
Abstract
Background
A patient survey developed by the Pre-Analytical Phase Special Interest Group of the Association for Clinical Biochemistry and Laboratory Medicine (ACB-PA-SIG) was conducted during November and December 2019. The survey aimed to determine the quality of information provided to patients in preparation for their blood test(s). In addition, the ACB-PA-SIG provide a number of recommendations, which, if adopted, may yield higher quality test results and improve patient management.
Methods
The survey was distributed at phlebotomy suites in two Hospitals: Ipswich Hospital (United Kingdom [UK]), and Cork University Hospital (Republic of Ireland [RoI]).
Results
Overall, 235 survey responses were received from the two sites. A total of 103 respondents received no information about preparing for their blood test and 92 had been told they did not need to fast. None of the patients surveyed had been instructed to fast for 12 h. Twenty-two patients had been told to avoid certain foods, drinks or medication, 14 were told to avoid strenuous activity and 41 respondents had been informed of the need to avoid alcohol/smoking prior to their blood test. Overall, only approximately 78 felt well informed about the blood taking process.
Conclusions
Based on the results of this survey, the ACB-PA-SIG conclude that: (1) clinicians should provide clear written information to patients regarding pre-analytical requirements; and (2) effective communication between laboratories and General Practitioners is required to disseminate information. In this paper, the ACB-PA-SIG provide a list of pre-analytical recommendations to standardize and improve practice across the UK and RoI.
Introduction
Laboratory medicine plays a crucial role in the patient management process, affecting up to 70% of clinical care decisions including those of diagnosis, treatment and monitoring.1–3 Delayed or inaccurate laboratory results may cause delayed or missed diagnoses, additional unnecessary investigations, inappropriate treatment decisions or prolonged hospital stays. All of these may negatively impact the patient experience, clinical outcome and compromise patient safety. 4 Therefore, it is vital that clinical laboratory results are of the highest possible quality.
Over the years, clinical laboratory services have been subject to increasingly more rigorous quality assessment, particularly since the introduction of ISO 15189:2012 standards. 5 However, the total testing process (TTP) still carries a significant risk of error spread across the pre-analytical, analytical and post-analytical phases. Numerous studies have demonstrated that most errors in the TTP occur in either the pre-analytical or post-analytical phases.6–9 Indeed, pre-analytical errors are estimated to account for 50–70% of all laboratory errors. These are caused by, but are not limited to, problems in patient preparation, sample collection, sample identification and suitability for analysis, as well as specimen transport and storage.8,10 The importance of blood specimen management to prevent laboratory errors has been recognized and efforts to standardize the extra-analytical phases have been made. 7 The benefits of optimizing the TTP will not be fully realized until the pre-analytical phase undergoes the same level of improvement that has been seen in the analytical phase over the past 10–15 years.5–6
Patient preparation is a critical pre-analytical issue; however, this step is often overlooked. 8 Modifiable factors such as fasting status, physical activity and therapeutic drug intake prior to blood collection may lead to significant variability in laboratory test results.9,10 General clinical chemistry and haematology tests, such as albumin, bilirubin, phosphate, calcium, magnesium, potassium and full blood count, have been shown to change significantly in concentration after consumption of even a light meal.11,12
In an ideal scenario, clinical information on the use of medicines and supplements would be obtained and there would be a standardized fasting time and time for sample collection. 8 In addition, patients would avoid abnormal strenuous activity, alcohol, caffeine and smoking for clearly defined periods before attending for their blood collection. 8 However, in the real world, information about adherence to these requirements may not always be provided, and it is not clear how many patients are aware of how these pre-analytical factors could affect their test results.
If blood samples are collected at an inappropriate time or under non-ideal conditions, a repeat blood test is often required to confirm or refute findings. This can cause patient anxiety and result in poor patient satisfaction and experience. Moreover, results produced under substandard conditions may lead to a number of different problematic scenarios: (1) erroneous results that are not obvious lead to inappropriate patient management and patients may or may not be re-bled; (2) erroneous results do not breach a clinical decision threshold, there is no change in patient management, but the patient may be re-bled to confirm or refute findings; or (3) results do not fit the clinical picture so the patient is re-bled. All scenarios lead to a financial burden on the health care economy due to extra procedures, treatments, investigations, repeated blood tests, in addition to the financial and non-financial costs to the patient.
