
Abstract
It is increasingly easy for the general public to access a wide range of laboratory tests. Tests can be ordered online with little or no input from a health professional. The complementary and alternative medicine (CAM) community promote and sell a wide range of tests, many of which are of dubious clinical significance. Many have little or no clinical utility and have been widely discredited, whilst others are established tests that are used for unvalidated purposes. They range from the highly complex, employing state of the art technology, e.g. heavy metal analysis using inductively coupled plasma-mass spectrometry, to the rudimentary, e.g. live blood cell analysis. Results of ‘CAM tests’ are often accompanied by extensive clinical interpretations which may recommend, or be used to justify, unnecessary or harmful treatments. There are now a small number of laboratories across the globe that specialize in CAM testing. Some CAM laboratories operate completely outside of any accreditation programme whilst others are fully accredited to the standard of established clinical laboratories. In this review, we explore CAM testing in the United States, the United Kingdom and Australia with a focus on the common tests on offer, how they are reported, the evidence base for their clinical application and the regulations governing their use. We will also review proposed changed to in-vitro diagnostic device regulations and how these might impact on CAM testing.
Keywords
Introduction
The way in which members of the public access laboratory tests has changed significantly in recent years. It is increasingly common for tests to be performed outside of traditional healthcare pathways and sometimes with little or no input from a healthcare professional. Patients can use home test kits bought online, send samples off by post or visit a variety of alternative practitioners who will organize tests for them. Of course increased access to diagnostic tests (if performed appropriately) can benefit both the patient and the clinician but increased accessibility comes at a risk; patients are increasingly exposed to tests that are unvalidated, misleading or discredited. In the complementary and alternative medicine (CAM) setting the results of such tests may be used to justify expensive, unnecessary or harmful treatments. In this review, we use the umbrella term ‘CAM testing’ to describe diagnostic testing of this nature, i.e. tests of little or no clinical benefit that represent a potential risk to patient safety.
Readers may be familiar with the higher profile facets of the CAM testing market that feature in the media, such as some direct-to-consumer genetic testing 1 or food intolerance tests 2 but they may be less familiar with others. Practitioners and laboratories marketing alternative tests are notoriously difficult to regulate and commonly make misleading claims of clinical benefit.3,4
It can be difficult to discover where samples for CAM testing are actually being analysed, whether the laboratory is accredited, what methodology is being used and whether the test is validated. Indeed, even accreditation to a recognized standard, such as ISO 15189, does not guarantee that a test is clinically valid.
A wide variety of analytical techniques are encountered in CAM testing and may include anything from the primitive, e.g. live blood cell analysis (LBA), to the state-of-the-art, e.g. ICP MS. Some tests have little or no clinical benefit regardless of how they are applied. Others may have valid clinical uses but may become misleading when used in the wrong clinical context.
Laboratories specializing in CAM testing often promote themselves as specialists in environmental, nutritional or natural medicine or other CAM disciplines. Some operate entirely outside of any recognized accreditation programme whilst others are accredited to the standard of established clinical laboratories. Some sell tests directly to the public; others state they only accept requests from health professionals, but on closer inspection requests are often accepted from Naturopaths, Nutritionists and other CAM practitioners, who are generally not registered health professionals in the UK, Australia and in most states of the US. 5 This introduces the further risk that not only might tests be requested inappropriately but laboratory reports may be misinterpreted. Tests are frequently performed in large profiles of analytes which increases the statistical probability that an abnormal result will be obtained regardless of any disease pathology.
In contrast with many conventional laboratory reports, CAM laboratory reports are usually designed with the patient in mind. They are often well presented with visually engaging graphics. There may be a detailed interpretation with complex language and pseudo-scientific terms. Reports frequently recommend treatments to remedy the ‘abnormalities’ detected.
This review will focus on some of the commonly-performed CAM tests, ranging from completely discredited tests to accepted tests used in unconventional ways. However, it is first necessary to qualify what is meant by test validity and how this is determined.
Validity and clinical utility of testing
The ACCE framework was originally developed for evaluation of genetic tests
6
. However it is applicable to all forms of laboratory tests and especially useful for evaluating CAM laboratory tests. There are four key factors for evaluation:
Laboratory and in-vitro diagnostic device regulation
Australia
In Australia, pathology laboratories only require accreditation by the National Association of Testing Authorities (NATA) if they want access to the Medical Benefits Schedule where the national health scheme Medicare rebates all or part of the cost of testing. All CAM laboratories in Australia directly bill the patient and thus were not required to be NATA-accredited prior to mid-2017.
The Therapeutic Goods Administration (TGA) regulates in-vitro diagnostic devices (IVDs). Commercially supplied IVDs are required to be listed on the Australian Register of Therapeutic Goods (ARTG). Lower risk in-house IVDs, such as those used in CAM laboratories, are not required to be listed on the ARTG but users are required to implement an appropriate Quality Management System (ISO 15189). However, there is no mechanism to ensure this is done in laboratories that are not NATA-accredited meaning they may not meet even basic quality standards, such as IQC and EQA.
ARTG listing 7 requires a conformity assessment that in theory has stringent requirements, but in practice a variety of devices that lack analytic validity, clinical validity and clinical utility have been listed. Furthermore, once a device has been listed for a limited range of purposes there is nothing to stop CAM practitioners and laboratories using it for other purposes. New rules are in place that required all laboratories using in-house IVDs to have been NATA-accredited or proceeding toward NATA-accreditation for those tests by 30 June 2017. The full effects of this regulatory change are not yet clear but it is likely to remove some in-house CAM IVDs from the market place. However, it will have no effect on commercial IVDs that have achieved ARTG listing despite lacking clinical validity and utility, such as food-specific IgG tests.
