
Abstract
Anaemia is a condition in which the number of red cells necessary to meet the body's physiological requirements is insufficient. Iron deficiency anaemia and the anaemia of chronic disease are the two most common causes of anaemia worldwide;1 iron homeostasis plays a pivotal role in the pathogenesis of both diseases. An understanding of how iron studies can be used to distinguish between these diseases is therefore essential not only for diagnosis but also in guiding management. This review will primarily focus on iron deficiency anaemia and anaemia of chronic disease; however, iron overload in anaemia will also be briefly discussed.
Iron homeostasis
The average human adult contains approximately 3 to 4 g iron.1,2 There is no excretory system for iron (aside from blood loss and mucosal shedding – which is not regulated by homeostasis), so absorption of iron from the gastrointestinal system is tightly controlled.
Iron absorption into the enterocyte occurs primarily in the terminal duodenum through the divalent metal transporter (DMT1). 3 Export of iron from the enterocyte is through the basolateral membrane by ferroportin-1. 4 Ferroportin-1 is also highly expressed at sites involved in iron transfer including macrophage membranes and the sinusoidal surfaces of hepatocytes. 5
Once iron is released from the enterocyte, it is transported to sites of usage and storage by transferrin. 2 Transferrin is a 75–80 kDa glycosylated protein that can carry up to two ferric ions; under physiological conditions around 30–40% of the iron-binding capacity of transferrin is used. 6 Transferrin then delivers the bound iron through transferrin receptor-1 (TfR1) to the sites of usage and storage; TfR1-mediated iron import is the main pathway used by erythrocytes and hepatocytes. 7 Iron transport into the macrophages of the reticuloendothelial system (RES) is primarily through erythrophagocytosis of senescent red blood cells. 6
Free iron is cytotoxic; if it is not immediately utilized after internalization, it will associate with ferritin, the main iron storage protein in the body. 8 The main site for iron storage is within the macrophages of the RES (particularly of the liver, spleen and bone marrow) and hepatocytes. 6 Export of iron from sites of storage is through ferroportin-1.
Regulation of iron homeostasis is mainly via iron regulatory proteins (IRP)/iron responsive elements (IRE) and hepcidin. The former control uptake and storage of iron, while the latter regulates iron export. Hepcidin plays a central role in iron homeostasis through its effect on ferroportin-1; after hepcidin binds to ferroportin-1, ferroportin-1 is internalized and degraded by lysosomes; the overall effect is to decrease ferroportin-1 expression and block iron export. 9
It is beyond the remit of this review to fully cover iron homeostasis, a recent review by Tomas Ganz 2 provides a comprehensive overview of this topic.
Iron studies
Iron studies are a panel of tests used to assess the amount of circulating iron and storage iron. These tests should be interpreted together. Below is a summary of the routine iron studies performed in most laboratories.
Ferritin
As the main iron storage protein in the body, the majority of ferritin is intracellular. However, a soluble form is found in the blood and can be assayed. 10
Ferritin concentrations vary by age and gender. From adolescence, males have higher values than females, a trend that persists into late adulthood. In females, ferritin concentrations remain relatively low until menopause and then rise. 11 In both sexes, ferritin increases from around 70 years of age. 12
A ferritin concentration <15 μg/L in adults 13 is diagnostic of iron deficiency. An elevated ferritin may reflect iron overload; however, ferritin is an acute phase protein, so may also be increased in liver disease, malignancy, infection and inflammation. 14 Therefore, a normal ferritin concentration alone does not necessarily exclude iron deficiency.
Serum iron
Serum iron is a measure of the amount of iron bound to transferrin in the plasma. Only a small proportion of the body's iron is bound to transferrin at any one time. 15 There is a rapid turnover of transferrin-bound iron and circulating iron concentration can be affected by dietary intake; as a result, there is significant variation in iron concentration within each day and between days. 16 For this reason, assessment of serum iron alone provides little helpful clinical information.
Total iron-binding capacity/transferrin
Total iron-binding capacity (TIBC) is an assay which determines the amount of iron that can be bound to unsaturated transferrin, i.e. the total number of transferrin binding sites per unit volume of plasma or serum. Historically, it was assessed by adding an excess of iron to plasma and measuring the amount of iron retained. 17 Therefore, TIBC is a proxy measure of transferrin.
