
Abstract
Gestational diabetes is a common pregnancy disorder which is generally managed with diet, exercise, metformin or insulin treatment and which usually resolves after delivery of the infant. Identifying and treating gestational diabetes improves maternal and fetal outcomes and allows for health promotion to reduce the mother’s risk of type 2 diabetes in later life. However, there remains considerable controversy about the optimal method of identification and diagnosis of women with gestational diabetes. The NICE-2015 diagnostic criteria (75 g oral glucose tolerance test (OGTT) 0 h ≥5.6 mmol/L; 2 h ≥7.8 mmol/L) are based upon cost-effectiveness estimates using observational data, while the WHO-2013 criteria (75 g OGTT 0 h ≥5.1 mmol/L; 1 h ≥10.0 mmol/L; 2 h ≥8.5 mmol/L) identify women and infants at risk of adverse outcomes according to prospective data. There is also considerable controversy about testing for gestational diabetes using universal or risk factor-based screening, and when and how testing should be performed. The aim of this review is to provide a summary of the clinical biochemistry aspects to these debates and to highlight the importance of appropriate identification of gestational diabetes and subsequent type 2 diabetes in this population.
Keywords
Introduction
Gestational diabetes (GDM), defined as hyperglycaemia with onset or first recognition in pregnancy,1,2 is becoming increasingly common in many populations worldwide. 3 In the United Kingdom, around 700,000 women give birth every year and 5% are thought to be affected by GDM. 4 Untreated, GDM is associated with adverse maternal and neonatal outcomes, including macrosomia (high birth weight, usually above a threshold of 4 or 4.5 kg), shoulder dystocia and pre-eclampsia, which can be prevented or ameliorated with appropriate intrapartum treatment to reduce blood glucose concentrations to euglycaemic concentrations. 2
The diagnosis and screening of GDM, areas of particular relevance to clinical biochemistry departments, have been fraught with controversy for many years. Indeed, a survey undertaken by NHS Diabetes several years ago found that among hospital departments who responded to the survey request, there were 13 different diagnostic criteria in use for GDM in the United Kingdom. 5 This degree of variety is likely to diminish following the publication of guidelines from the National Institute for Health and Care Excellence (NICE) in February 2015. 4 The aim of the current review is to summarize the changes recommended in the new guideline and to discuss their likely implications upon the screening and diagnosis of GDM.
Defining GDM as a disease entity
GDM, as defined as hyperglycaemia with onset or first recognition in pregnancy,1,2 is a heterogeneous condition. Early reports of GDM focused on a condition which resolved after delivery of the fetus 6 but which was associated with the development of permanent diabetes in later life. 7 This implies that hyperglycaemia in pregnancy occurs due to an acute worsening of glycaemic control during pregnancy in the context of chronically abnormal and gradually deteriorating glucose homeostasis. However, in practice, as GDM is defined based on glucose concentrations rather than pathology, a number of different pathological processes could contribute, such as pre-existing insulin resistance, pre-existing insulin insufficiency and pregnancy hormone-induced short-term disturbances in insulin release or function. These subtle pathological differences are poorly understood but may account for differences in maternal phenotypes, perinatal outcomes and long-term diabetes risk.
Normal pregnancy is associated with short-term variations in the body’s control of glucose homeostasis. During the first and early second trimester, blood glucose concentrations may be normal or low, but after around 20–28 weeks, insulin resistance is typical. 8 The development of insulin resistance is likely to be multifactorial in aetiology and may be caused by increasing concentrations of human placental lactogen, human placental growth hormone and tumour necrosis factor-alpha or falling concentrations of adiponectin. 9 In all pregnant women, insulin requirements increase by an estimated 200–250% during this period and healthy pregnant women maintain euglycaemia by increasing insulin production. 8 Although many women with GDM mount a substantial insulin response, this compensatory increase is unable to effectively reduce fasting or postprandial glucose to euglycaemic concentrations. 8
Diagnostic criteria for GDM
Although diabetes in pregnancy which resolves in the postpartum period was first described in the 19th century, 6 the association of pregnancy diabetes with adverse outcomes was only determined around the middle of the 20th century. Jackson, 7 based in Cape Town, South Africa, observed that women who eventually developed diabetes in later life often had a history of giving birth to macrosomic or stillborn infants. Interestingly, Jackson found that women who developed overt diabetes within five years after pregnancy were at highest risk of having a stillborn or macrosomic infant. He went on to establish a reference range for a 50 g glucose challenge at 36 weeks’ gestation and identified that glycosuria was not a good predictor of outcomes, partly due to an altered renal threshold for glucose excretion. 7 Jackson’s work identifying and quantifying the risks of hyperglycaemia in pregnancy was reproduced by others in different populations and GDM began to be recognized as a disease with short- and long-term repercussions.10–12 However, the best method of diagnosing and treating the disease remained unclear.