United States
The 1998 Clinical Laboratory Improvement Amendments (CLIA) law establishes quality standards for all non-research laboratory testing to ensure accuracy, reliability and timeliness of test results. The Centers for Medicare and Medicaid Services (CMS) along with the Food and Drug Administration (FDA) and the Centers for Disease Control and Prevention (CDC) are responsible for implementing CLIA. CLIA applies to all entities providing clinical laboratory services except some laboratories which are exempt, including forensic laboratories, drug testing laboratories certified by the Substance Abuse and Mental Health Services Administration and some Federal laboratories. In addition, there are thousands of small laboratories providing simple laboratory procedures that have been given a certificate of waiver by the FDA. Laboratory surveyors do not make routine visits to waived laboratories to ensure compliance with CLIA requirements. This was recently flagged by the American Association of Clinical Chemistry as an issue of significant concern. 8
CLIA certification requires laboratories to meet standards in a variety of areas including staff qualifications; proficiency testing and test accuracy, reliability and timeliness. It does not require demonstration of clinical validity and utility. Thus, CAM laboratories in the US can be CLIA certified while offering tests that are neither clinically valid nor clinically useful. 9 The CDC and CMS have looked at aspects of CAM testing, especially relating to live blood analysis, but have not addressed these issues.10,11
Recently, the FDA has proposed that it will begin to regulate lab-developed tests with a view to ensuring that they are clinically valid but this proposal has met with significant resistance.12,13
United Kingdom and the European Union
In the UK, laboratory accreditation is not mandatory in order to offer clinical diagnostic testing. The vast majority of laboratories offering NHS services will however be accredited to the ISO 15189 standard by UK Accreditation Service (UKAS) or be in the process of transitioning to this from existing accreditation under Clinical Pathology Accreditation UK (CPA). Most CAM laboratories offering private services direct to patients or healthcare practitioners are not accredited. Whilst accreditation ensures high standards of management and analytical quality, CPA standards did not contain any requirement to ensure the tests offered have of clinical validity. The ISO 15189 standard does require extensive validation/verification but again this is focused on analytical aspects. Furthermore, UKAS assessment is carried out on a test by test basis. This could lead to CAM laboratories claiming accreditation by submitting a small number of tests from their repertoire for assessment whilst leaving others ‘out of scope’. This has the potential to mislead patients and practitioners about the quality of the tests they are purchasing.
Currently, the only legal requirement for laboratories offering medical diagnostic services in the UK is registration with the Care Quality Commission (CQC), which inspects diagnostic services in England but not the rest of the UK. This has been mandatory since 2010 but at the time of writing there are still a number of (unaccredited) laboratories offering diagnostic services without CQC registration. In addition, the CQC standards for standalone laboratories are designed primarily for the assessment of patient-facing services, and make little assessment of analytical quality. This is despite suggestions in a recent national Pathology Quality Assurance Review that the CQC would use formal accreditation as a marker of quality. 14
IVDs marketed in the European Union (EU) are regulated under the IVD Directive 98/79/EC. 15 To be legally marketed, an IVD must bear a ‘CE mark’ indicating conformance with the directive. Until recently, most IVDs have been self-certified by the manufacturer but following revision of the IVD regulations in 2016 IVDs will in future require conformity assessment by an authorized ‘Notified Body’, which in the UK is the MHRA (Medicines and Healthcare Regulatory Authority).
There is no published register of CE marked IVDs which makes checking the status of tests difficult. It is hoped that the proposed European Database on Medical Devices (EUDAMED) will be a step forward in this regard. 16
