
Abstract
Objective
Myonectin, a newly discovered myokine, enhances fatty acid uptake in cultured adipocytes and hepatocytes and suppresses circulating levels of free fatty acids in mice. Recent studies showed that serum myonectin concentration is negatively correlated with obesity. This study was undertaken to evaluate the change of serum myonectin in obese patients after laparoscopic sleeve gastrectomy.
Methods
This study was performed in a population of 42 obese and 58 control subjects from April of 2018 to December of 2019. All obese subjects underwent laparoscopic sleeve gastrectomy. Anthropometric measurements, lipid profiles, HbA1c and serum myonectin were assessed at baseline and six months after laparoscopic sleeve gastrectomy.
Results
Serum myonectin concentrations were significantly lower in the obese patients than in the controls. Serum myonectin concentrations were increased at six months after laparoscopic sleeve gastrectomy. Simple linear regression analysis indicated that serum myonectin was negatively correlated with weight, waist circumference, hip circumference, body mass index, fasting plasma glucose, homeostasis model assessment of insulin resistance and HbA1c. Only body mass index was still inversely correlated with serum myonectin after multiple linear regression analysis.
Conclusion
Serum myonectin is correlated with obesity and increased after laparoscopic sleeve gastrectomy.
Introduction
Obesity prevalence has increased all over the world in the last decades. Obesity results from the imbalance of multifactorial homeostasis such as environmental, behavioural, genetic, physiological, cellular and molecular functions. Obesity contributes to multiple health problems such as cardiovascular disease, sleep apnoea, aging and diabetes. 1 Weight loss can ameliorate or eliminate the metabolic risk factors related to these morbidities. 2 Bariatric surgery including the laparoscopic adjustable gastric band, laparoscopic sleeve gastrectomy (LSG) and the Roux-en-Y gastric bypass, has been shown to be the most effective treatment for morbid obesity. Clinical evidence has proven that bariatric surgery can reduce cardiovascular mortalities, decrease diabetic complications and improve life quality. 3
Myonectin, also called as CTRP15—C1q/TNF-related protein, is located on locus 2q37.3 and is released from skeletal muscle by the two major stimuli of exercise and nutrient (glucose and lipids) intake. Myonectin regulates lipid metabolism by promoting fatty acid uptake in adipose tissue and liver. 4 Obese non-diabetic subjects have significantly lower serum myonectin concentrations compared with lean non-diabetic controls. 5 This indicates that myonectin may be negatively correlated with obesity. Bariatric surgery is the most effective treatment for morbid obesity. Therefore, it is hypothesized that serum myonectin concentrations may alter after bariatric surgery.
This study was performed to investigate the correlation of serum myonectin concentrations with obesity and assess the change of serum myonectin concentrations after LSG.
Materials and methods
Study population
Forty-two morbidly obese subjects who were scheduled for the application of LSG with regular follow-ups for six months participated in this study from April 2018 to December 2019. Subjects were excluded from the study if they had a secondary cause of obesity (hypothalamic obesity, Cushing syndrome and pituitary dysfunction), gastrointestinal disease that was a contraindication for laparoscopic surgery, any other severe systemic disease that would have served as a contraindication to surgery. Fifty-eight healthy normal-weight volunteers were age- and sex-matched and were designated as the control group. The study protocol and recruitment were approved by the Ethical Committee of our Hospital. All participants gave written, informed consent.
Anthropometric assessment and laboratory analysis
Height, body weight (BW), waist circumference (WC), hip circumference (HC) and blood pressure were measured by trained operators pre-LSG and six months post-LSG. Body mass index (BMI) was calculated as weight in kilograms divided by height squared in meters (kg/m2). Waist–hip ratio (WHR) was calculated as HC divided by WC.
Laboratory methods
Venous blood samples were taken from all the subjects following a fast of at least 8 h both at baseline and six months after LSG. Serum lipids, fasting plasma glucose (FPG), fasting insulin and HbA1c were measured. Serum was centrifuged and stored at − 80°C for myonectin assay. Serum myonectin concentrations were measurement using a commercially available enzyme-linked immunosorbent assay kit (Aviscera Biosciences, Santa Clara, CA). Homeostasis model assessment of insulin resistance (HOMA-IR) was calculated as insulin reading (µIU/mL) multiplied by plasma glucose level (mmol/L) and divided by 22.5.
