
Abstract
Background
Congenital disorders of glycosylation (CDG) are a growing group of rare genetic disorders. The most frequently used screening method is sialotransferrin profiling using isoelectric focusing (IEF). Capillary zone electrophoresis (CZE) may be a simple and fast alternative. We investigated the Capillarys™ CDT assay (Sebia, France) to screen for N-glycosylation disorders, using IEF as gold standard.
Methods
Intra- and inter-assay precision were established, and analyses in heparin-anticoagulated plasma and serum were compared. Accuracy was assessed by comparing IEF and CZE profiles of 153 samples, including 49 normal, 53 CDG type I, 2 CDG type II, 1 combined CDG type I and type II and 48 samples with a Tf-polymorphism. Neuraminidase-treated plasma was analysed to discriminate CDG and Tf-polymorphisms using samples of 52 subjects (25 had a confirmed Tf-polymorphism). Age-dependent reference values were established using profiles of 312 samples.
Results
Heparin-plasma is as suitable as serum for CDG screening with the Capillarys™ CDT assay. The precision of the method is high, with a limit of quantification (LOQ) of 0.5%. All profiles, including CDG and Tf-polymorphisms, were correctly identified with CZE. Forty-nine of 52 neuraminidase-treated samples correctly identified the presence/absence of a Tf-polymorphism. Interferences in 3/52 samples hampered interpretation. Sialo-Tf profiles were dependent of age, in particular in the first three months of age.
Conclusions
CZE analysis with the Capillarys™ CDT kit (Sebia) is a fast and reliable method for screening of N-glycosylation defects. Tf-polymorphisms could be excluded after overnight incubation with neuraminidase.
Keywords
Introduction
Congenital disorders of glycosylation (CDG) are a rapidly growing group of rare genetic disorders caused by deficiencies in enzymes involved in the synthesis or remodelling of the carbohydrate backbone of glycoproteins and glycolipids. A total of 105 glycosylation defects have thus far been identified and the number is growing.1,2 Recently, other forms of CDG have been identified with defects in vesicular trafficking, pH homeostasis or Mn2+ homeostasis. CDG is associated with broad clinical phenotypes, for an overview we refer to the recent review of Péanne et al. 1 With a few exceptions, screening of defects in N-glycosylation and combined N- and O-glycosylation defects, leading to diminished end-standing sialic acid, is possible by analysis of sialotransferrin (sialo-Tf) patterns in plasma. To discriminate the isolated N-glycosylation and combined N- and O-glycosylation defects, additional analyses are necessary, for example by sialo-Apo-CIII profiling. Defects in N-glycosylation are caused by defects in glycan synthesis in the endoplasmic reticulum (CDG type I) or by defects in the processing of the glycans, mainly in the GOLGI (CDG type II). Transferrin (Tf) is a plasma iron transport protein, with two asparagine N-glycosylation sites, each having a maximum of four end-standing sialic acid residues. Normally, plasma Tf consists of tetrasialo-Tf, with small portions of penta-, tri- and disialo-Tf. A CDG type I pattern is associated with increased disialo- and often asialo-Tf fractions, whereas most CDG type II are associated with overall Tf hypoglycosylation, frequently with an increased trisialo-Tf fraction. Combinations of CDG type I and II patterns also exist. The most frequently used screening method for CDG is isoelectric focusing (IEF) in combination with immunofixation. Several other analytical methods have been developed to analyse sialo-Tf fractions, including high-performance liquid chromatography (HPLC), capillary zone electrophoresis (CZE), or mass spectrometry (MS).3–5 CZE is a simple and fast method for sialo-Tf analysis. Other studies have already shown that this method is promising with regard to screening for CDG.5–12 The Sebia Capillarys™ CDT kit is developed for diagnosing alcohol abuse. In this method, Tf isoforms are separated in silica capillaries by electrophoretic mobility and electro-osmotic flow at high voltage in an alkaline buffer. A specific diluent is used to allow for saturation of Tf with iron. Sialo-Tf fractions are detected during migration by UV absorbance. The Capillarys 2™ is fast compared with IEF; in our experience, it is able to analyse up to 28 samples per hour. No sample preparation is required with the CDT kit, in contrast to other CZE methods. Until now, only two papers appeared on the application of this specific CDT kit for CDG screening.7,10 The number of patients was, however, very low in both papers, i.e. two 7 and eight patients, 10 respectively. In this paper, we investigated the value of the CDT method for screening of N-glycosylation disorders, using IEF as gold standard and determined reference values. In addition, we compared two sample types, i.e. heparin-anticoagulated plasma and serum, and investigated the possibility to confirm Tf polymorphisms with CZE after treatment of plasma with neuraminidase.