This survey sought to assess preparative information provided to patients when attending for blood testing in two hospitals in the UK and RoI. In addition, the ACB-PA-SIG aimed to provide a number of recommendations, mirroring what is common practice in other countries, 13 which we believe would yield higher quality test results and improve patient experience. The recommendations can be communicated to GP surgeries and outpatient facilities, and be referred to in online information sites for patients and healthcare professionals such as Lab Tests Online UK (LTO-UK). 9
Materials and methods
Patient participants
The patient survey was conducted at Ipswich Hospital, a partner site of East Suffolk and North Essex NHS Foundation Trust (ESNEFT) in the UK, and Cork University Hospital (CUH), RoI. The survey was available to outpatients attending phlebotomy services as part of their standard clinical care during weekdays of November and December 2019. Patients attending phlebotomy suites were asked if they wished to complete a survey about preparing for their blood test, which was accompanied by a letter explaining the purpose of the survey. The survey consisted of a paper–pencil questionnaire to be completed by patients before the blood sample(s) were taken by a phlebotomist, participation was voluntary and confidential, and respondents were informed that data would be anonymous and untraceable. Due to the anonymous nature of the questionnaire, approval by an ethics committee was not required at either site.
The questionnaire
The questionnaire was developed by members of the ACB-PA-SIG. Questions were designed to examine patient preparation practices for blood sample collection and were not based on any defined criteria. All questions and respective answering options are shown in Table 1, where numbers of respondents have been converted into a percentage they have been rounded to whole numbers, unless they constitute <10% of participants. The response rate (RR) is provided for each question (Q) using the following notation Qx; RR=y.
Survey questions and answers.
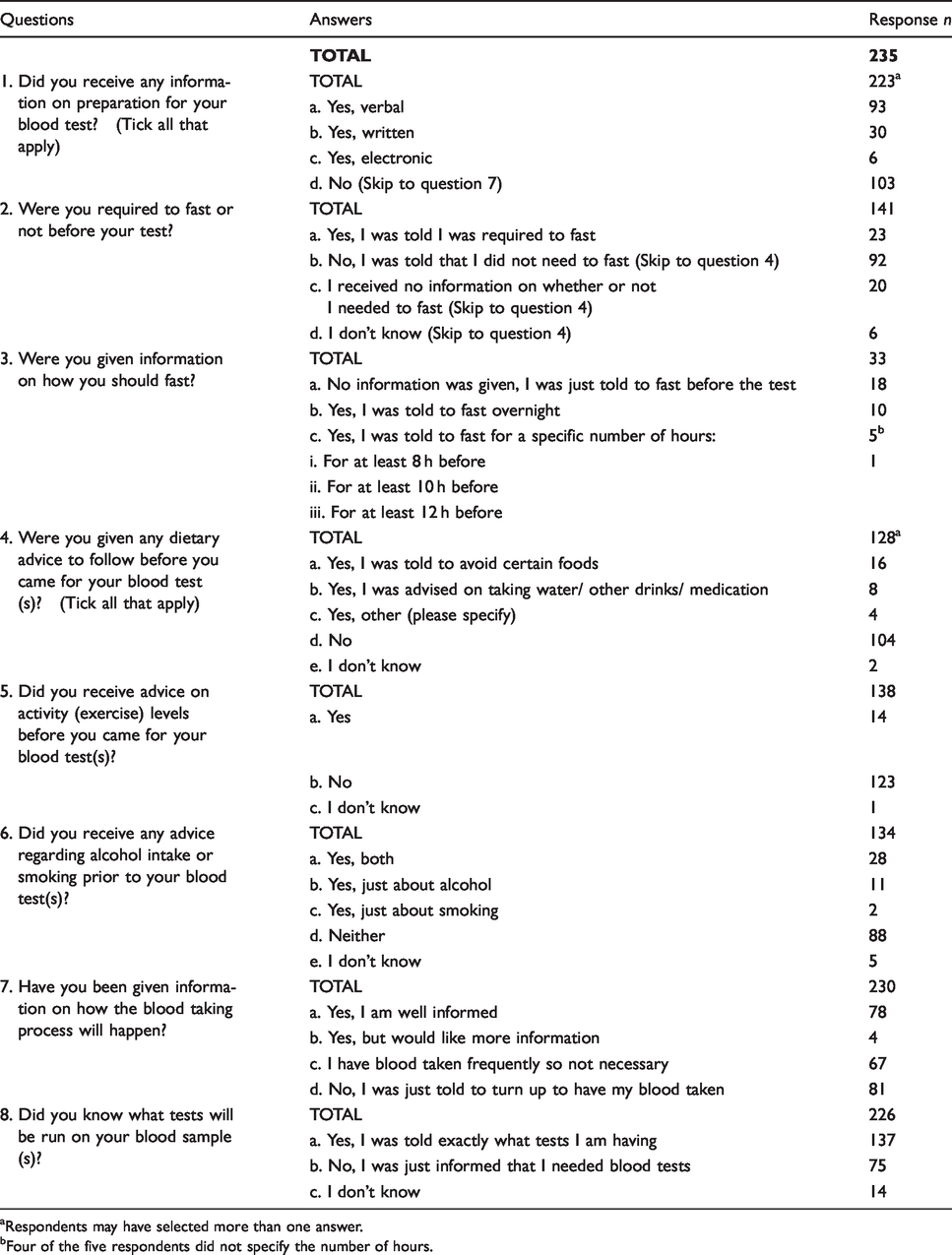
aRespondents may have selected more than one answer.
bFour of the five respondents did not specify the number of hours.
Results
Overall, 235 patients across the two sites completed the survey: 54 at ESNEFT and 181 at CUH. Q1 queried whether patients had received information in preparation for their blood test(s) (Q1; RR = 225), with n = 103 indicating that they had received no information about preparation (Figure 1(i)). However, out of the 103, n = 8 individuals contradicted their answer in subsequent responses: whether to fast or not (n = 8), to avoid certain foods (n = 1), about activity levels (n = 2) and/or advice about alcohol intake or smoking (n = 4). In addition, of the 103, n = 19 felt well informed, n = 35 had their blood taken frequently so did not think further information was necessary and n = 91 skipped from Q1 to Q7 as prompted in the survey. A total of 12 (of the 103 answering ‘No’ in Q1) disregarded the prompt and moved straight on to answer Q2.
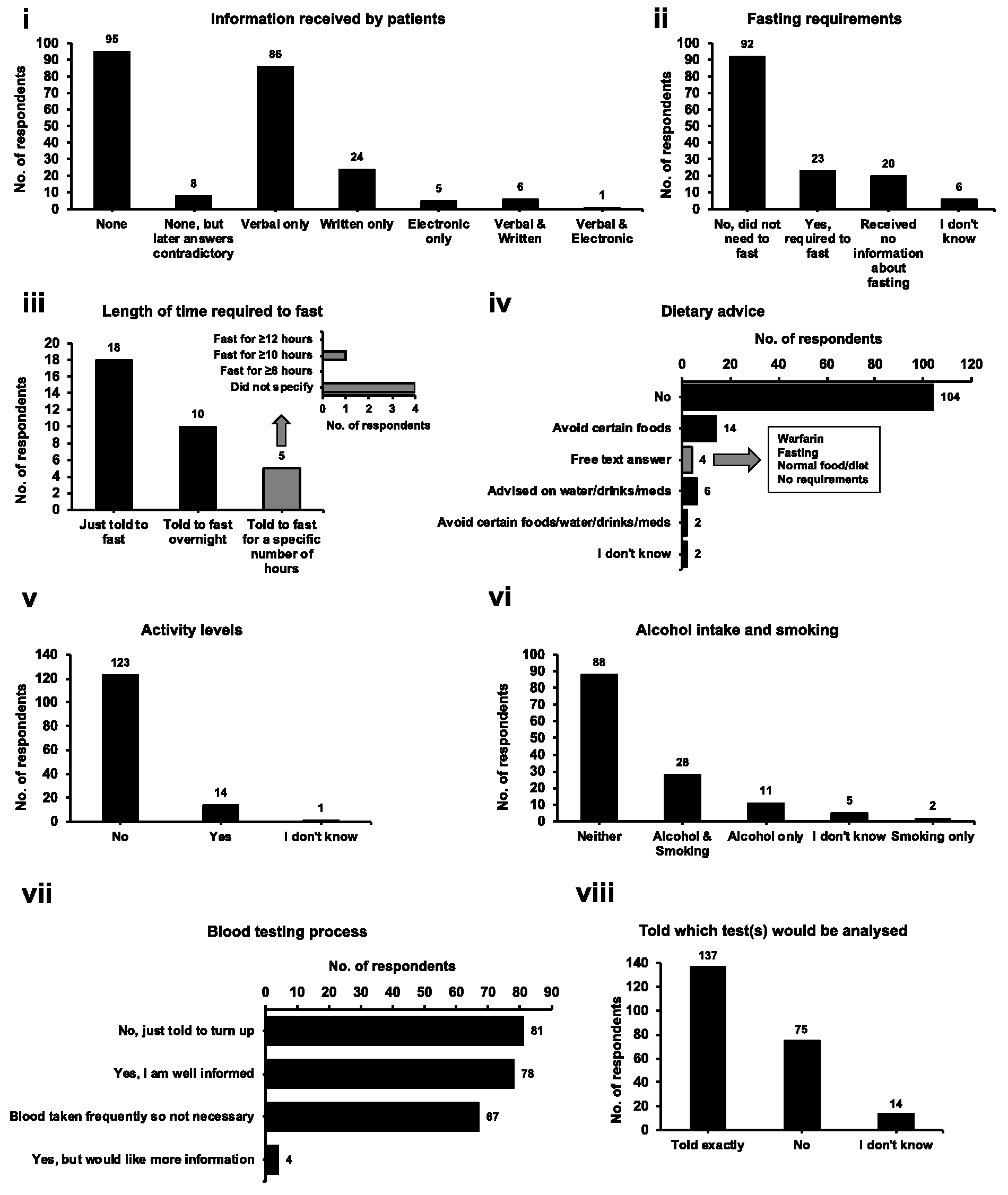
Preparation for blood test(s).