Statistical analysis
Statistical analysis was carried out using SPSS version 17.0 software program. The results were displayed as mean ± standard errors. Unpaired t test or Chi-square tests was performed to compare the differences of characteristic between obese subjects and healthy controls. The correlation between serum myonectin and other parameters was analysed using simple linear regression analysis. Those variables with a P < 0.05 were entered into a multiple linear regression model to determine the contribution of various factors to serum myonectin. Statistical significance before and after surgery was evaluated using the paired two-tailed t-test. Statistical significance was accepted at a level of P-value less than 0.05.
Results
Baseline clinical characteristics of obese subjects and controls
The clinical characteristics of the two groups are presented in Table 1. Obese subjects showed elevated BW, WC, HC, WHR, BMI, systolic blood pressure (SBP), diastolic blood pressure (DBP), FPG, fasting insulin, HOMA-IR, HbA1c, triglycerides (TG), prevalence of hypertension and diabetes, as well as decreased high-density lipoprotein cholesterol (HDL-C) compared with the controls.
Various characteristics of obese patients and controls.
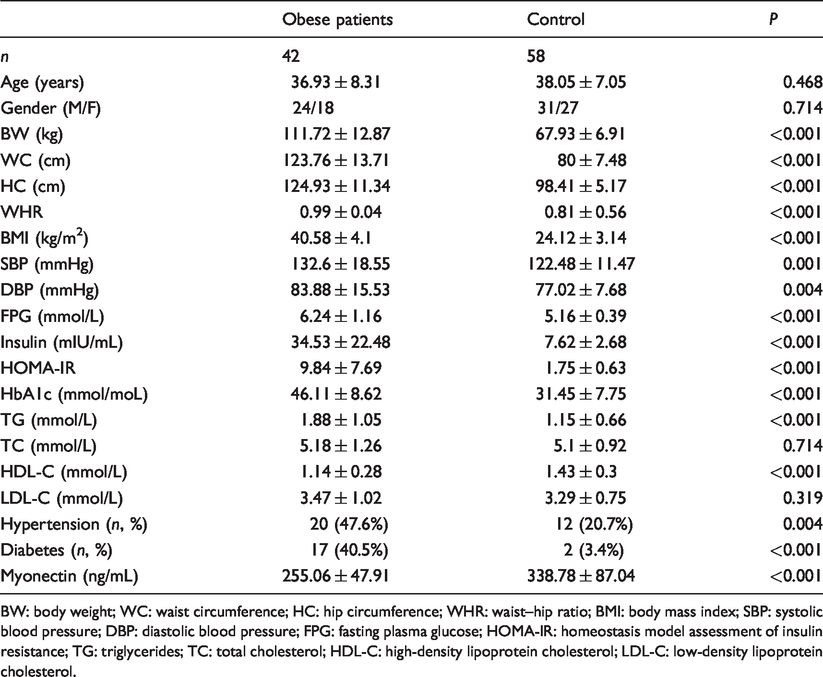
BW: body weight; WC: waist circumference; HC: hip circumference; WHR: waist–hip ratio; BMI: body mass index; SBP: systolic blood pressure; DBP: diastolic blood pressure; FPG: fasting plasma glucose; HOMA-IR: homeostasis model assessment of insulin resistance; TG: triglycerides; TC: total cholesterol; HDL-C: high-density lipoprotein cholesterol; LDL-C: low-density lipoprotein cholesterol.
Serum myonectin concentrations
Obese subjects had lower serum myonectin concentrations compared with the controls (Table 1).
The correlation of serum myonectin with other variables
Simple linear regression analysis indicated that serum myonectin was negatively correlated with BW, WC, HC, BMI, FPG, HOMA-IR and HbA1c (Table 2). Only BMI was still inversely correlated with serum myonectin after multiple linear regression analysis (Table 2).
The correlation between serum myonectin and other clinical parameters in obese patients.