The IVD Regulation was adopted in May 2016 and will be fully applied by EU member states from 2022, which allows a 5-year period of transition (N. Jassam, personal communication. 10 March 2016). The revised Regulation is a substantial transformation from its predecessor and introduces a risk-based classification system for determining the level of conformity assessment required (see Table 1). It is likely the majority of CAM tests will be classified as Class A or B. Whilst it will be possible for some in-house testing performed within health institutions to be exempt, it is likely that in-house tests marketed by CAM laboratories will not. The new Regulation also introduces a requirement to demonstrate clinical validity, a concept that had been previously lacking. However, it is currently unclear what level of evidence will be required.
Risk-based classification of IVDs based on recommendations from the Global Harmonisation Task Force (GHTF). 17
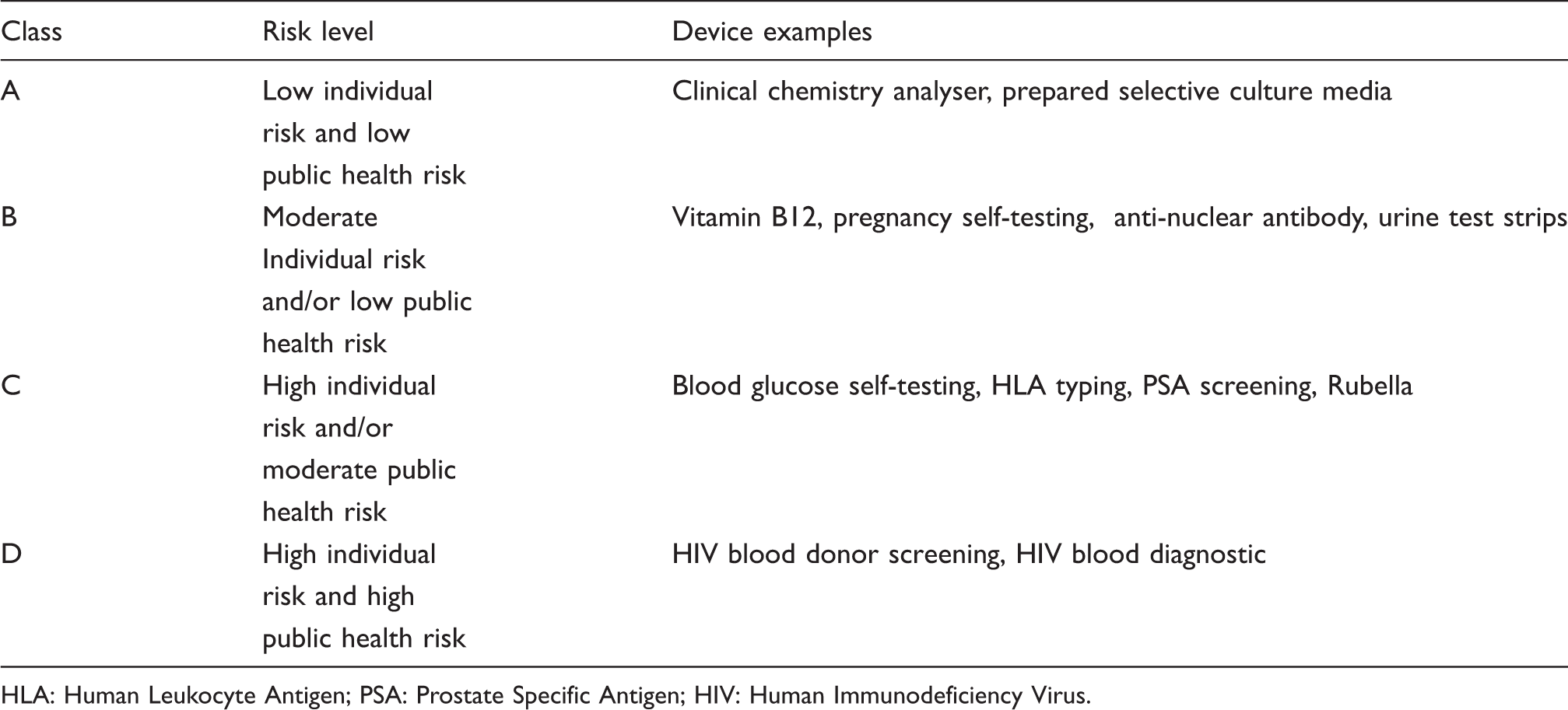
HLA: Human Leukocyte Antigen; PSA: Prostate Specific Antigen; HIV: Human Immunodeficiency Virus.
The extent to which the UK will implement the new Regulation is now uncertain given the country’s imminent withdrawal from the EU.
Laboratory tests commonly used in CAM
Live blood cell analysis
LBA, also known as dark-field video analysis, or nutritional blood analysis, is a technique based on the analysis of unstained, ‘live’ peripheral blood using a high-resolution dark field microscope. Its origins lie with a German zoologist named Gunther Enderlein who was a proponent of the long since discredited theories of ‘pleomorphism’. Analysis is performed in ‘real time’ in consultation with the patient using a linked video monitor as practitioners interpret cell morphology and the presence of specific features and ‘pathogen structures’ that appear as the sample is ‘stressed’ during slide preparation. Practitioners have claimed that the technique can diagnose anything from nutritional and energy ‘imbalances’ to acidaemia and haematological malignancies.
There are two small studies in the literature that have looked at the effectiveness of LBA. The first looked at inter-practitioner reproducibility. 18 Two experienced practitioners analysed 48 blood samples from 24 diabetic patients on multiple occasions and inter-observer and test–retest reliability were calculated. In 31% of observations, the two observers disagreed on the features present and when repeat samples on individual patients were retested, there was 26% discordance with the observer’s own previous findings. The authors acknowledge the small size of the study but conclude nonetheless that the technique is very difficult to standardize and its reliability is not high enough to serve as a basic diagnostic test. A second study was designed to test claims that LBA can be used to identify cancer at a very early stage. 19 An experienced practitioner blindly analysed blood samples from 110 patients, 12 of whom had radiological evidence of metastatic lesions. Only 3 of the 12 cancer patients were correctly identified (sensitivity 0.25) while 40 patients were incorrectly diagnosed with cancer (specificity 0.64). Although based on the assessment of only one practitioner, this study clearly illustrates the risks associated with this technique.
In the US, the CDC and CMS – who implement the CLIA accreditation programme – list LBA as an ‘unestablished test’. By default, LBA is therefore categorized as a ‘high complexity’ test requiring any site offering it to be fully CLIA-certified for high complexity testing (the standard for medical laboratories). Any site offering LBA without appropriate CLIA certification can be sanctioned under federal or state law.
The CMS state that it is ‘virtually impossible’ for a facility offering LBA to meet certification requirements and in 2001 launched a crackdown on those offering it. 10 They audited 200 sites (of an estimated 10,000–15,000 in total) offering LBA and found that 80% were uncertified with the remaining 20% either having their certification revoked or agreeing to discontinue offering the test. LBA remains widely available in the US despite this tight regulation emphasizing the scale of the task faced by regulators.
In the UK, the Trading Standards Institute brought about a rare conviction of an LBA practitioner under the 1939 Cancer Act 20 but perhaps the only UK regulator to have consistently taken action is the Advertising Standards Authority, who have upheld a number of complaints and forced the removal of offending promotional material. 21 They state: ‘CAP [Committees of Advertising Practice] is yet to see any evidence for the efficacy of this therapy which, without rigorous evidence to support it, should be advertised on an availability-only platform’.