Unlike serum iron, TIBC does not have rapidly changing concentrations in the plasma. However, it is not a useful marker of early iron deficiency as values do not change until stores are depleted. 18
Transferrin is the transporter protein for iron and its concentration can be determined by immunological methods. 18 Both TIBC and transferrin rise in iron deplete states and fall in inflammatory and iron overload disorders.
Transferrin saturation
This is derived by dividing serum iron by TIBC. As the name suggests, it is the percentage of transferrin bound to iron. In iron deplete states, the amount of iron is reduced and therefore the transferrin saturation will be reduced (and vice versa). A transferrin saturation of <15% in association with an elevated TIBC is indicative of iron deficiency anaemia. A transferrin saturation of >45% is suggestive of iron overload and will usually require further investigation. 19 As previously mentioned, the variation in plasma concentration of iron is considerable, and therefore, there will be daily variation in the transferrin saturation; as a result, transferrin saturation must be interpreted alongside other iron studies.
Iron deficiency anaemia
Iron deficiency anaemia is due to the lack of sufficient iron to form normal red blood cells; it is the most common cause of anaemia worldwide. 1 Iron deficiency may be the result of blood loss, inadequate dietary intake or malabsorption. The gold standard for diagnosing iron deficiency is the absence of stainable iron on bone marrow biopsy; however, this is impractical, and iron deficiency is usually assessed by laboratory parameters on a peripheral blood sample.
Laboratory diagnosis of iron deficiency anaemia
Full blood count and blood film
By WHO criteria, anaemia is defined as a haemoglobin concentration (Hb) of <120 g/L in a female or <130 g/L in a male. 13 In the early stages of iron deficiency, haematopoiesis is not affected; as stores diminish further, the red cells become microcytic first and then hypochromic before the Hb falls. As well as microcytosis and hypochromia, the blood film may feature poikilocytosis (variation in shape, including pencil cells) and anisocytosis (variation in size). 20 Microcytosis is reflected in the full blood count (FBC) as a reduction in the mean cell volume (MCV) and hypochromia as a reduction in the mean cell haemoglobin concentration.
Iron studies
Hepcidin feedback is regulated by concentrations of iron; in iron deplete states, circulating concentrations of this hormone fall. 21 As hepcidin falls, ferroportin expression increases, leading to increased absorption of iron from enterocytes and increased iron export from storage cells. The IRP/IRE system also works to reduce the conversion of cytosolic iron into ferritin. Lastly, in order to optimize delivery of exported iron to areas of high demand, the production of transferrin is upregulated in the liver.
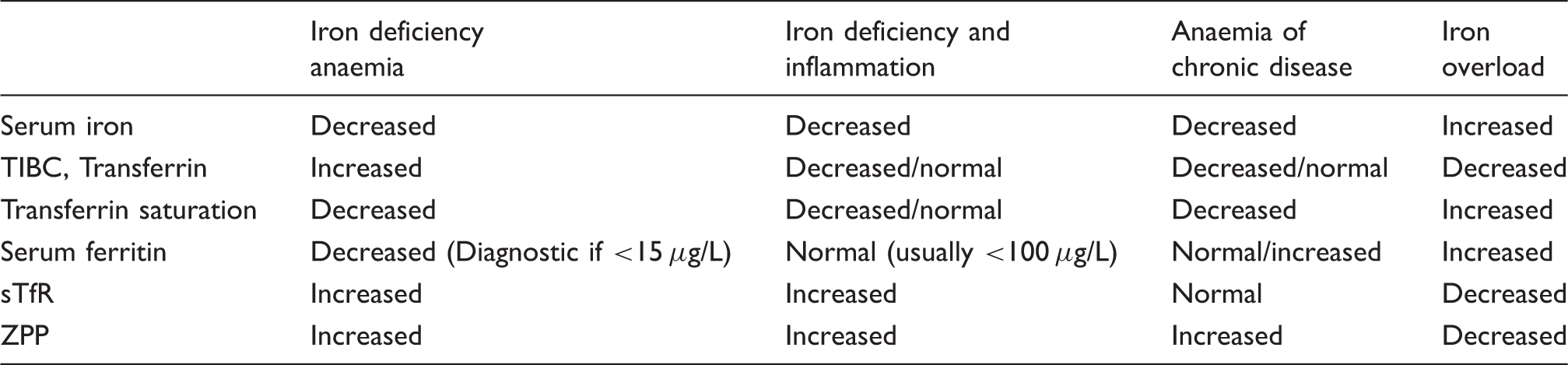
Iron studies can reflect this physiological response. Circulating transferrin and TIBC are elevated. Serum iron falls; the relative decrease in supply compared with demand reduces the circulating pool. Transferrin saturation is reduced (typically <15%) due to increased TIBC and reduced serum iron. The increased export of iron from stores and decreased ferritin production lead to a fall in circulating ferritin; a concentration of <15 μg/L is diagnostic of iron deficiency. 13
Interpretation of biochemical tests in diseases of iron status.