Materials and methods
IEF analysis
IEF of serum or plasma Tf was performed essentially as described by Van Eijk and Van Noort. 13 In short, 10 μL plasma was incubated with an Fe(III)-citrate solution to saturate Tf with Fe(III). Supernatant (1 μL) was subsequently applied on a polyacrylamide gel with a pH gradient of 4.0–6.5 (PhastGel, GE Healthcare Bio-Sciences). After electrophoresis (2000 V), Tf is immunofixated using Rabbit antihuman Tf and coloured using Coomassie Brilliant Blue R250.
CZE analysis
Multicapillary CZE was performed on a commercially available system (Sebia, Capillarys 2™, France). Seven silica capillaries operate in parallel (effective length 17.5 cm × 25 μm I.D.), and detection of the sialo-Tf occurs with UV detection at 200 nm wavelength. All reagents were provided in a commercial kit named Capillarys™ CDT assay, including buffer solution, wash solution, sample diluent and plastic consumables. Data analysis was performed with the software package Phoresis 8.6.3 (Sebia, France).
Validation of CZE analysis
Comparison heparin-anticoagulated plasma and serum sialo-Tf profiles
Samples of 48 subjects with normal sialo-Tf profiles were used to compare sialo-Tf profiles in heparin-anticoagulated plasma and in serum. Samples were analysed and compared by Passing-Bablok regression analysis.
Intra- and inter-assay precision
Three samples were used for precision studies: (1) commercial normal control (Sebia, CDT), (2) a heparin-anticoagulated plasma sample of a patient with a CDG type I profile and (3) a heparin-anticoagulated plasma sample of an apparently healthy person without a Tf polymorphism. Samples were analysed in a single day (seven times; once in each capillary) to calculate intra-assay variation and each capillary once per day for 8–10 days to calculate inter-assay variation per capillary and their mean variation as representative of the inter-assay variation. The coefficients of variation (CV) were calculated by dividing the standard deviation by the mean (SD/mean × 100%).
Accuracy
Accuracy was assessed by comparing IEF and CZE profiles of 153 anonymized samples, including 49 reference samples, 48 samples of subjects with a Tf-polymorphism, 53 samples with a CDG type I profile, i.e. 48 samples from CDG type I patients and 5 samples from a patient with hereditary fructose intolerance [HFI]), 2 samples from a CDG type II patient and 1 sample from a patient with a combined CDG type I and II pattern. The CDG type I population consisted of 17 PMM2-CDG, 15 PMI-CDG, 6 ALG6-CDG, 6 ALG12-CDG and 3 patients with a CDG type I profile (definitive genetic diagnoses not established due to loss to follow-up). The patient with the CDG type II pattern had no genetic diagnoses yet, but no Tf polymorphism was demonstrated; the profile was consistent in all available samples and the patient had a highly abnormal sialo-Apo-CIII profile confirming a CDG. The patient with a combined CDG type I and II pattern was diagnosed with PGM1-CDG. Most samples with a Tf-polymorphism or with CDG type I and/or II profiles were previously examined by IEF and reanalysed with CZE. These samples were stored deep frozen for a maximum period of 15 years in −80°C. The other data derived from patients suspected of a CDG, whose samples were prospectively analysed in the context of diagnostic procedures with both IEF and CZE.
Reference values
Reference values were calculated using 312 samples analysed by CZE with a normal sialo-Tf profile. Samples derived from patients whose samples were analysed in the context of diagnostic procedures. Age dependency was assessed by Spearman Rank tests (at P < 0.05), and by visual inspection of the relation between age and sialo-Tf fraction. Ninety-five per cent reference values were calculated as 2.5 to 97.5 percentiles.
Neuraminidase treatment
An additional set of 52 samples were treated with neuraminidase, of which 25 had a Tf polymorphism on IEF (25 controls) and 27 had no Tf polymorphism on IEF (17 CDG patients, 10 controls). Heparin-anticoagulated plasma samples (90 μL) were incubated at room temperature (20–25°C) overnight with 10 μL (5 U/110 μL MilliQ water) neuraminidase (Roche Diagnostics International Ltd, Mannheim, Germany). Samples were analysed with CZE and qualitatively compared with results produced earlier with IEF. We did not aim to fully characterize the Tf-polymorphisms.
Ethical statement
The conducted research is not related to human use as meant in the Medical Research involving Human Subjects Act, since we made use of coded samples that were already used for similar diagnostic purposes. The study design was in accordance with the current revision of the Helsinki Declaration.