During the same time period, the oral glucose tolerance test (OGTT) had been widely used in non-pregnant patients, and evidence was available to show that OGTT results were different in unselected pregnant women. 13 O’Sullivan and Mahan found that pregnant women had low fasting and high postprandial glucose concentrations compared with non-pregnant women exposed to a 100 g OGTT. They went on to study responses to a 100 g 3 h OGTT and identified cut-off values for GDM based upon concentrations two standard deviations (SD) above the mean for each of the fasting, 1, 2, and 3 h post load glucose values. They suggested that two abnormalities should be required to make a diagnosis. This first set of diagnostic criteria aimed to identify women at risk of subsequent type 2 diabetes (T2DM) and affected women had a 22.6% risk of developing the disease in the following eight years. 14 Using these criteria, GDM was diagnosed in around 2% of pregnancies.
Current and recent criteria used for diagnosis of GDM based on the oral glucose tolerance test (OGTT).
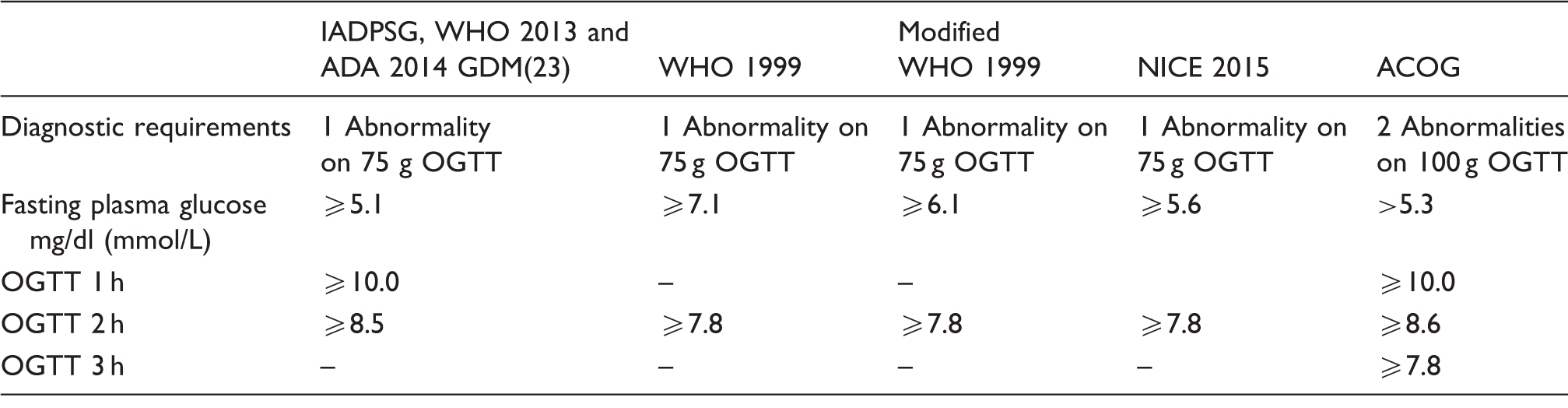
ACOG: American College of Obstetricians and Gynaecologists; IADPSG: international association of the diabetes in pregnancy study groups; NICE: national institute for health and clinical excellence; WHO: world health organization.
Recommendations for screening for GDM in pregnant women.

ACOG: American College of Obstetricians and Gynaecologists; ADA: American Diabetes Association; GDM: gestational diabetes; IADPSG: international association of the diabetes in pregnancy study groups; NICE: national institute for health and clinical excellence; OGTT: oral glucose tolerance test; POCT: point of care testing; T2DM: type 2 diabetes; WHO: world health organization.