There are assays which can be helpful in diagnosing iron deficiency in cases when it is not clear from conventional iron studies; these are discussed below.
Soluble transferrin receptor
Soluble transferrin receptor (sTfR) results from the proteolysis of TfR and occurs following the binding of transferrin to TfR, this produces monomers that are measurable in plasma or serum. The concentration of sTfR is therefore an indirect measure of total TfR. 24 TfR-mediated iron import is the main pathway used by erythrocytes and hepatocytes; most TfRs are located on erythroid progenitors. 25 As a result sTfR concentration is believed to reflect erythroid turnover and is determined by erythroid proliferation rate and iron demand; sTfR concentrations will increase in iron deficiency. 26 Concentrations can also be increased in other high erythroid turnover states such as haemolytic anaemia and thalassaemia. 27
Unlike ferritin, sTfR is not an acute phase reactant, so serum concentrations do not rise in inflammatory states; therefore, sTfR can be useful in diagnosing iron deficiency in such cases. In addition, sTfR/log ferritin index can be useful in diagnosing early iron deficiency and may have a higher sensitivity and specificity than sTfR alone. 28
sTfR is not a widely available assay. There is no uniform standard for measuring serum concentration or a universally established reference range. Therefore, while this may eventually be useful in determining iron status, validation is still necessary in population studies. 27
Zinc protoporphyrin
In the last step of haemoglobin production, ferrous protoporphyrin is combined with globin to make haemoglobin. When there is a lack of iron, zinc replaces iron to produce zinc protoporphyrin. The normal ratio of iron to zinc in protoporphyrin is approximately around 30,000:1, but zinc protoporphyrin (ZPP) will increase to measurable concentrations with progressive iron deficiency. 18 Currently, this assay is not widely available but could be considered when conventional iron studies are not diagnostic.
Anaemia of chronic disease
Anaemia of chronic disease (ACD) is the second most common cause of anaemia worldwide 1 ; it was first identified in 1962 after studies on anaemia associated with infection. 29 ACD is expected to become more prevalent in the future, as the number of elderly patients with chronic inflammatory conditions rises.
A variety of clinical conditions can lead to ACD such as infection, inflammatory disorders (including inflammatory bowel disease and rheumatological conditions) and malignancy; these three causes account for 75% of cases. 30 ACD is immune driven. Cytokines induced by activated leucocytes exert multiple effects that contribute to the fall in haemoglobin; these include changes in iron homeostasis, erythropoietic activity, erythropoietin production and the life span of erythrocytes. 1
A particular case of ACD is the anaemia of chronic renal failure. This is mediated by a decrease in circulating erythropoietin, which leads to a reduction in erythropoietic activity; this antiproliferative effect is enhanced by accumulating uraemic toxins. 31 In patients with end stage disease, chronic inflammation has also been shown to correlate with the degree of anaemia. 32 The activation of immune cells may stem from repeated infection and/or contact activation from dialysis membranes. In these patients, the changes of iron homeostasis mirror those found in ACD. 1
The diagnosis of ACD can be challenging and is perhaps best explained in conjunction with the pathophysiological mechanisms underlying this disease.
Dysregulation of iron homeostasis and its effect on laboratory markers
Disturbance of iron homeostasis is a hallmark of ACD and is driven by inflammatory cytokines.
There is an increase in interferon-γ (IFN-γ), tumour necrosis factor-α (TNF-α), interleukin-1 (IL-1), interleukin-6 (IL-6) and interleukin-10 (IL-10). 1 IL-6 and lipopolysaccharide (endotoxin found on the outer membrane of Gram-negative bacteria) are strong inducers of hepatic hepcidin production, 33 this results in reduced ferroportin-1 expression and sequestration of iron within the enterocytes, hepatocytes and macrophages. 9 Iron import is unregulated in the macrophages by increased DMT-1 expression (mediated by IFN-γ and lipopolysaccharide), upregulation of TfR expression (mediated by IL-10) and lastly phagocytosis of senescent erythrocytes, a process which is enhanced by TNF-α-mediated damage of erythrocyte membranes. 1 Lastly, TNF-α, IL-1, IL-6 and IL-10 all induce ferritin expression and stimulate the storage of iron. 6
The overall effect is increased iron storage, particularly in the macrophages, and decreased availability of iron which ultimately leads to iron restricted erythropoiesis. 34 This can be assessed by laboratory markers.
