
Abstract
Serological tests for COVID-19 antibodies have been hailed as a potential ‘game-changer’ which could limit the spread of infection and relaxation of some of the current restrictions relating to social distancing. Their availability is vital and urgently needed in fighting the current pandemic. Across the world, in many countries, guidance has been given to laboratories and commercial manufacturers to help them to accelerate the availability of tests they develop in order to achieve more rapid and widespread testing capacity. The UK government, for example, has ordered millions of finger-prick tests to allow community testing. Similarly, in the United States (US), COVID-19 has been declared a public health emergency, thereby justifying the authorization of emergency use of in vitro testing including COVID-19 antibodies. The finger-prick tests ordered by the UK government are point-of-care tests (POCT) that use lateral-flow devices from a few drops of blood, with reportedly reliable results available in less than 20 min; these devices are similar in design to those used for urine pregnancy testing. 1
Significant latitude has been extended to developers of tests for COVID-19 antibodies. In the US, the Food and Drug Administration (FDA) has granted permission for marketing or use of kits once appropriate ‘in-house’ evaluation has been performed to determine their accuracy and reliability. However, in the rush for serological testing, it is important that all of those implementing these measures recognize the complexity and, especially, limitations of these tests. Clinical laboratories are aware of the relatively high rate of inaccuracy of these tests and the pitfalls of POCT procedures even when quality assurance and quality control (QC) are documented for validation and proper accreditation. 2 Therefore, the participation of clinical laboratory scientists in assessing the viability of such products is paramount.
Laboratory professionals recognize that all serological tests for antibodies, including COVID-19 antibodies, have inherently high analytical, unavoidable error rates. The error rate of these tests is variable, random, insidious and unpredictable, and is caused by different classes and subclasses of specific antibodies that are produced over the period of an activated immune response (in this case COVID-19 infection). This is compounded by the huge array (billions) of other endogenous antibodies which can be produced, some of which are, in some individuals, fortuitously capable of interacting with the antibodies used as biological reagents. There is thus some intrinsic inaccuracy even when the best methodologies, most reliable reagents and stringent internal and external quality controls are implemented. To imply that such tests would be as simple and reliable as a pregnancy test is misleading; urine is immunoglobulin-free and inaccuracy due to cross-reactivity is not possible.