An international impasse
The lack of international consensus about diagnostic criteria for GDM creates great challenges for improving global management of the condition. Many attempts have been made at developing a consensus. The ACOG committee considered adopting the IADPSG criteria but concluded that there was insufficient evidence that the extra cohort of women identified by the IADPSG criteria were genuinely at risk of adverse pregnancy outcomes or that treatment could improve outcomes. 20 Other commentators have suggested that requiring only one abnormality confers poor diagnostic precision, presumably by increasing the false-positive rate. 26 However, no data are available to quantify this alleged imprecision or to compare it with the imprecision of a two-abnormality approach. Several studies have assessed pregnancy outcomes in women with IADPSG-positive GDM in comparison to GDM diagnosed with other criteria and found that the extra cases of GDM identified with the IADPSG guidelines appear to be at verifiable increased risk of pregnancy complications.27–30 Very few studies have addressed the cost-effectiveness of implementing the IADPSG criteria, but there is some evidence to suggest that adoption of these criteria can be cost-effective 31 due to the opportunity to reduce adverse pregnancy outcomes.
A NICE solution?
Summary of 2015 NICE guidelines for GDM diagnosis and screening.
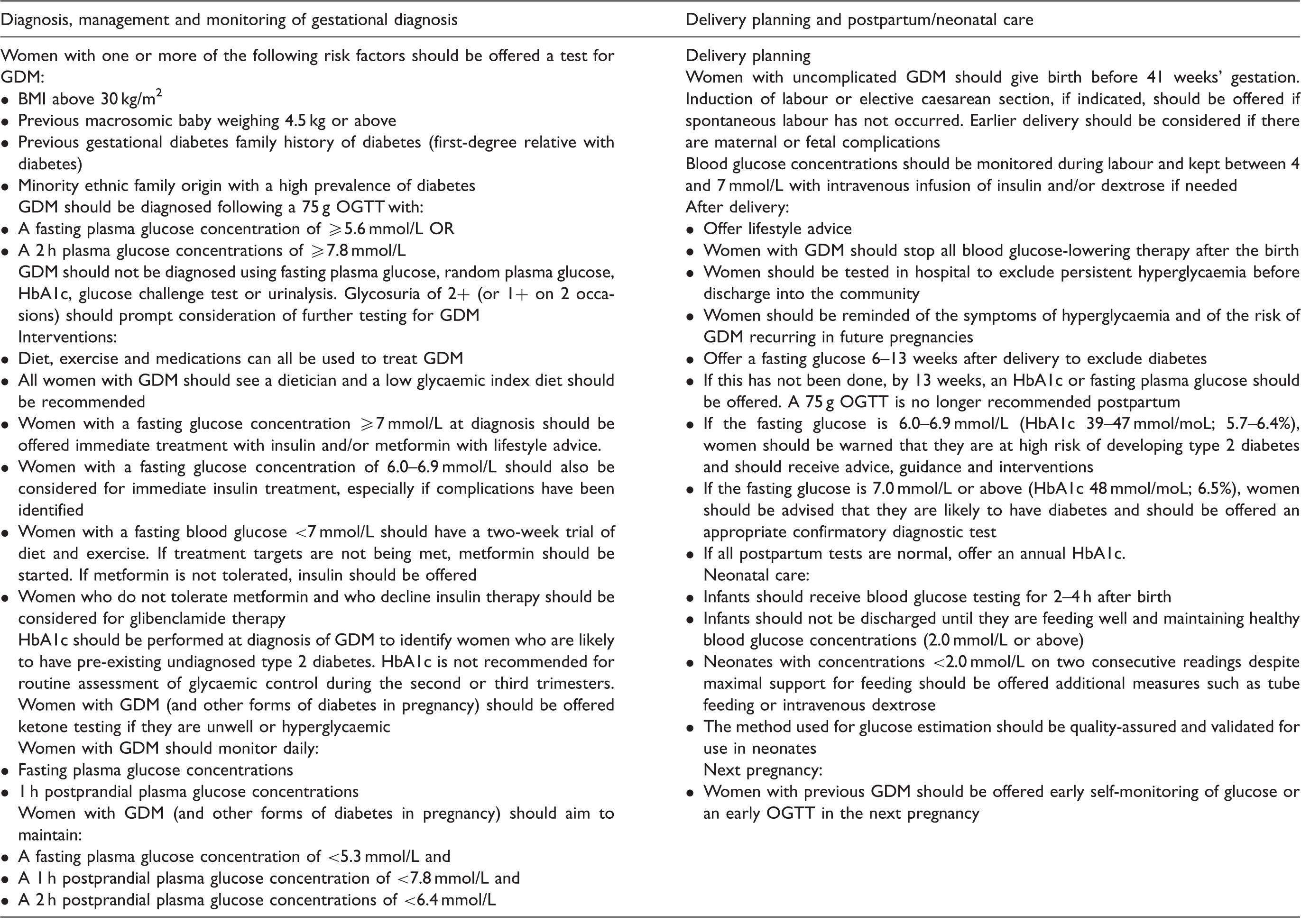
BMI: body mass index; GDM: gestational diabetes; NICE: national institute for health and clinical excellence; OGTT: oral glucose tolerance test.