Results
Comparison between heparin-anticoagulated plasma and serum CZE profiles
No significant bias was found between serum and heparin-anticoagulated plasma samples (n = 48) by Passing-Bablok analyses (P < 0.05). The correlation coefficients were 0.988 (pentasialotransferrin [S5-Tf]), 0.990 (tetrasialotransferrin [S4-Tf]), 0.998 (trisialotransferrin [S3-Tf]) and 0.932 (disialotransferrin [S2-Tf]). Percentages of monosialotransferrin (S1-Tf) and asialotransferrin (S0-Tf) fractions were too low for statistical analyses.
Intra- and inter-assay precision
Intra- and inter-assay precision are presented in Table 1. Sialo-Tf fractions had coefficients of variation (CV) between 0.1% and 19.6%. The CV was mainly dependent on the amount (percentage) of sialo-Tf present in the sample. The S5-Tf fraction had relatively high inter-assay variability compared with other fractions at similar amounts (percentages) present. Fractions below 0.5% seem to reach the limit of quantification (LOQ) defined as an imprecision >20%.
Intra- and interday precision of sialotransferrin fractions with CZE.
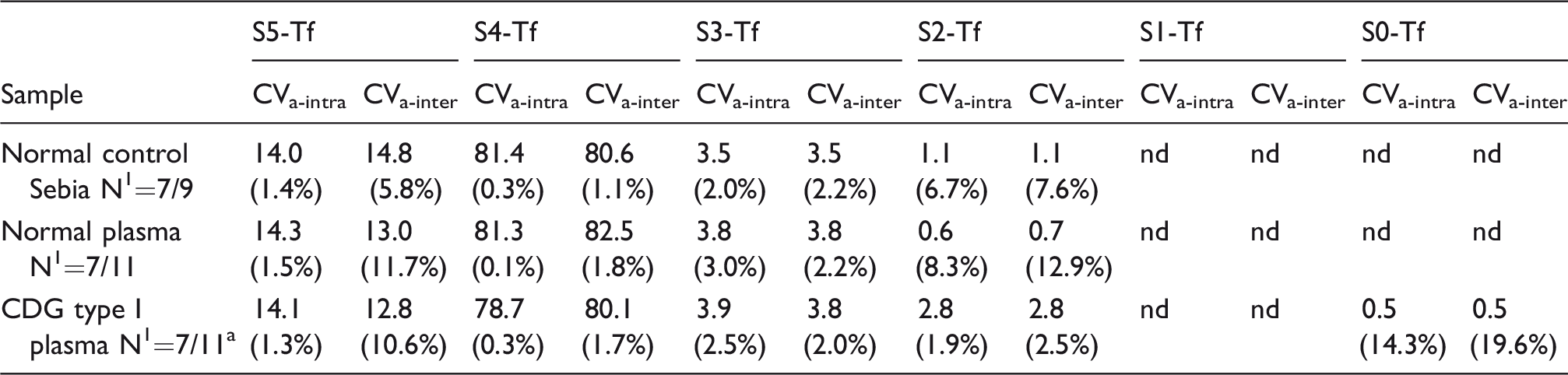
Note: Sialo-Tf fractions are notated as S5-Tf to S0-Tf.
Of the CDG type I sample, 11 samples were analysed for CVa-inter for capillaries 1,3,6 and 10 samples for capillaries 2,4,5,7.
CVa-intra: intra-assay variation; CVa-inter: inter-assay variation; Numbers (N) represent numbers for CVa-intra/numbers for CVa-inter .
Values represent mean fractions (sialo-Tf %) and in parentheses the corresponding variation coefficients (CV%).
Accuracy
Figure 1 (left) shows six examples of the various patterns analysed in our sample set, e.g. profiles of a control (1a), two CDG type I patients (1b and 1c), a CDG type II patient (1d) and two subjects with a Tf polymorphism (1e, 1f).