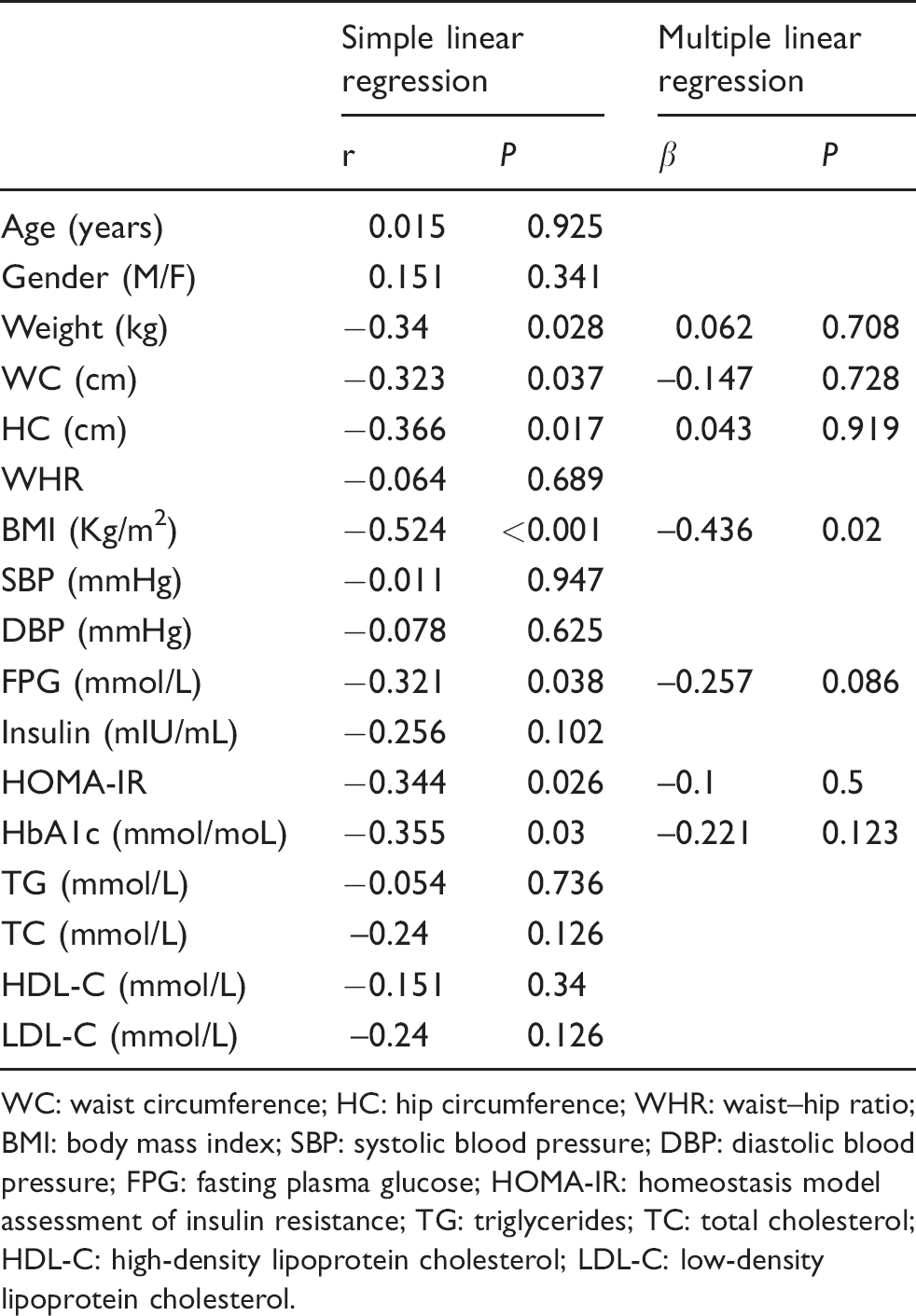
WC: waist circumference; HC: hip circumference; WHR: waist–hip ratio; BMI: body mass index; SBP: systolic blood pressure; DBP: diastolic blood pressure; FPG: fasting plasma glucose; HOMA-IR: homeostasis model assessment of insulin resistance; TG: triglycerides; TC: total cholesterol; HDL-C: high-density lipoprotein cholesterol; LDL-C: low-density lipoprotein cholesterol.
Clinical characteristics pre-LSG and six months post-LSG
Obese patients showed decreased levels of BW, WC, HC, WHR, BMI, SBP, DBP, FPG, fasting insulin, HOMA-IR, HbA1c, TG, total cholesterol, low-density lipoprotein cholesterol, prevalence of hypertension and diabetes, as well as increased HDL-C six months post-LSG compared with those during pre-LSG (Table 3).
Various characteristics of obese patients at baseline and six months after LSG.