The 2015 NICE thresholds have added to the controversy surrounding GDM diagnosis by failing to adopt criteria consistent with those of the WHO, 2 which are based upon prospective evidence from the HAPO study. 22 Furthermore, although the threshold of 5.6 mmol/L is expected to improve outcomes compared with the previous threshold of 7.0 mmol/L, the NICE-2015 criteria have never been tested in clinical practice and were instead derived theoretically from available data on clinical outcomes and cost-effectiveness. 4 The data used came from prospective and retrospective studies and some unpublished data taken from centres across the UK. Unfortunately, there were relatively few studies reporting cost-effectiveness of different approaches to diagnosis and screening of GDM. Many studies had methodological flaws and this limited the quality of evidence available for the NICE analysis. Furthermore, outcomes such as macrosomia and large-for-gestational age were difficult to attach a cost to and were therefore not included in the analysis. Long-term risks were also not included in the analysis. Women with GDM are at risk of diabetes in later life and their offspring are at risk of diabetes in adulthood. 32 Diagnosis of GDM allows health promotion and gives women access to diet and lifestyle advice which may benefit both the patient and their family. However, there is currently very little evidence to suggest that diagnosing GDM has beneficial effects on obesity or diet in later life, or that earlier diagnosis of T2DM through enhanced surveillance reduces complication rates and health-care costs.
Screening for GDM
The issue of how best to identify women who have GDM is also complex and controversial. The WHO recommends universal screening of all pregnant women with the 75 g OGTT. However, this approach has important resource implications and has been considered unfeasible by many, especially in resource-poor areas of the world. NICE recommends (in both 2008 and 2015 guidelines) the use of a selective screening approach, where screening is only offered to women based upon risk factors including previous GDM, previous macrosomic infant, a family history of diabetes in a first-degree relative, ethnic origin with a high diabetes prevalence or to women with obesity.4,33 Women with one or more risk factors should be offered a 75 g OGTT at 24–28 weeks’ gestation. However, while risk factor-based screening approaches are both practical and economical, they will tend to miss women who develop GDM in the absence of traditional risk factors, who may account for up to 20% of cases depending upon the population.34–36 Concerningly, the selective screening approach also appears to perform particularly poorly in some ethnic groups.37–39 There is also some evidence that health-care professionals do not always take a thorough history of relevant risk factors from pregnant women at booking leading to inconsistencies to this approach. 40
Biochemical testing offers some advantages over a risk factor-based approach. A wide range of glucose-related tests have been used for the screening of GDM in the past. Various approaches have included urinalysis for glucose, fasting blood glucose, random blood glucose, the 1 h 50 g glucose challenge test (GCT) and both 75 g and 100 g OGTTs. Current guidelines2,4 now recommend testing women using a one-step approach with a 75 g OGTT. However, a two-step approach is still used in the United States and elsewhere, based upon a 50 g GCT with a 1 h post load glucose measurement. Women who have an elevated GCT result (usually ≥7.8 mmol/L) are then offered an OGTT. However, screening with the GCT may miss women with fasting hyperglycaemia who are now known to be at increased risk of pregnancy complications, even if the postprandial glucose concentrations are within acceptable limits.22,30 Other screening approaches using random glucose or fasting glucose have also had limitations in clinical practice due to poor sensitivity or specificity.41–43 We recently assessed the validity of a random blood glucose taken at antenatal booking which was found to be more predictive of the development of GDM later in pregnancy compared with the presence of maternal obesity. 44
Screening for overt diabetes in the antenatal population
Many healthy young women have little contact with health services until they become pregnant. This creates particular challenges in identifying women with pre-existing undiagnosed diabetes (‘overt diabetes’) who are at a much higher risk of complications compared with women with GDM. Women with overt diabetes have hyperglycaemia prior to conception and during the first trimester, which creates an increased risk of fetal anomalies and miscarriage. Screening for overt diabetes is therefore vital and should occur early in gestation. The 2015 NICE guidelines make no recommendations for the identification of women with overt diabetes but conclude that better evidence is required to assess the prevalence of undiagnosed T2DM in the antenatal population and to assess different strategies to identify these women. 4 We have previously shown that a random blood glucose at antenatal booking can be used to screen for overt diabetes, 45 a test which is convenient, economical and widely available.