Q2 asked patients if they were required to fast or not before their test (Q2; RR = 141). A majority (n =92) answered that they were told they did not need to fast (Figure 1(ii)). In response to Q2, if respondents answered ‘No’ or ‘I received no information’ or ‘I don’t know’ (total n = 118) they were asked to skip to Q4; n = 9 moved on to Q3 but the remaining n = 109 skipped to Q4. Q3 asked for further information about fasting to see if participants had been told to fast for a specific number of hours. In total, 14% of participants (n = 33) answered this question but none had been told to fast for at least 12 h, although n =1 had been told to fast for ≥10 h (Figure 1(iii)).
Q4 queried if patients had received dietary advice before attending for their blood test (Q4; RR = 128), with n = 22 being told to avoid certain foods, drinks or medication (Figure 1(iv)). Four respondents ticked the option for ‘Yes, other’ giving a free text answer (Figure 1(iv)). Q5 asked if patients had received advice on activity levels before their blood test (Q5; RR = 138). One-hundred and twenty-three participants said that they had not received advice (Figure 1(v)), and one commented that they had been sent straight from their GP surgery to get their blood test performed. Q6 asked if advice had been given regarding alcohol consumption or smoking prior to having their blood test (Q6; RR = 134). Many participants (n = 101) did not answer this question due to previous prompts, but of those that did, most (n = 93) said they had not received advice or did not know (Figure 1(vi)). One respondent had written a free text response that they did not drink or smoke.