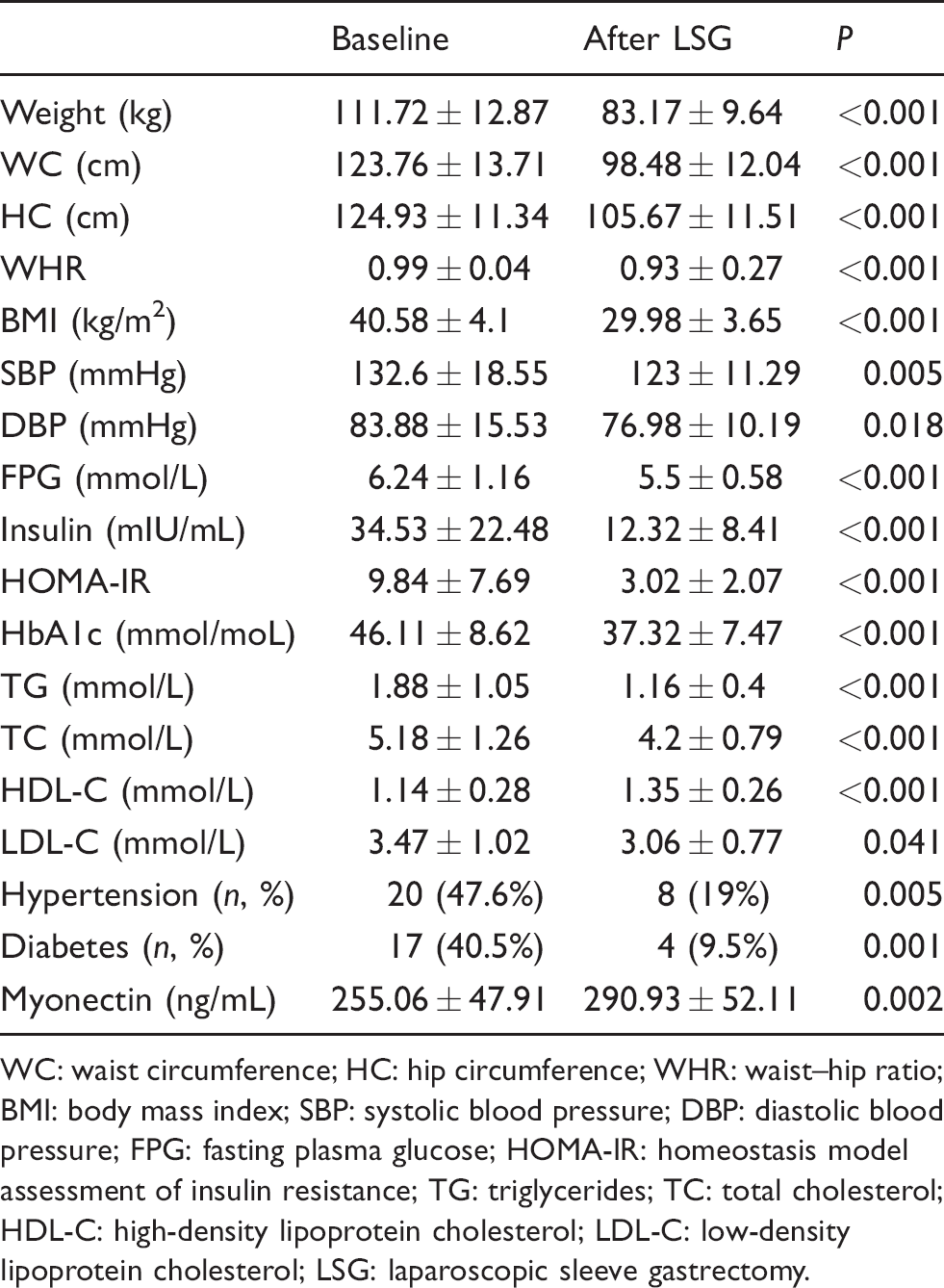
WC: waist circumference; HC: hip circumference; WHR: waist–hip ratio; BMI: body mass index; SBP: systolic blood pressure; DBP: diastolic blood pressure; FPG: fasting plasma glucose; HOMA-IR: homeostasis model assessment of insulin resistance; TG: triglycerides; TC: total cholesterol; HDL-C: high-density lipoprotein cholesterol; LDL-C: low-density lipoprotein cholesterol; LSG: laparoscopic sleeve gastrectomy.