Leukocytotoxic tests: Bryan’s test, ALCAT test, MELISA test
The leukocytotoxic test was first described by Black in 1956. 22 In the original test, solutions of protein allergens were allowed to dry on a glass slide. Then plasma from the patient and buffy coat leukocytes from either the patient or a non-allergic donor were mixed and placed in contact with the dried allergen on the slide and observed under the microscope. Black claimed that in sensitized patients the leukocytes, which are mainly polymorphonuclear leukocytes, showed toxic effects and died within 15 min to 2 h but did not do so if the patient was not sensitized to that allergen. In the latest version of the test, both buffy coat cells and plasma are from the patient’s blood sample. The test was subsequently popularized by Bryan and Bryan from 1960 onwards,22–25 despite the publication of a study in 1958 26 which could not replicate Black’s original findings. Lieberman assessed Bryan’s methods in a controlled study and found that the test had very poor correlation with known allergens, a high false-positive rate and poor within-individual and inter-operator reproducibility. 27 Subsequent studies have come to the same conclusion that the test is unreliable and should not be used.28,29
The ALCAT test is a more recent commercial, mechanized version of the cytotoxic test. A blood specimen is mixed with allergen and then passed through an electronic cell counter which measures leukocyte cell size. The manufacturer supplies panels of hundreds of foods, environmental chemicals, food colourings, moulds, herbs and some drugs. The evidence for the ALCAT test has been evaluated by a number of independent reviewers. Potter et al. 30 recommended against its use in 1992 because of lack of evidence. In 1998, the Allergy Society of South Africa 31 recommended against its use because of lack of evidence and adverse findings in two small South African studies.32,33 Wüthrich evaluated the evidence for the ALCAT test in 2005 and again in 2014 and found no credible evidence to support the test.34,35
Earlier statements from professional societies including the New York Academy of Medicine 36 and American Academy of Allergy 37 have recommended against using the cytotoxic test (Bryan’s test). Later statements from the Allergy Society of South Africa, 31 the European Academy of Allergy and Clinical Immunology38,39 and The Australasian Society of Clinical Immunology and Allergy 40 have all recommended against using either form of the cytotoxic test (Bryan’s or the ALCAT) for the diagnosis of food intolerance or allergy.
MELISA (Memory Lymphocyte Immuno-Stimulation Assay) is a commercially-available assay used primarily to test for metal sensitivity and more recently for Lyme disease. Literature reports on the validity of MELISA testing are mixed. Some indicate that MELISA testing is accurate and clinically useful.41–45 However, these reports originate from a commercial laboratory providing the test. In contrast, a number of independent researchers have reported that MELISA is so non-specific as to be of no clinical utility.46–50
Food intolerance testing using food antigen-specific IgG4 antibodies
Food intolerance or sensitivity testing is now widely available as a direct-to-consumer test and is often based on the analysis of serum food antigen-specific IgG4 antibodies (sIgG). Tests are commonly offered as a panel, sometimes comprising sIgG to over 200 food components. Major manufacturers, such as Siemens and Thermofisher, have CE marked immunoassay kits on the market in the EU but none have FDA approval for clinical use in the US. 51 The test is marketed suggesting it can identify foods responsible for causing a variety of symptoms, such as bloating, abdominal pain, fatigue, depression, irritable bowel and skin complaints. Patients taking the test will often receive an interpretive report which recommends excluding foods from the diet.
Interest in sIgG grew when work in the 1980s suggested these antibodies might induce histamine release from basophils. 52 Despite much research since this has never been confirmed and a role for sIgG in IgE mediated disease remains to be proven. A 2004 randomized controlled trial of food elimination diet based on sIgG testing suggested some benefit for patients with IBS 53 but this was robustly challenged on the grounds of poor study design 54 and subsequent studies have failed to show an association between sIgG and IBS symptoms. 55 Numerous studies have now demonstrated that food-specific sIgG antibodies are frequently present in unselected populations with no evidence of food intolerance or food allergy. This has been clearly demonstrated in children where for some common foods, such as cow’s milk, egg and wheat, sIgG antibodies appear to be detectable in almost every case and often at high concentration.56,57 Similarly, in adults, large cross-sectional studies have demonstrated high levels of sIgG to common foods with little or no correlation to clinical symptoms. 58 These studies support the theory that the presence of food-specific IgG indicates a benign response to antigen exposure rather than any disease process.
Whilst there is a role for the analysis for sIgG in some instances, for example precipitating IgG antibodies for type III immune reactions or IgG tGA/EMA (anti-tissue transglutaminase antibodies/anti-endomysial antibodies) for coeliac disease (CD) in IgA deficient patients, 59 there is no evidence that sIgG is of any benefit in the context of food intolerance or food allergy. It is clear that dietary exclusion based on sIgG results would result in considerable over-treatment and potential harm from unnecessary dietary restriction, especially in children. It is for this reason that many professional organizations, including the National Institute for Health and Care Excellence (NICE) in the UK, recommend against sIgG testing for clinical purposes.40,60–62
The European Academy of Allergy and Clinical Immunology (EAACI) state unequivocally in their position statement of 2008 63 :
Food-specific IgG4 does not indicate (imminent) food allergy or intolerance, but rather a physiological response of the immune system after exposition to food components. Therefore, testing of IgG4 to foods is considered as irrelevant for the laboratory work-up of food allergy or intolerance and should not be performed in case of food related complaints.
Hair analysis for trace elements and minerals
Direct-to-consumer hair tests usually fall into one of two categories: (1) Electrodiagnostic tests for allergy, food intolerance or nutritional ‘imbalances’, (2) Quantitation of minerals, trace elements and/or toxic metals. Electrodiagnostic analysis, commonly known as bioresonance testing, EAV (Electroacupunture According to Voll) or Vega testing, is widely available but has no basis in science whatsoever and will not be considered further here. Direct quantitation of trace elements is usually offered as an all-in-one screen for individuals with nutritional and/or toxicological concerns. Analysis is usually performed using ‘in-house’ assays employing technology such as inductively coupled plasma atomic emission spectroscopy (ICP-AES) or ICP-MS (ICP-mass spectrometry). Reports often include detailed interpretation highlighting nutritional deficiencies or heavy metal toxicities and further investigations that may be required. 64
Hair is an appealing, non-invasive specimen type for toxicological and nutritional screening and has received much interest in this respect. In the 1980s, commercial analysis became popular among some patient groups, especially in the US. However, concerns were quickly raised over the validity and interpretation of results.65,66 It was demonstrated that some US laboratories were reporting vastly different results on identical hair samples from healthy individuals.