The last two questions were based on the broad understanding of the blood taking process and whether patients were aware of what tests had been requested. Q7 asked if patients had been given information on how the blood taking process would happen (Q7; RR = 230). There was a reasonable divide of those that were just told to turn up for a blood test (n = 81) and those that felt well informed (n = 78) (Figure 1(vii)). In addition, n = 67 said they have their blood taken frequently so did not feel it was necessary to receive information. One respondent said that they felt well informed after 33 years, presumably, as they required regular blood tests. The final question queried whether patients knew what tests would be analysed on their blood sample(s) (Q8; RR = 226). A majority (n = 137) said they had been told exactly what tests would be analysed, but n = 89 had just been informed they needed blood tests or did not know (Figure 1(viii)). One participant said they knew exactly what tests had been requested but only because they had asked their GP. Finally, one respondent felt well informed as they had been on warfarin for nine years and thought excellent information was available when required.
Discussion
Survey responses were received from n = 235 patients giving a reasonable indication of patient awareness of pre-analytical requirements. However, it constituted a small number of the total patients that would have attended for a blood test during this period; for example, it is estimated >10,000 patients would have attended the ESNEFT outpatient phlebotomy suite during November and December 2019. It is possible that not every patient was offered the chance to complete the survey, this being dependent on the time-constraints and engagement of staff on duty each day. A more direct approach to recruit participants could have improved the response rate. In addition, results may be biased by a higher participation of individuals more interested in the blood sampling process.
Individual response to modifiable pre-analytical factors is heterogeneous, making standardization in preparation for a blood test particularly important. 10 The more factors that are controlled, the more stable the patient’s baseline of blood results, reducing the chance of an erroneous result leading to unnecessary investigations or treatment changes.
In response to Q1, n = 103 stated that they had been given no information about the blood testing process, but n = 8 went on to contradict this answer. It may be that they did not make a direct connection between pre-analytical requirements (e.g. fasting) and the blood taking process. The n = 8 individuals had all been given information on whether to fast or not, but they were not told a specific duration for fasting, and 5/8 did not receive information about the intake of water or other drinks (including alcohol). Moreover, being told to fast or not is complicated by the fact that the definition of fasting and its duration are not well defined. 6
Biological variability has a major impact on the interpretation of test results and entails many factors including diet, stress, exercise, gender and age, as well as emotional state, posture and time of day. 12 Fasting is probably the best known and rigorously investigated biological pre-analytical factor. 10 However, there is still varied compliance and unawareness of its importance amongst both patients and clinical staff.11,14 The response to food and drink intake is variable amongst individuals, emphasizing the importance of controlling this parameter, as it may vary with metabolic rate, body composition, rate of food absorption and meal content. 15
López-Garrigós et al. found in their 2018/2019 survey of 254 subjects that 28% received no information about fasting; however, nearly all chose to fast anyway, although only 12% knew that 12 h was the recommended time and only 22% fasted for this length of time. 14 Kackov et al. also carried out a similar survey regarding awareness of fasting status. 11 They conducted an anonymous survey of 150 outpatients in 2013; finding that 61% were not fully aware of the proper definition of fasting and 52% received no information about preparation for their test(s). 11 A substantial 57% considered fasting a requirement for all laboratory tests but did not alter their behaviour. 11 Patients that did receive instructions from their clinician or nurse were only informed to fast but with no details, and very few (5%) looked up instructions on the internet. 11 The lack of obtaining information from electronic resources was supported by Miler and Šimundić who found that only 1/59 patients used the internet to find instructions on how to collect a 24 h urine specimen. 16