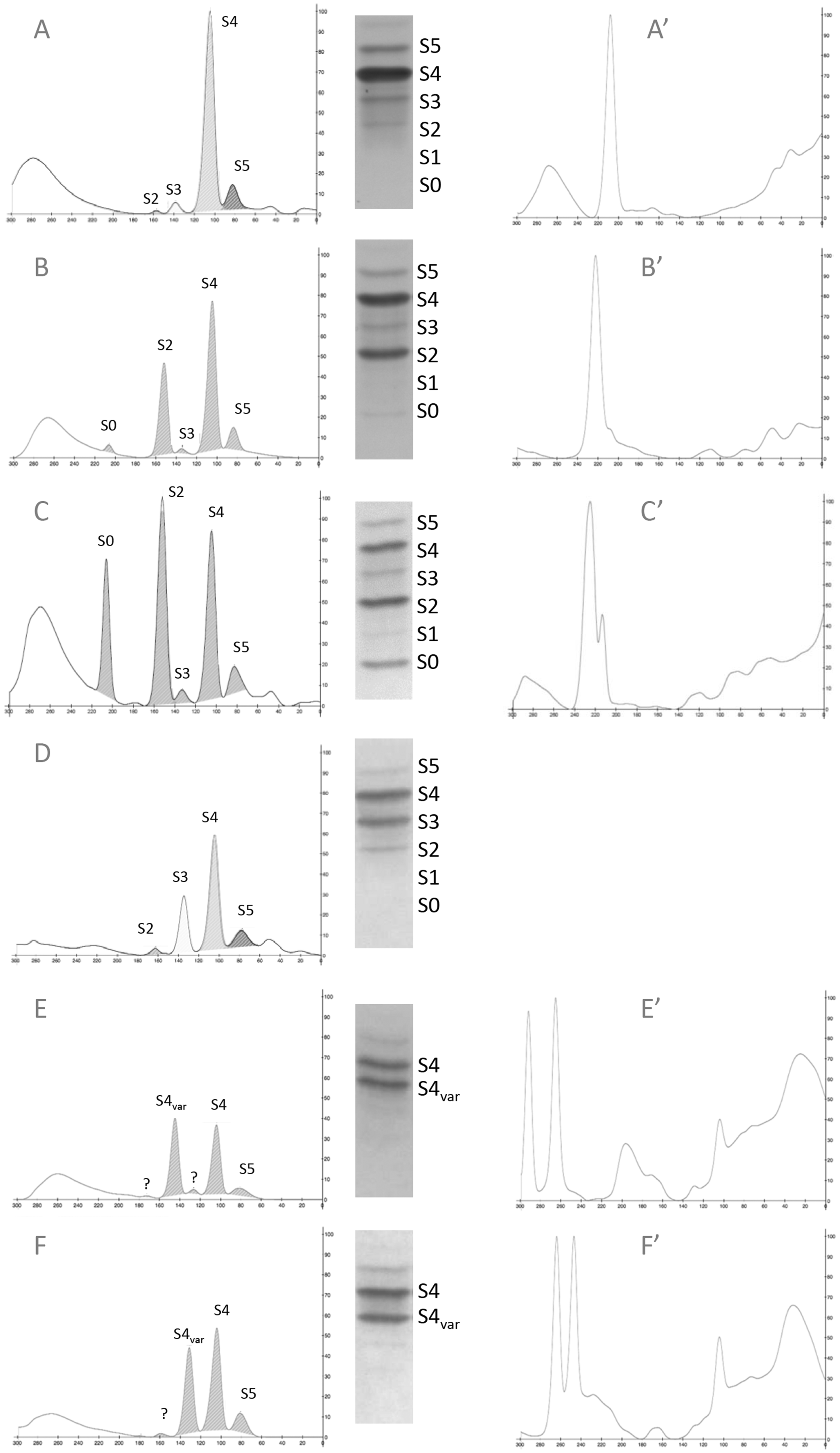
Examples of sialo-Tf profiles with CZE.
Of the 153 plasma samples that were analysed with both IEF and CZE, 105 samples could be quantified, i.e. 49 samples with a normal pattern (S0-Tf range: 0.0–0.4%, S1-Tf 0.0–0.0%, S2-Tf 0.0–1.1%, S3-Tf 0.0–12.8%, S4-Tf 72.6–99.1%, S5-Tf 0.9–20.0%), 45 samples of CDG type I and HFI patients (S0-Tf range: 0.0–38.2%, S1-Tf 0.0–1.4%, S2-Tf 3.1–53.7%, S3-Tf 0.0–8.4%, S4-Tf 10.2–90.7%, S5-Tf 1.4–21.3%), 8 samples of PMI-CDG (n = 3) and HFI (n = 1) patients under treatment, i.e. liver transplant or mannose for PMI-CDG and fructose- and sucrose-free diet for HFI (S0-Tf range 0.0–0.0%, S1-Tf 0.0–0.0%, S2-Tf 0.4–3.0%, S3-Tf 1.6–8.7%, S4-Tf 74.6–82.5%, S5-Tf 12.5–17.6%), 2 samples of a CDG type II patient (S0-Tf range 0.0–0.0%, S1-Tf 0.0–0.0%, S2-Tf 2.6–2.7%, S3-Tf 26.8–27.8%, S4-Tf 58.3–61.0%, S5-Tf 8.5–12.3%) and 1 sample of a PGM1-CDG patient with a combined CDG type I and II profile (S0-Tf range 2.5%, S1-Tf 0.0%, S2-Tf 10.3%, S3-Tf 9.6%, S4-Tf 62.3%, S5-Tf 15.3%). In these 105 samples, all without Tf-polymorphisms, significant biases between CZE and IEF were found for all fractions, except for S0-Tf (r = 0.947). Bias and correlation coefficients (r) were as follows: S5-Tf (CZE = 0.53×IEF + 3.5, r = 0.627), S4-Tf (CZE = 1.18×IEF, r = 0.891), S3-Tf (CZE = 0.61×IEF−1.4, r = 0.893) and S2-Tf (CZE = 0.89×IEF−1.8, r = 0.968). S1-Tf was absent in most samples, and therefore statistical analyses were not possible for this fraction. All CDG patients had abnormal profiles with both IEF and CZE, and all controls had normal profiles with both methods; diagnostic accuracy of CZE compared with IEF was 100%. Tf-polymorphisms (n = 48) were left out in these analyses, because sialo-Tf fractions could not be quantified.
