken by Wang et al. 8 although the number of cases evaluated was relatively small and the selection criteria were not clear.
To the best of our knowledge, this study estimates fT4 with the indirect method with the highest number of cases evaluated to date. The selection of outpatients without repeated measurements allowed for a more confident selection of cases from presumably healthy subjects.
The maximum difference of fT4 medians between group of ages (from group age 40–49 and group age ≥ 80) is about 10% (Table 1), compatible with the between assay analytical variability (coefficient of variation 5–6%). Therefore, the differences are not clinically significant, and there is probably no need to establish age-related RI.
Footnotes
Acknowledgements
None.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
N/A.
Guarantor
RD.
Contributorship
RD and PC researched literature and conceived the study. RD performed data extraction and statistical analysis. RD wrote the first draft of the manuscript. RD and PC reviewed and edited the manuscript and approved the final version of the manuscript.