In this survey, n = 92 respondents were told they did not need to fast, and none were told to fast for 12 h. Even a light breakfast can affect many routine coagulation, haematological and biochemical parameters 1–4 h after food intake. This includes (but is not limited to) activated partial thromboplastin time, red blood cell count (RBC), haemoglobin (Hb), haematocrit (Hct), mean corpuscular volume, triglyceride, thyroid function tests (TFTs), lactate dehydrogenase, total protein, albumin, urea, creatinine, alkaline phosphatase, total bilirubin, urate, calcium, phosphate and magnesium.8,17–21 Food intake also temporarily increases venous blood pH and inflammatory markers, such as interleukin-6. 21 The majority of reference intervals and diagnostic cut-offs are based on early morning (7:00–9:00), fasting samples from a reference population. 10 It is, therefore, necessary to compare blood results when patients are in the same temporal and fasting state to avoid interpretative errors. 21 In addition, many analytes have diurnal variation, e.g. cortisol, testosterone, iron and transaminases, a particular problem when determining these parameters in shift workers. 22 The same issue applies to add-on requests when the time a sample was taken is not likely to be considered. The mechanism of the effect of food intake on blood tests varies: constituting haemodilution effects, the release of interfering factors into the bloodstream (e.g. lipids) and also metabolic or hormonal changes to measurands.10,21 Despite this, many tests are regularly requested without the mention of a need to fast, 21 a prime example being a TFT. However, a significant decrease in thyroid stimulating hormone (TSH) and free thyroxine has been identified 1 h after eating breakfast. 20
Fasting can, in theory, start at any time of day; however, the most convenient fasting period is overnight when compliance is likely to be highest and is arguably the time that biological variability is at a minimum. Outpatients are often told to attend for a blood test immediately after their medical consultation or they may be told to make a booking after a certain period, e.g. one month. Patients referred directly for a blood test are unlikely to be fasting, and those attending weeks later are unlikely to remember if they were given preparative information. 23 If glucose and lipids are requested, patients may be aware that the tests can be affected by diet; 24 however, there will be a lack of awareness about other analytes such as electrolytes and proteins as interferences are not as widely reported. Other tests require avoidance of specific foods and/or medications, information of which should be clearly communicated to the patient.
Many national and international groups including the European Federation for Clinical Chemistry and Laboratory Medicine (EFLM) Working Group for Preanalytical Phase (WG-PRE) and Latin America Confederation of Clinical Biochemistry (COLABIOCLI) Working Group for Preanalytical Phase (WG-PRE-LATAM) recommend a 12-h fast prior to blood tests,13,20,21 and we support this for all blood tests especially in cases of longitudinal monitoring. This is, of course, not feasible for most inpatient phlebotomy, for patients on parenteral nutrition, and in emergency departments. Adherence to these recommendations would increase laboratory workflow in the mornings, but enable faster turnaround times of acute work in the afternoon.
Only 22 patients in this survey were told to avoid food/drinks/medication prior to their blood test. Patients may drink water directly before a blood test to enable/promote venous access. Similarly, it has been identified that patients change their drinking habits during the collection of urine samples. 16 Unger et al. and Benozzi et al. found that drinking 300 mL of water 1 h before a blood test did not impact routine haematology and biochemistry results in a small cohort of women.25,26 However, 1 h after drinking a 12 oz. café latte, there is an acute and significant increase in blood glucose of up to 12%.10,27
The survey did not ask participants specific information about whether they had received information about taking morning medications. Although one patient reported being told to avoid warfarin before their blood test. In general, medications should be avoided unless vital; however, physicians should advise patients on an individual basis weighing up the risk of affecting blood test results versus the benefits of pharmacotherapy. An exception being the monitoring of certain therapeutic drug concentrations where blood sample timing pre- or post-dose is essential for interpretation.