Tf polymorphisms were recognized with both CZE and IEF, but eluted differently. With IEF, three polymorphisms were identified in our samples, with the S4-Tf variant appearing nearby S5 (n = 28), S3 (n = 17) or S0 (n = 3). The variant eluting nearby S5-Tf with IEF appeared nearby S3-Tf with CZE (data not shown). The variant eluting nearby S3-Tf with IEF eluted with CZE nearby S2 (n = 11/17, see Figure 1(e)) or S3 (n = 6/17, see Figure 1(f)). This separation probably results from separation of the different so-called Tf-D variants, as demonstrated by Caslavska et al. 14 The variant S4-Tf that eluted at S0 position with IEF was not detected with CZE (a normal profile was shown).
Neuraminidase treatment
Figure 1 (right) shows profiles of five samples after treatment with neuraminidase. Samples before and after neuraminidase treatment are displayed in the same row, i.e. Figure 1(a′) is the neuraminidase-treated sample of Figure 1(a). Unfortunately, there was not enough sample left to perform neuraminidase treatment on sample 1C (CDG type II).
Fifty-two samples were treated with neuraminidase, of which 27 had no polymorphism. In 25 of these 27 samples, either with a normal pattern (Figure 1(a)) or a CDG type I pattern (Figure 1(b)), a single peak migrating cathodic to S0-Tf appeared after neuraminidase treatment (Figure 1(a′) and (b′)). In 2/27 samples, an interfering compound appeared. In four samples, all of confirmed CDG patients with a relatively large S0-fraction, two co-eluting peaks were shown (see Figure 1(c′)). All other samples showed a single peak. In 24/25 samples with a Tf polymorphism (Figure 1(e) and (f)), two baseline-separated peaks migrating cathodic to S0-Tf appeared after neuraminidase treatment (Figure 1(e′) and (f′)), demonstrating the presence of a Tf variant. Interpretation of the profile was not possible in 1/25, because of an interfering compound eluting nearby asialo-Tf.
CZE and IEF in a patient with a mildly abnormal CDG type I pattern
Figure 2 shows CZE and IEF profiles of an ALG12-CDG (CDG-1g) patient at 3 days and 46 days of age (neuraminidase profiles were normal), demonstrating the accuracy of the CZE method in diagnosing mild CDG profiles. The CZE profile was clearly abnormal at both days 3 and 46, whereas the IEF profile at day 3 was less pronounced. The S2-Tf fraction with IEF was 2.4 times the upper reference limit (URL), whereas it was 8.3 times the URL with CZE.