65
Many were adding interpretations suggesting ‘nutritional imbalances’ and/or heavy metal toxicity, for which they recommended unnecessary treatments. Warnings, including from the American Medical Association,
67
apparently went unheeded because two similar studies in the US
68
and Germany
69
15 years later showed that little had changed. This spurred the CDC
70
to review the validity of hair element analysis and they listed a range of issues that were contributing to inconsistent results:
Variable collection procedures (site, specimen weight, container) Variable preanalytical preparation (washing, digestion) Method specific variation Lack of standards and QC materials Interferences and sample contamination Poor understanding of biological processes underpinning element incorporation into hair Lack of reference ranges and poor understanding of inter-individual variation Lack of correlation between element levels in hair and target tissues.
Readers are directed to this and other reviews for more detailed analysis of pre-analytical factors.66,71,72 There is evidence that the optimal preanalytical procedure may vary between elements, which makes multi-element analysis problematic. 73,74
Defining reference ranges for hair elements is fraught with difficulty, even where studies are well controlled with large cohorts. 75 In addition to preanalytical issues, results differ with age, race, geographic location, hair colour and sex.66,75,76. It is therefore impossible to judge the appropriateness of reference ranges used by CAM laboratories. The impact of this was demonstrated when South Korean researchers distributed identical hair samples to three laboratories using the same analytical methodology. 77 Whilst the laboratories produced comparable numerical values, their interpretations were wildly different, largely due to variation in reference ranges. There are also questions over conflicts of interest because many CAM laboratories work in collaboration with CAM practitioners who sell treatments on the basis of ‘abnormal’ hair test results. 65
Despite the substantial literature on hair element analysis and its applications, the vast majority of studies have been small and of poor quality. There are few replicated associations between hair element levels and specific disease entities. 78 There is some evidence that hair testing may be useful in environmental studies or at a population level.72,79,80 It has also been applied in cases of severe heavy metal toxicity to retrospectively confirm exposure. 66 However, studies correlating hair element levels to established measures of nutritional or toxicity status on an individual level continue to produce inconsistent results.72,81–83 The CMS National Coverage Determination for hair analysis states: ‘The correlation of hair analysis to the chemical state of the whole body is not possible at this time, and therefore this diagnostic procedure cannot be considered to be reasonable and necessary.’ 84
There remains little evidence to support the use of hair element analysis in routine nutritional or toxicological assessment, especially where tests on other specimen types with an established evidence base are easily accessible.
Antioxidant status
CAM laboratories commonly offer assessments of antioxidant status, ranging from a single analyte, such as reduced glutathione, to panels of vitamins or tests for total antioxidant status using a dye oxidation/reduction method. CAM practitioners and laboratories may claim that free radicals cause or aggravate many ailments, such as cancer, Alzheimer’s disease, heart disease, chronic fatigue syndrome (CFS) and dementia. 85
While free radicals may have a role in many conditions, the relevant question is whether there is any clinical utility in measuring antioxidant status. The only paper to address this question directly found that there was no clinical justification for measuring antioxidant status except for research purposes. 86 A recent review 87 highlights some of the problems with using laboratory biomarkers as proxies for ‘oxidative stress’. Two of the most important reactive oxygen species have half-lives so short (10−9 s for hydroxyl radical and 10−3 s for H2O2 88 ) that they cannot be measured directly. All of the proxy biomarkers of oxidative stress being measured in blood are derived from a variety of organs throughout the body and some may be produced by mechanisms unrelated to oxidative stress. The authors also point out that no regulatory authority has approved any antioxidant supplement for the treatment of any conditions. 87
Despite research showing altered antioxidant or oxidant status in a variety of conditions, and some that shows changed antioxidant status after supplementation, no clinical indications for laboratory measurement of ‘oxidative stress’ or for antioxidant supplementation have been found. The most recent update of the Cochrane review 89 on the subject and a subsequent review 90 have both found no evidence to support the use of antioxidant supplements in the primary or secondary prevention of chronic diseases or mortality. Supplementation with beta-carotene, vitamin A, and vitamin E may actually increase mortality. 90
Urine kryptopyrrole
Measurement of urine kryptopyrrole was first mentioned in the 1960s by biochemist and psychiatrist Dr Abram Hoffer. He found a substance in the urine of alcoholics given LSD as a therapy and also in the urine of people with schizophrenia. 91 The substance gave a purple colour on paper chromatography with Ehrlich’s reagent and so was called ‘mauve factor’. Mauve factor was subsequently shown to be a pyrrole derivative and was renamed ‘kryptopyrrole’, although there has been disagreement as to its identity.92,93
Hoffer and others developed theories about the relationship between mauve factor and vitamin deficiencies and he went on to use high dose ‘megavitamin therapy’ in a variety of psychiatric and neurological disorders. During the 1970s, studies were published showing no relationship between mauve factor and several psychiatric disorders.94–98 A subsequent double-blind study showed no benefit from megavitamin therapy in schizophrenia. 99
Kryptopyrrole and ‘mauve factor’ were discredited as a diagnostic analyte by the 1980s but undeterred, Hoffer founded the Journal of Schizophrenia in 1967 allowing Hoffer and colleagues to publish their work. The journal later changed its name to the Journal of Orthomolecular Medicine.
The urine kryptopyrrole test is widely available and can be ordered ‘direct-to-consumer’ in many countries.100–103 It is marketed suggesting it is useful in the diagnosis of a wide range of conditions, including bi-polar disorder, schizophrenia and depression. There is no evidence in the mainstream peer-reviewed literature that the test is useful in any of these conditions or for any other clinical purpose.