Physical activity is another important pre-analytical factor rarely mentioned to patients, that can affect the serum fatty acid profile, 28 as well as a number of hormones, including growth hormone (GH), cortisol, prolactin, TFTs, steroids, gonadotrophins, insulin and catecholamines.29,30 Exercise can have a direct (metabolism/hormones) and indirect (increased fluid intake and supplements) effect on analytes. 6 In addition, acute physical exercise can cause haemoconcentration due to dehydration, hepatic and muscle cell damage with release of biomarkers (e.g. transaminases and creatine kinase), as well as an acute inflammatory response and generation of reactive oxygen species. 12 Transient benign increases in cardiac troponins and natriuretic peptides have been reported in endurance and strenuous training, even in young healthy subjects, due to increased cardiac output. 12 Moreover, professional athletes can have an increase in creatinine post-exercise, which in some cases would exceed acute kidney injury criteria. 12
A majority of participants (123/138) answering Q5 in this survey, indicated that they were given no advice on activity before attending for their blood test. Ideally, vigorous activity not normally performed by the patient should be avoided for 24 h prior to blood sampling. 13 Vigorous or strenuous activity is defined as requiring a large amount of effort and causing rapid breathing and a substantial increase in heart rate, e.g. running. 31 In a survey undertaken by López-Garrigós et al. in 2018–2019, nearly one-third of participants had undertaken strenuous activity during the 48–72 h period pre-blood collection. 14 Moreover, posture and activity directly before a phlebotomy appointment can affect blood test results, with significant increases in Hb, Hct and RBC when moving from a supine to sitting and sitting to a standing position. 21 It is recommended that outpatients are seated for 15 min before having their blood taken. 13
Many participants (43%) did not answer the question about alcohol/smoking in this survey, mainly because previous responses prompted them to skip past this question. Of those that did, 93/134 were given no advice or responded that they did not know whether they had received advice. Alcohol should be avoided for at least 24 h prior to blood tests, 14 and smoking (similarly to caffeine) should not be permitted on the morning of a blood test.10,14 Acute cigarette smoking increases both prolactin and GH secretion, and activates the hypothalamic-pituitary-adrenal axis. Moreover, active or passive smoking lowers TSH due to stimulation of thyroid hormone release. 32 In some cases, avoidance of alcohol, smoking and/or exercise prior to a blood test will not give a true picture of a patients’ physiological norm. However, since each factor can result in marked day-to-day variability in test results, minimizing acute effects is helpful particularly for longitudinal biomarker monitoring.
The survey aimed to assess whether patients felt informed about the blood testing process. In response, 149/235 patients felt they had been given information other than just being told they needed a blood test. Kljakovic carried out a similar survey of 135 patients at blood collection centres in Canberra, Australia, in 2012. 33 He found that 88/135 reported receiving information in preparation for their blood test, 61% being told how to prepare by their clinician and 25% stating they knew themselves. 33 However, a quarter wanted more information, and although 90% understood why blood tests were required, 37% could not name any of the tests requested. 33
One obvious pre-analytical factor not mentioned in this study was the time of blood collection. Participants are likely to have attended any time between 08:30 and 17:30 when the department was open. Unfortunately, participants were not asked to record the time of day, but responses may have been inaccurate if patients had to wait a significant amount of time for their appointment. Leppänen and Dugué reported statistically significant changes in 22 of 32 commonly measured analytes 40–80 min after breakfast and 130–170 min after breakfast compared with a fasting 8:00 sample. 34 However, few laboratory professionals are likely to add a comment to reports about result uncertainty due to sample timing. 34
There remains a lack of standardization of patient preparation for laboratory testing. One of the biggest challenges to successful harmonization is poor patient knowledge and awareness as demonstrated by the results of this survey and others.11,33 Patients are not often informed about pre-analytical requirements, likely because the requestor is unaware or does not have the time to explain it to them. 6 In addition, the validity of results was dependent on the reliability of patient memory. Reports indicate that 40–80% of medical information provided to patients is forgotten immediately and nearly half of information remembered is incorrect. 23 Information needs to be specific and uncomplicated, and if provided verbally, supported by written or visual material. 23 Both explicit categorization of information and provision of written/pictorial instructions can improve retention and adherence to guidance. 23 Supplying information on hospital internet sites does not appear to be valuable, as patients rarely use this resource. 11 In addition, information may be difficult for patients to find if they are not sure exactly what they are looking for because they are unaware of what tests they are having. Resources such as LTO-UK are highly regarded, but medical professionals could improve patient awareness by distributing LTO-UK leaflets and posters in phlebotomy suites. Unfortunately, the design of this study did not allow identification of what information patients had actually received prior to their blood test. Further controlled studies, with input from physicians and enhanced questionnaire design are required.
It is not easy for UK and RoI laboratory staff to keep patients informed since they rarely encounter patients. By the time patients attend for a blood test, it is often too late to change modifiable pre-analytical conditions. In addition, phlebotomists are unlikely to ask patients questions other than enquiring about their fasting status and only if they think it is relevant. However, most phlebotomists will accurately record the time of blood collection, which can be missed in primary and secondary care situations where pre-printed forms and/or labels are used.