Serum myonectin concentrations pre-LSG and six months post-LSG
Serum myonectin concentrations were significantly increased post-LSG compared with pre-LSG (Table 3).
Discussion
There has been growing evidence of the regulation of muscle mass and the metabolism of other tissues by release from skeletal muscle of soluble factors known as myokines. Myokines are described as molecules produced and secreted by skeletal muscle in response to physical activity. 6 Myokines have emerged as novel molecular mediators of fat browning, suggesting a role of myokines in obesity. 7 Recent studies have shown myokines such as irisin, fibroblast growth factor 21 and meteorin-like were correlated with obesity and showed altered concentrations after bariatric surgery.8–10 Myonectin is a recently identified novel myokine expressed mainly in skeletal muscle. The present study demonstrated that myonectin is correlated with obesity and significantly increased after LSG. This suggests crosstalk between skeletal muscle and adipose tissue.
Obese non-diabetic and diabetic subjects have significantly lower serum myonectin concentrations compared with lean non-diabetic controls or lean diabetic subjects. 5 Our studies also showed the decreased serum myonectin concentrations in obese subjects compared with healthy controls. Peterson et al. reported that the mRNA expression of myonectin was increased in the diaphragm muscles of obese Zucker rats compared with lean Zucker rats. 11 However, the differences of protein and serum concentrations of myonectin were not compared between the two groups in the study.
Myonectin-deficient male mice fed a high-fat diet had greater fat storage and significantly enlarged adipocytes compared with wild-type litter mates. 12 Recombinant myonectin administration reduced circulating levels of free fatty acids without altering adipose tissue lipolysis in mice. 4 In addition, myonectin promoted fatty acid uptake in cultured adipocytes and hepatocytes by up-regulating the expression of genes that promote lipid uptake. 4 Recombinant myonectin administration suppressed starvation-induced autophagy in mouse liver and cultured hepatocytes, underscoring the importance of myonectin-mediated tissue crosstalk in maintaining energy homeostasis. 13 All these investigations point to the key role of myonectin in regulating energy homeostasis and obesity.
Myokines are peptides produced and secreted by the skeletal muscle, with autocrine, paracrine and endocrine actions. These myokines provide the basis for crosstalk between skeletal muscle and other organs including adipose tissue. Adipose tissue, especially white adipose tissue, acts as an endocrine organ and modulates metabolism by signalling other organs. By inhibiting fat storage and regulating lipid metabolism in adipose tissue, myonectin may have a role in protecting against obesity. The correlation between reduced myonectin and obesity reflects the crosstalk between skeletal muscle and adipose tissue. We hypothesize that in obesity status, adipose tissue sends adverse signal via adipokines to skeletal muscle tissue. Adipokines have an adverse effect on skeletal muscle and lead to reduced myonectin secretion from skeletal muscle. Reduced myonectin in turn has an adverse impact on the regulation on the lipid metabolism of adipose tissue and may promote obesity. The correlation between reduced myonectin and obesity reflects the crosstalk between skeletal muscle and adipose tissue. Obese patients had significantly reduced BW following bariatric surgery. We hypothesize that reduced adipokine signalling as a result of the reduced adipose tissue mass leads to increased myonectin secretion from skeletal muscle.
Exercise impacts myonectin production and blood concentration: myonectin protein concentration in the diaphragm muscles of obese Zucker rat was increased following nine weeks of aerobic training. 11 Four weeks of treadmill exercise also increased circulating myonectin concentrations in wild-type mice. 14 In addition, serum myonectin concentrations increased significantly in obese and overweight women for three weekly 45-min sessions of aerobic exercise training for eight weeks. 15
This study has several potential limitations. First, the conclusions are limited by relatively small sample size. Secondly, the follow-up time is relatively short. In a future study, we will further expand the sample size and extend the follow-up time to observe the change in myonectin concentrations in the longer term.
In short, serum myonectin concentrations are correlated with obesity and are increased after LSG.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
The ethics committee of Shandong Provincial Hospital, Cheeloo College of Medicine, Shandong University (20180324).
Guarantor
CQ.
Contributorship
CQ researched literature and conceived the study. LL and QW were involved in protocol development, gaining ethical approval, patient recruitment and data analysis. LL wrote the first draft of the article. All authors reviewed and edited the article and approved the final version of the article.