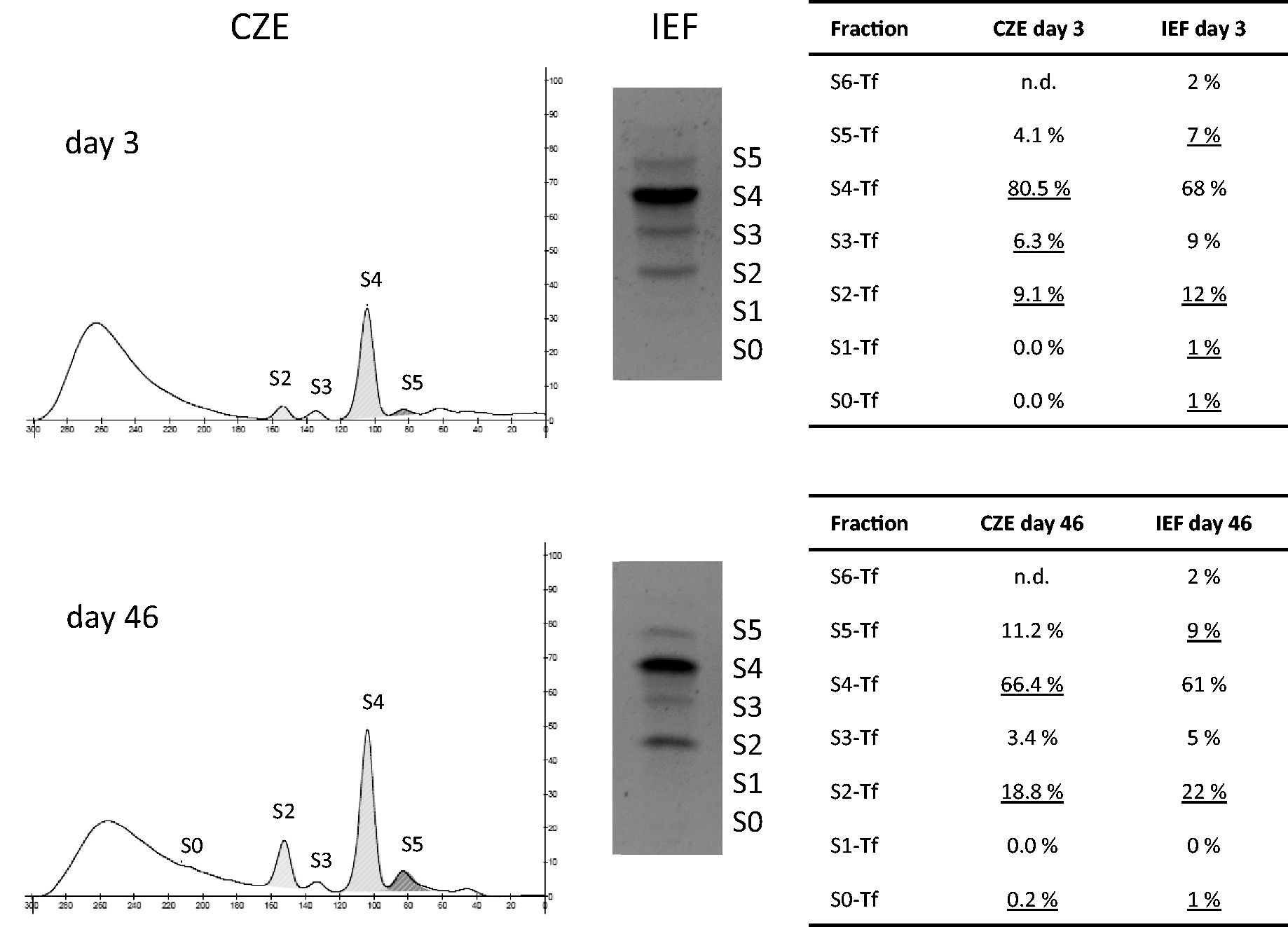
CZE and IEF sialo-Tf profiles of CDG type I patient.
Reference values
The mean (range) age of the reference group (n = 312) with normal profiles was 5.7 (0.0–52.5) years. Sialo-Tf fractions were significantly age dependent mainly in children below three months of age. After this age, S4- and S3-Tf fractions slightly increased at the expense of S5-Tf and some S2-Tf until approximately the age of 5 years, but this did not affect the upper limits of the reference values to a clinically significant extent. We decided to calculate the reference values for all ages, using 2.5 and 97.5 percentiles, see Table 2.
Reference values of Tf-fractions with CZE.
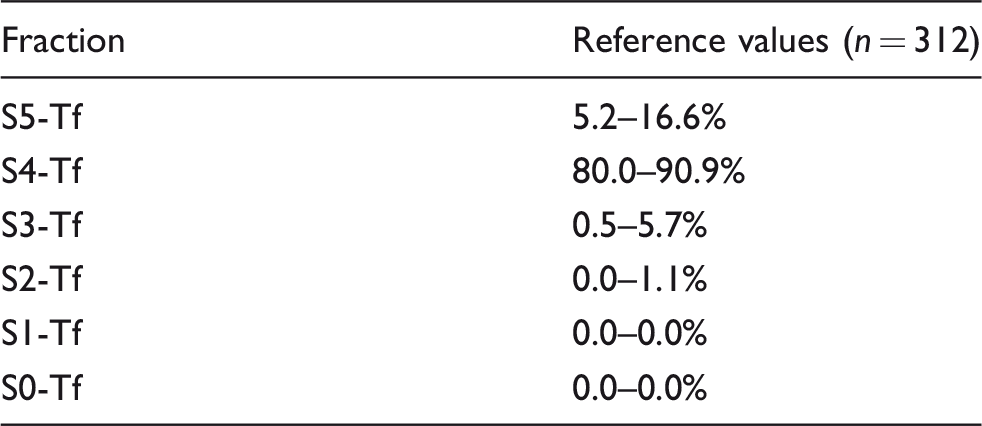
S0-Tf: asialotransferrin; S1-Tf: monosialotransferrin; S2-Tf: disialotransferrin; S3-Tf: trisialotransferrin; S4-Tf: tetrasialotransferrin; S5-Tf: pentasialotransferrin.