In an ideal world, patients would obtain clear written instructions either on the back of request forms or disseminated by medical professionals, for example, a ‘do’s and don’t’s’ list in preparation for attending for their blood test. The preferred provider of such information is the requesting clinician.11,35 Figure 2 lists our recommendations for patients attending for non-urgent blood tests. The recommendations befit an ideal scenario but flexibility is warranted, particularly for tests where clinical studies demonstrating the effects of pre-analytical factors are lacking. Following UK and RoI stakeholder review, consensus recommendations may be achieved, but in the interim, the list can be utilized by outpatient facilities and GP surgeries to standardize the information given to patients and minimize pre-analytical variability. It is hoped that provision of such information will improve both patient satisfaction and health outcomes.
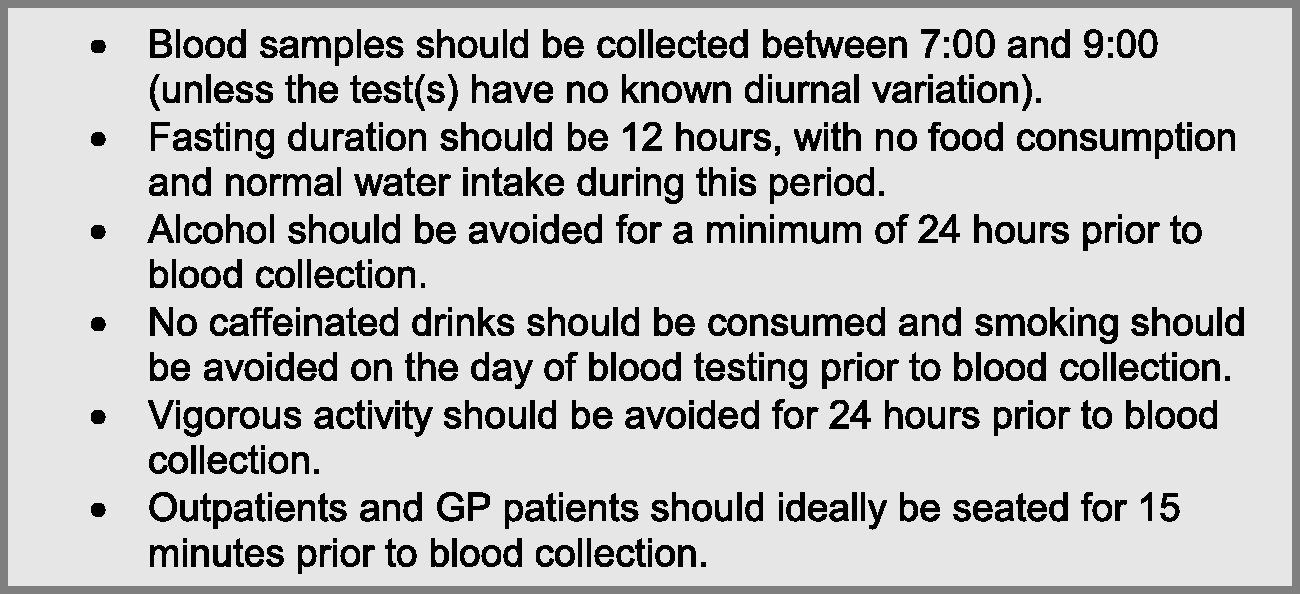
List of pre-analytical recommendations for reliable blood test results.
The main limitations of this study were the small sample size and only distributing the survey at two hospitals within the UK and RoI. The number of responses was skewed in favour of CUH, which may affect the applicability of findings at UK sites. Specific information could have been determined, for example, what food or medication patients had been told to avoid. It would also have been interesting to ask what tests patients were having; however, there were concerns in obtaining information that could have enabled patient identification.
Footnotes
Acknowledgements
We would like to thank and acknowledge all patients that took part in the survey, and the phlebotomy departments for distributing and collecting paper copies of the survey.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
Not applicable.
Guarantor
SH.
Contributorship
MPC, AS and SJC conceived the study. SH, MPC, AS and SJC developed the survey and were involved in study design. MJ and NRR were involved in data analysis. SH and MJ wrote the first draft of the manuscript. All authors reviewed and edited the manuscript and approved the final version of the manuscript.