Mitochrondrial function: neutrophil ATP profile
Mitochondrial disorders are uncommon genetic diseases with many neurological and metabolic presentations, including myopathy. Diagnosis is complex, involving molecular genetics and muscle biopsy.104,105 Electron transport activity and mitochondrial content are secondarily affected by many factors, especially physical activity. 105
It has been hypothesized that mitochondrial dysfunction may account for the post-exertional malaise of CFS. One UK laboratory offers an 'ATP profile' that is claimed to correlate with physical disability in CFS. 106 The test may be used to tailor unconventional therapies. 107
Myhill et al. claim that mitochondrial function can be assayed by measuring whole cell ATP levels in neutrophils, with manipulation of magnesium, pH and sodium azide levels. 108 The test has never been independently replicated or validated against established mitochondrial function tests. Patient data were included retrospectively, after the authors had formed the impression it was ‘providing helpful information’. 108 Patients funded the tests; no conflict of interest was declared. Control samples were not paired for physical activity level, and the same control data have been used in several publications.106,107,109
Neutrophils are an unsuitable choice for mitochondrial testing, because they use glycolysis for most energy requirements. The few mitochondria found in neutrophils do not significantly contribute to ATP levels110,111 and their respiratory chain activity is so low that they may serve as a model for certain mitochondrial disorders. 112
Mitochondrial myopathy typically causes elevated CK, 104 which is not a feature of CFS. 113 Validated tests of oxidative phosphorylation/ATP production show no difference in patients with CFS, and clearly distinguish CFS from mitochondrial disease.113,114 Lower mitochondrial density (but not functionality) was seen where the control group was not matched for physical activity, 114 but the difference disappears when a sedentary control group is used. 113 This suggests that any finding of lowered mitochondrial content is a consequence rather than cause of CFS.
Candida testing
Candidiasis hypersentivity syndrome (CHS) is a hypothesized condition ostensibly caused by a systemic reaction to overgrowth of Candida species on mucous membranes or in the gastrointestinal tract. The theory dates to a 1983 book ‘The Yeast Connection’ by an American Physician, William Crook. 115 Proponents claim that low-level colonization with Candida can cause systemic symptoms, such as fatigue, muscle weakness, depression and abdominal bloating. The theory is widely considered disproven but remains popular amongst CAM practitioners. A well designed, double-blind randomized controlled trial of Nystatin therapy for women with symptoms attributed to CHS showed no effect of anti-fungal therapy on symptoms. 116
In addition to supplements and dietary modification, treatments offered to remedy the condition often include potent antifungal agents, such as Ketoconazole and severe iatrogenic complications have been documented in some of these patients. 117
The tests most commonly promoted for the diagnosis of Candida are serological tests and stool tests (often part of a ‘complete digestive/dysbiosis stool profile’). Also available are tests for fungal metabolites, such as serum/urine D-arabinitol, urine tartaric acid and, more recently, urine organic acid profiling. The majority of the available evidence on diagnostic testing for Candida centres on severe fungal infections, such as candidaemia, invasive candidiasis or chronic disseminated candidiasis. Such conditions are usually only seen in immunocompromised patients. It is worth noting the tests recommended by the European Society of Clinical Microbiology and Infectious Diseases for the diagnosis of these conditions: culture, serum mannan/anti-mannan antibodies, serum B-D-Glucan, direct microscopy and histopathology. 118
Screening patients with non-specific symptoms carries a high risk of false positive or clinically irrelevant results. This is because Candida spp. colonization is very common – anywhere between 4–88% of healthy, immunocompetent adults. 119 Stool culture, serological or fungal marker tests therefore frequently give positive results in healthy controls.119,120 Sensitivity and specificity also vary considerably for some tests depending on the methodology used and the cut-offs selected, D-arabinitol being a particularly good example. 120
Studies investigating the role of Candida spp. colonization in the pathogenesis of specific symptoms linked with CHS have consistently failed to show a link. Two frequently quoted studies have suggested a link between Candida spp. and diarrhoeal disease; Talwar et al. cultured Candida spp. in stool of 54.8% of patients with diarrhoea of unknown cause 121 whilst Chaudhury et al. found Candida spp. as the sole pathogen in 15.3% of 978 diarrhoeal stool. 122 Unfortunately, neither assess culture positive rates in control groups and so provide limited information on the pathogenic role of yeasts in these conditions. There are also conflicting studies; Middleton et al. showed that only 3 of 38 patients with IBS symptoms had positive stool cultures for Candida albicans 123 and Mawle et al. showed no difference in Candida serology and fungal markers between 26 chronic fatigue patients and 52 controls. 124
There is no good evidence that urine tartaric acid analysis or organic acid profiling is useful in the diagnosis of fungal infection.
Post-chelator challenge testing
Tests for chronic heavy metal toxicity are popular among individuals with unexplained, non-specific symptoms, particularly those with amalgam fillings or high intake of fish that suspect mercury toxicity, and parents of children with autism. A common approach is to use post-chelator challenge testing (PCCT). This usually involves the patient being sent a kit at home and collecting urine for a variable period of time (practitioners can recommend anywhere from 4 to 48 h) following self-administration of a chelating agent, such as dimercaptosuccinic acid (DMSA), dimercaptopropanesulfonic acid (DMPS), dimercaprol or edetate calcium disodium (CaNa2–EDTA). These agents bind metallic elements from within tissues and are very effective at increasing their excretion from the body. Analysis is usually performed using ‘in-house’ ICP-MS or AES-MS assays, which in some cases have been cleared by the FDA, although not for clinical use.51,125 Elevated results may be interpreted as an indication for ‘detoxification’, sometimes involving powerful chelating agents that can have serious side effects and have caused a number of fatalities.126–129
Even in healthy individuals with no history of exposure, urine metal excretion can increase by up to 10 times following PCCT, depending on the collection strategy.130,131 This appears to be a normal response where non-toxic levels of some metals accumulate in tissues as a consequence of normal background environmental exposure. It is this phenomenon that is often misunderstood and in some cases abused by CAM practitioners and laboratories to suggest metal toxicity where none exists.128,132,133 Indeed, practitioners may recommend a separate unchallenged collection using the difference in results with the PCCT sample to further emphasize ‘toxic burden’. Proponents often claim there is no safe level of exposure to heavy metals but there is little evidence to support this assertion and much to refute it.134–137
Interestingly, where exposure is known to have occurred, there is evidence that post-challenge urine levels of some metals are not significantly higher in exposed individuals versus controls.129,131
Laboratories offering PCCT frequently report post-challenge metal excretion levels against reference intervals derived from unprovoked individuals. This inevitably leads to at least one ‘elevated’ result and opens the door to potential misinterpretation. 133 So far as we are aware validated reference intervals and cut-offs for clinical toxicity do not exist for samples taken post-chelation. 132 Further uncertainty is added by variable pre-test chelation procedures and urine collection protocols.