Discussion
We investigated the value of the CDT method for screening of N-glycosylation disorders, using IEF as gold standard, and determined reference values. We additionally compared the use of heparin-anticoagulated plasma with serum and the possibility to investigate Tf polymorphisms with CZE after treatment of plasma with neuraminidase.
At this moment, IEF is the most common applied method to screen for N-glycosylation and combined N- and O-glycosylation defects. 4 Our results showed that CZE with the CDT method is a good and simple alternative for CDG screening compared with IEF. The method requires much less hands-on time compared with IEF. All abnormal profiles, i.e. CDG or Tf-polymorphisms, were correctly identified with CZE, using heparin-anticoagulated plasma. The precision of the method is high. Hexasialotransferrin (S6-Tf), often visible when analysing samples with IEF, could not be detected with certainty with the Sebia CZE method. The precision of the method decreases when fractions drop below 1%, and the LOQ is reached when fractions are below 0.5%. The precision of the CZE method is better compared with the precision with our IEF method, which has CVs varying from 3.0% for high abundant fractions (70%) to 36% for low abundant fractions (1.4%), with an LOQ of approximately 6%. CZE has therefore at least similar sensitivity to recognize so-called mild CDG type I profiles. This is further illustrated by the results of a plasma sample with a mild CDG type I profile, see Figure 2. Earlier reports showed that the precision of CZE with the Capillarys 2™ of Sebia is also one of the highest compared with other CDT methods. 15
Even though CDG screening is possible with this readily available technique, screening of these rare inborn errors should always be an integral part of metabolic screening in genetic metabolic laboratories. CDG screening alone is never sufficient to screen for patients with the aspecific symptoms that accompany these different diseases. There are only a very few CDG types whose symptoms may directly point at a CDG, and also in these patients, abnormal screening should always be confirmed in specialized laboratories.
Heparin- or EDTA-anticoagulated plasma is most often applied in genetic metabolic laboratories. Use of EDTA-plasma is not recommended by Sebia. From the relations between serum and heparin-anticoagulated plasma in normal profiles, and from the agreement between CE and IEF methods in patients and controls with heparin-anticoagulated plasma, we showed that heparin-anticoagulated plasma is as good as serum for screening with the CDT method, i.e. heparin did not invalidate quantification of (low) sialo-Tf fractions.
It was previously suggested that CZE is a good alternative to IEF for CDG screening.6–12 The largest study performed thus far on the use of CZE for CDG screening was performed by Carchon et al. 6 They demonstrated in 792 CZE analyses using the CEofix™-CDT kit (Analis, Namur, Belgium) on a Beckmann Coulter P/ACE 5000 system that all abnormal profiles and confirmed CDG samples were correctly identified by CZE. Only two papers have previously analysed the performance of the CDT kit for CDG screening on a Sebia Capillarys™,7,10 and both papers showed that CDG patients were correctly identified with the CDT kit; however, the number of patients investigated was very low, i.e. two 7 and eight, 10 respectively. Our results with a larger population of CDG patients are in agreement with the good performance for analysing CDG. The Capillarys CDT method has the advantage above the CEofix™-CDT kit that iron saturation is not necessary before loading the sample on the capillaries, thereby reducing sampling handling and increasing automation.7,10
An important factor to consider when analysing sialoTf-fractions is the existence of Tf (micro)heterogeneity due to Tf polymorphisms. These polymorphisms affect the isoelectric point of Tf, and therefore interfere with the interpretation of sialo-Tf profiles. 4 In CZE, these polymorphisms also hamper interpretation, in particular since the profiles seem comparable to CDG profiles (also see Figure 1). The S4-Tf variant appearing at S2-Tf with CZE (see Figure 1(e)) might be confused with a CDG type I profile (Figure 1(b) and (c)), in particular in CDG patients with an absent S0-Tf fraction. These profiles may be differentiated in most samples by the variant S3-Tf appearing at the S1-Tf position in Tf polymorphisms only. The S4-Tf appearing at the S3-Tf position with CZE (Figure 1(f)) is highly comparable to the pattern of the CDG type II patient, a very rare group of disorders (Figure 1(d)). The ratio of the S4-Tf and the variant S4-Tf may give a clue to diagnoses, since in (most) Tf polymorphisms, the ratio is approximately 50%. There are however exceptions, because of mixed profiles in the presence of a Tf variant. To differentiate a CDG type I or a mixed CDG type I and II profile from a Tf polymorphism with certainty, we recommend to repeat the analysis after incubation of plasma with neuraminidase. With IEF analysis, it is already good practice to re-examine abnormal sialo-Tf profiles after incubation of serum or plasma with neuraminidase to investigate whether the abnormalities are due to a Tf polymorphism. 