FBC and blood film
ACD varies in severity, but patients typically present with mild (Hb >100 g/L) or moderate (Hb 85–100 g/L) reductions in haemoglobin concentrations. 35 Microscopically, the erythrocytes are usually normocytic and normochromic. Concurrent haematinic deficiencies, haemoglobinopathies and the underlying disease can all affect the red cell indices and blood film features; therefore, the FBC alone is not sufficient in the diagnosis of ACD.
Iron studies
Serum iron is reduced in ACD, reflecting the decreased availability of iron. Serum transferrin is typically normal or low, and its fall in acute inflammation is thought to be due to increased degradation. 36 Depending on transferrin concentration, TIBC can be low or normal. Transferrin saturation is typically low and is a reflection of the decreased serum iron. Serum ferritin is either normal or elevated, in part due to ferritin's role as an acute phase protein but also the net effect of diversion of the body's iron into this storage protein within the RES in ACD. Table 1 summarizes these changes.
sTfR
As previously discussed, sTfR is not affected by inflammatory cytokines and therefore can be useful in differentiating between isolated ACD (in which the concentration would be normal) and ACD associated with true iron deficiency when sTfR would be elevated.
ZPP
In patients with impaired iron supply for erythropoeisis, regardless of the cause, ZPP concentrations will rise. Therefore, ZPP concentrations rise in ACD and cannot be used to assess whether there is superimposed iron deficiency. 37
Hepcidin
Hepcidin plays a central role in the dysregulation of iron homeostasis seen in ACD. Hepcidin is usually elevated in ACD; however, the increase in production may be opposed by the effects of iron deficiency. 38 Therefore, concentration may be useful in distinguishing patients with pure ACD from those with superimposed iron deficiency. However, the long-term effects of hepcidin may be to induce iron deficiency, and therefore, its use in diagnosing ACD needs to be more carefully evaluated and standardized. 39
Iron overload
Iron overload in the setting of anaemia is commonly iatrogenic (repeated red cell transfusion in patients with thalassaemia major, for example). However, it is also a well-documented phenomenon in certain diseases such as non-transfusion-dependent thalassaemias and sideroblastic anaemia.
In iron overload, the capacity for transferrin to transport iron is exceeded; this results in an increase in non-transferrin-bound iron within the plasma, leading to direct oxidative damage to tissues and organs. 40 Iron accumulation in the parenchyma can lead to significant organ damage including liver cirrhosis, diabetes and myocardial damage; early diagnosis and treatment are particularly important for patients in whom iron overload is the main factor in limiting survival.
While it is beyond the remit of this review to describe the pathogenesis of iron overload in these conditions, the effect of iron overload on iron studies will be discussed.
Diagnosing iron overload
Typically in iron overload, iron studies show elevated ferritin, serum iron and transferrin saturation; there is a decrease in both TIBC and transferrin. A raised transferrin saturation is often an early marker of iron overload; a saturation of >45% is highly suggestive of iron overload. 19 Table 1 summarizes these changes.
While there is evidence that serum ferritin concentration correlates with the degree of parenchymal loading in organs such as the liver, its accuracy can be compounded by factors such as inflammation and the underlying disease process. 41 Determination of liver iron concentration through biopsy is a reliable indicator of total body iron stores in patients with thalassaemia major; however, this procedure is invasive. 42 Non-invasive techniques such as MRI T2* have been shown to quantify iron in both the liver and myocardium; MRI can be useful in diagnosing iron overload and guiding response to treatment. 43
Summary
Iron is an essential element required for growth and survival. Deficiency and dysregulation of iron homeostasis form the basis of the two commonest causes of anaemia worldwide, iron deficiency anaemia and ACD. Iron studies can be useful in the differentiation between the two disease processes and be used to guide diagnosis and treatment.
Footnotes
Acknowledgements
This article was prepared at the invitation of the Clinical Sciences Reviews Committee of the Association for Clinical Biochemistry and Laboratory Medicine.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
Not applicable.
Guarantor
JU.
Contributorship
YYP drafted the manuscript; JU critically revised of the manuscript. YYP and JU approved the manuscript for submission/publication.