The most worrying aspect of PCCT is the adverse effects, including fatalities, caused by the chelating agents used both during the test itself and as part of detoxification treatment protocols.126–129
Despite broad criticism from health professionals, toxicologists and regulators, including the FDA and CDC, PCCT remains widely available, particularly in the US. Recent efforts by a US physician to emphasize the misleading nature of PCCT were met with libel lawsuit from a US laboratory after he criticized their PCCT test in an online blog. 138
Secretory IgA
Secretory IgA (sIgA) is produced at mucosal cell surfaces and is readily detectable in stool supernatants, saliva and other secretions. 139 Commercial immunoassay kits are available for the analysis of total sIgA and for specific sIgAs in saliva and stool supernatant. At the time of writing none of these had FDA approval for clinical use but most appeared to be CE marked. 51 Tests using these assays are being promoted by CAM practitioners and websites as a tool to assess immune health with claims that abnormal results may suggest autoimmune disease, asthma, allergy, infection, inflammatory bowel disease, dental caries and many other conditions. The stool test may also be advertised as an alternative for the diagnosis of coeliac disease. 140
Whilst tests for total salivary sIgA have received interest in the literature there is no convincing evidence that analysis is useful in the diagnosis of any condition.139,141–143
The mechanisms underlying the production of sIgA in saliva are not well understood and the relationship to systemic immunity is unclear but there is good evidence that salivary levels do not reflect intestinal humoral immunity. 144 Other factors that may reduce the clinical utility of results include natural variations in salivary flow rate, variable specimen collection protocols and poorly standardized assays.
Initial interest in specific sIgA centred on coeliac antigens (antigliadin, antiendomysium, anti-human transglutaminase) in saliva. However, it soon became clear that diagnostic sensitivity was considerably lower than established serum serology.145,146 Specific salivary sIgA antibodies to infectious disease antigens do show some promise for the diagnosis of specific infectious diseases.139,147,148
Specific sIgA antibodies against gliadin, endomysium and tissue transglutaminase (tTG) are all detectable in the stool of patients with CD. 149 Some early results suggested that stool anti-tTG in particular might help improve upon the diagnostic performance of established serum tests in diagnosing CD. 150 However, when a team in Germany assessed the performance of two sIgA ELISA kits, 140 results were disappointing. They analysed stool samples from 20 children with histologically confirmed CD and 64 controls for sIgA antibodies to gliadin and recombinant human tTG. Even after combining results for both antibodies and optimizing cut-offs, diagnostic performance was still inadequate with sensitivity 82% and specificity 58%. The authors note that performance would be considerably worse in the general population with a much lower pre-test probability of disease.
Testing using sIgA is likely to lead to further unnecessary investigation, anxiety and possibly inappropriate treatment, such as dietary exclusion. Screening for CD using sIgA carries a significant risk of missing a potentially serious diagnosis.
Adrenal stress profile
For the 'adrenal stress profile', patients are asked to collect saliva at several time points during the day which are then analysed for cortisol and DHEAS. Collection and sample handling instructions vary significantly between retailers. Depending on the profile purchased, the patient samples may also be tested for a variety of other hormones, such as testosterone, androstenedione, oestrogens, progesterone, melatonin and even neurotransmitters. For further discussion on the pitfalls of salivary sex steroid analysis, readers are directed to Wood’s 2009 review of salivary steroid assays. 151 It is often unclear what methods are employed by laboratories but there are FDA approved and CE marked immunoassay kits available for salivary cortisol. Interestingly, there are no FDA-approved assays for salivary DHEA/DHEAS but there is at least one that is CE marked. 152
Any alteration in saliva cortisol levels, ratio to DHEAS, or circadian rhythm may be interpreted by CAM laboratories as signifying adrenal dysfunction. This is often used to support the medically-unrecognized diagnosis of adrenal fatigue. Alternative practitioners claim this poorly-defined adrenal dysfunction is caused by chronic physiological or psychological stress, resulting in a variety of non-specific symptoms. There is no consensus on criteria for diagnosis or recommended treatments, though the diagnosis is often used to justify the prescription of nutritional supplements.153,154
Unstimulated saliva cortisol is rarely useful for detecting mild or subclinical adrenal dysfunction. 155 Late-night saliva cortisol has good sensitivity and specificity for Cushing’s syndrome155,156 since it correlates well with the characteristic elevation in blood free cortisol levels. 151 It is less reliable for distinguishing subclinical hypercortisolaemia. 155 In adrenal insufficiency, saliva cortisol after tetracosactide or insulin stimulation shows comparable diagnostic accuracy to serum/plasma cortisol157,158 but unstimulated morning saliva cortisol only distinguishes overt adrenal insufficiency.157,159,160 DHEAS has potential to aid in the diagnosis of adrenal insufficiency, though most research is based on serum measurements where isolated low serum DHEAS level has low specificity for this condition.161,162
Meta-analysis has linked severe chronic psychological stress with altered cortisol circadian rhythm, but there is large inter-individual variation, results are highly dependent on stressor type and duration163,164, and it cannot be assumed that adrenal function itself is altered. 165 There is no evidence that such research translates into a clinically useful diagnostic or prognostic test for individuals. There are no published data validating the adrenal stress profile for the investigation or diagnosis of any condition.
Discussion
We have looked at the evidence base for a range of commonly ordered CAM laboratory tests. There are many others not covered in this review. The common factor in all these tests is the lack of evidence for clinical validity and utility as used in CAM practice. This should not be surprising since this is true for CAM practice in general. Once there is a sound evidence base for an intervention, such as a laboratory test, then it generally becomes incorporated into conventional medical practice.