4 Neuraminidase cleaves sialic acid groups of Tf, leaving only asialo-Tf fractions. In case of a heterozygous Tf polymorphism, two bands instead of one appear, proving that the abnormal profile was at least partly due to a Tf polymorphism. Two papers were published, showing the potential to characterize Tf polymorphisms with CZE using the CEofix™-CDT kit (Analis, Belgium) on a PA800 CE system of Beckman Coulter (Fullerton, CA, USA).14,16 Identification of the specific Tf variant was not the aim of our study, we were particularly interested to see if neuraminidase treatment could differentiate the Tf polymorphisms from the CDG patients. In this way, a reduction in the number of patients who need CDG confirmation and subtype specification in specialized laboratories can be achieved. We showed that Tf polymorphisms could indeed be differentiated from CDG profiles when analysing neuraminidase-treated samples with the Sebia CDT kit on the Capillarys 2™. Three samples showed an interference (only) after treatment with neuraminidase. These profiles could not be interpreted and should be reanalysed using an alternative method. No such interferences were shown in samples that were stored up to three weeks; it is as yet unknown if the interferences are due to degradation of proteins during long-term storage of the samples. In theory, a Tf-polymorphism may be present in a patient with a CDG. In case of doubt, analysis with an alternative method to confirm the presence of a CDG, for example mass-spectrometry, may be necessary. Interestingly, in CDG type I patients, two co-eluting S0-fractions are present after neuraminidase treatment. This effect is most pronounced in samples with relatively high asialo-Tf. The two fractions after neuraminidase treatment seem to appear in CDG type I patients only, probably because naturally occurring asialo-Tf without glycan chains is present next to the neuraminidase cleaved Tf with glycan chains. The absence of glycan chains is likely to affect electrophoretic behaviour.
Quantitative differences between IEF and CZE methods exist; therefore, specific reference values for CZE need to be determined. The current method is sensitive even at low sialo-Tf fractions revealing a relation between plasma sialo-Tf fractions and age, in particular in the first year of life. Most remarkably, S3-Tf and S5-Tf increase with age, as previously shown by Zamboni et al. 12 Changing serum N-glycan profiles with age is already known, 17 although the physiology is not yet completely understood.
The main limitation of the CZE method is the occurrence of mainly unknown interferences, because of the non-specific detection of compounds (mainly peptide bonds) at 200 nm. According to the manual of the Capillarys™ CDT assay, immunoglobulins (appearing anodic to S0-Tf), C-reactive protein, C3d protein due to complement 3 degradation (appearing cathodic to S5-Tf), haemolysis, high fibrinogen and substances in samples of patients with severe liver disease also interfere. Interferences were also found in samples of patients with several types of cancer, including lung, breast and colorectal carcinoma. 18 Total bilirubin, triglycerides, cholesterol and haemoglobin did not interfere up to concentrations of 256.5 μmol/L, 9.41 mmol/L, 10.87 mmol/L and 1.5 g/L, respectively. 19 To diminish the effects of interferences, Sebia provides a treatment reagent. No interferences hampering interpretation were identified in the analysed samples (without neuraminidase treatment). In case such an interference appears, we recommend reanalysing samples with IEF or N-glycan mass-spectrometry. All samples with CDG type I and/or type II profiles should also be confirmed enzymatically or genetically by follow-up testing in reference laboratories.
We conclude that CZE is a fast and reliable method for screening of N-glycosylation defects in serum or heparin anticoagulated plasma samples. Samples can be investigated with CZE for Tf polymorphisms after overnight incubation with neuraminidase.
Footnotes
Acknowledgements
Koos van de Belt is gratefully acknowledged for his help with starting up the Capillarys™ CDT assay on the Capillarys 2™.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
The conducted research is not related to human use as meant in the Medical Research involving Human Subjects Act, since we made use of samples that were already used for similar diagnostic purposes. The study design was in accordance with the current revision of the Helsinki Declaration.
Guarantor
MRH-F.
Contributorship
HK and FvdS were responsible for analytical measurements. HK contributed to the planning of the experiment, analytical measurements and writing parts of the manuscript. RH-F was responsible for the study design and the writing of the manuscript. All authors critically read the manuscript and approved the final version.