False-positive and false-negative results are therefore inevitable and will vary in cohorts with different prevalence of antibodies. The likelihood of erroneous results in different cohorts can be estimated when information such as the inaccuracy of the test and the prevalence of COVID-19 antibodies is taken into consideration.3,4 Two hypothetical examples, in populations with high and low prevalence, illustrate this point. It is reasonable to expect that most previously infected patients (i.e. testing positive with reverse transcriptase-PCR assays) will have developed COVID-19 antibodies. 1 Using a serology test with ±2% inaccuracy, and assuming 95% prevalence of antibodies, some 29% of the negative results in such a cohort would be false negatives. By contrast, if the same test were used in a cohort with low prevalence of COVID-19 antibodies (say, 10%), e.g. general population, 17% of all positive results would be false positives, giving a false sense of security on the assumption that past infection confers immunity. 1 The formulae on which these estimates are based are simple, and the calculations are shown in Figure 1. They show that false-positive results are more likely in cohorts with low prevalence of COVID-19 antibodies, and false-negative results more likely in cohorts with high prevalence of antibodies. False results may persist for weeks, months or even longer. Appropriate follow-up tests may help to identify some false results when suspected (e.g. by repeating the test using a different analytical platform). 4
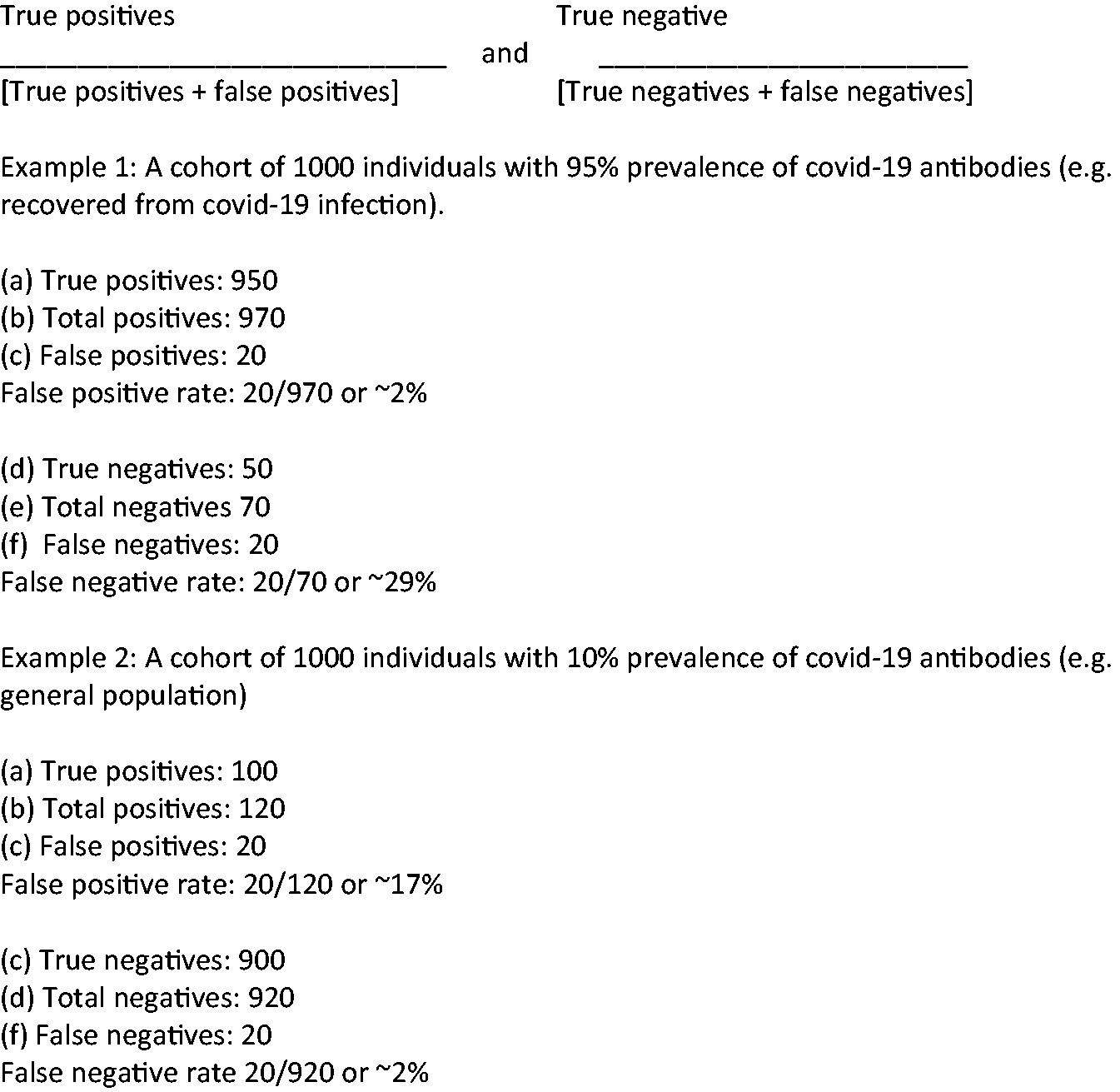
The calculations shown in the figure are based on a test inaccuracy of ±2%. In 1000 tests, 20 false positive and 20 false negative may be expected. The calculations are approximations, but would not be radically different from those resulting from a precise statistical calculation using Bayesian statistic.3,4
In conclusion, serological screening tests for COVID-19 antibodies are desirable and if conducted and interpreted properly, may help to correctly identify most (but not all) of those who have had a recent COVID-19 infection. Inaccuracy of antibodies tests is, however, unavoidable and will inevitably lead to misclassifications. This must be acknowledged if unreasonable expectations are to be avoided.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
Not applicable.
Guarantor
AAAI.
Contributorship
Sole author.