CAM practice is a huge business. Spending on CAM in Australia in 2016 was estimated to be AUS$3.9bn, 166 in the UK in 2008 £4.5bn 167 and in the US in 2012 US$30.2bn. 168 CAM laboratory practice is a small part of this expenditure and CAM laboratory testing is tiny in proportion to spending on conventional pathology testing. The out-of-pocket costs to individuals however may be high.
CAM laboratory testing is not available via the NHS in UK and is not covered by the national health insurance scheme in Australia but in the US may be covered to some extent by private health insurance plans, Medicare, state Medicaid programmes, and military health insurance plans. 169 In Washington State since 1996, State law has required that private health insurance cover licensed CAM providers. 170 Because CAM laboratories in Australia are not NATA-accredited, patients must pay the full cost of their testing.
Most CAM testing in the UK is carried out privately and not via NHS laboratory services. This does not, however, mean that there is no impact on NHS resources. Most patients receiving an abnormal result from a ‘self-test’ of any kind will consult a doctor 171 and may ask for follow-up investigations or treatment via the NHS. This takes up valuable GP time and may lead to further unnecessary tests or investigations.
It is increasingly recognized that unnecessary diagnostic testing can result in harm to patients.172–174 The risks can vary depending on the test but it seems reasonable to assume that where the test is not clinically valid those risks are increased. CAM tests for heavy metal toxicity have been specifically identified by the FDA as a risk to patient safety because they have been linked to potentially dangerous practices with chelating agents that have led to fatalities.126,128 CAM tests are commonly used to diagnose food intolerances or food allergy and where this leads to inappropriate dietary restriction there is a risk of serious nutritional deficiencies, particularly in children.175–177 Where CAM testing leads to an incorrect diagnosis of bacterial or fungal infection, inappropriate treatment with antibiotic or antifungal agents has been known to cause serious side-effects and even deaths.117,178
Diagnostic testing is increasingly popular amongst CAM practitioners. This has been driven largely by accessibility but there may be some underlying factors that make CAM testing particularly appealing in alternative medicine:
Adding an element of science to the consultation. Patients know that conventional medicine relies heavily on laboratory diagnostics. If the CAM practitioner orders laboratory tests, the patient may feel they are benefiting from a scientific approach. Producing material diagnostic data to support a diagnosis. As discussed previously, CAM lab reports are well presented in a format that is attractive to patients adding legitimacy to a diagnosis. Tests are often ordered as large profiles of multiple analytes. It follows that this will increase the probability of getting results outside of a given reference interval purely by chance. ‘Abnormal’ results give the CAM practitioner something to build a narrative around if clinical findings are unclear. This is particularly relevant for patients who have chronic conditions, such as CFS or fibromyalgia where a definitive cause has not been established and treatment options are limited. Generating business opportunities using abnormal results. Some practitioners may use abnormal laboratory results to justify further testing, supplements or therapies that they can offer. By offering tests that are not available through traditional healthcare services some CAM practitioners may claim they are offering a unique specialist service that their doctor is unable to provide. This can be particularly appealing to patients with unexplained symptoms for which there are a limited range of evidenced-based investigations and treatments available.
Why is CAM so popular in countries with good healthcare and education systems? Despite most of the population having at least high-school level education in the UK, US and Australia, studies have shown that health literacy is still poor.179–181 For most people this makes it difficult to make an informed comparison between the claims of CAM practitioners and the offerings of conventional medicine. While it is commonly believed that people turn to CAM because of the failures of conventional medicine, studies have shown that most people who use CAM are not dissatisfied with their conventional medical care, they just want to extend the range of options available to them.182,183
In this review, we have critically discussed regulation of CAM laboratory testing. This is clearly deficient in all three countries. Where CAM testing is regulated at all, regulatory authorities such as UKAS and MHRA in the UK, CMS, FDA and CDC in the US and TGA in Australia primarily evaluate analytical validity of the tests a laboratory offers. Clinical validity and clinical utility are either not evaluated adequately or not evaluated at all and the ethical, legal and social implications of a test may only be considered on a reactive basis when consumers complain about how tests are advertised.
In Europe, the US and Australia there are proposed regulatory changes that may affect some of the diagnostic tests covered in this review. These changes will introduce requirements for all IVDs to demonstrate clinical validity and there is a particular focus on laboratory developed ‘in-house’ in-vitro diagnostic tests. In the past, most of these types of tests were of a very simple nature. However, this situation is rapidly changing, particularly with the advent of faster and cheaper nucleic acid technology allowing many labs to develop in-house genetic tests and this level of development has also spread to the CAM diagnostics area. In Europe, a revised IVD Regulation is under development which will introduce more stringent requirements on laboratory developed tests that are marketed for clinical use. This will also come with additional obligations on manufacturers to demonstrate clinical validity of their products. The FDA in the US has proposed further oversight of lab-developed tests and has published 20 case studies of faulty lab-developed tests that have resulted in harm to patients.13,184 These case studies include a number of CAM type tests, but also controversially include non-invasive prenatal testing for trisomies. In Australia, the TGA has introduced a regulation that from mid-2017 all laboratories offering in-house or lab-developed tests must be accredited by the NATA, the organization that is currently charged with accrediting all medical laboratories that wish to access Medicare, the national health insurance scheme. 185 In practice, this is likely to remove many in-house CAM laboratory tests from the marketplace in Australia as NATA accreditation requires that tests be shown to have clinical validity and utility as well as analytical validity. 186
Consumers should have freedom of choice in healthcare but should always have access to accurate information about the products they are choosing. This is frequently not the case with CAM testing. Consumers are exposed to poorly regulated diagnostic tests and devices that are being used to make incorrect or misleading medical diagnoses, in many cases leading to inappropriate or harmful treatments. In our view, regulatory oversight of CAM laboratory testing is currently inadequate in all three jurisdictions considered here.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
Not required.
Guarantor
SLJ.
Contributorship
All authors researched the literature, wrote the manuscript, and edited the manuscript.