Screening for persistent diabetes in the postnatal population
A further opportunity to identify women with diabetes exists after pregnancy as some women with GDM will not return to normal glucose homeostasis after the birth. Overall, the lifetime risk of T2DM after GDM is high (50–70%),46,47 and the rates of identification of T2DM within the first year are significant. The reasons for this early progression to T2DM are unclear. Theoretically, these women may have declining pancreatic function prior to pregnancy or pregnancy itself may have accelerated existing pancreatic insufficiency. The possibility of monogenic forms of diabetes (such as maturity onset diabetes of the young (MODY)) or pregnancy-induced hypertriglyceridaemic pancreatitis (clinical or subclinical) should also be considered. Early progression to T2DM is associated with increased maternal age, obesity, excessive weight gain during pregnancy, early diagnosis of GDM, insulin requiring GDM and high glucose results on the antenatal OGTT.
Identifying diabetes in the postpartum period is challenging. Glucose homeostasis takes time to stabilize after birth, and the altered red cell turnover and possibility of recent intrapartum haemorrhage makes HbA1c measurement unreliable initially. The 2015 NICE guidelines recommend postpartum testing after six weeks using fasting plasma glucose (FPG) or an HbA1c after 13 weeks. 4 The OGTT is no longer recommended. Women with postpartum prediabetes (fasting glucose 6.0–6.9 mmol/L and/or HbA1c 39–47 mmol/moL) should be offered lifestyle advice and told that they are at high risk of diabetes. Women with a result consistent with diabetes (fasting glucose ≥7.0 mmol/L or HbA1c ≥48 mmol/moL) should be offered an appropriate confirmatory test. If all postpartum tests are normal, an annual HbA1c should be offered. 4 Importantly, breast feeding can reduce the incidence of diabetes by around 50% within the first two years postpartum. 48 However, lactation can also give misleadingly low results on glucose screening, and women with borderline results should be particularly encouraged to attend for ongoing screening.
The differential diagnosis of GDM
Diabetes which is first diagnosed in pregnancy is often assumed to be GDM but can also be:
Pregestational undiagnosed or developing type 1 diabetes (T1DM). Pre-existing undiagnosed T2DM. MODY diabetes. Pancreatic destruction (Type 3 c diabetes), for example, due to hypertriglyceridaemia.
The patient’s first visit to the diabetes in pregnancy clinic is the main opportunity to assess the underlying diagnosis. Clinicians should have a low threshold for considering pregestational diabetes as the risks are higher for mother and child and treatment with insulin would normally be required from the outset. Patients with pregestational diabetes may have a high HbA1c (≥48 mmol/moL) at diagnosis, OGTT results within the thresholds for overt diabetes or evidence of a large-for-gestational-age fetus on ultrasonography at 20 weeks, particularly with a large fetal abdominal circumference. Undiagnosed T1DM might be associated with progressively worsening blood glucose control, ketosis and the presence of autoantibodies such as anti-islet and anti-glutamic acid decarboxylase (GAD) antibodies. Ketosis can also occur in T2DM or GDM in association with reduced carbohydrate intake. Pancreatic destruction (Type 3 c diabetes) may present in a similar way to T1DM but without autoantibody involvement. Triglycerides should be measured in hyperglycaemic women with abdominal pain, new skin lesions or a history of prepregnancy hypertriglyceridaemia.
Recent evidence has shown that MODY diabetes (due to genetic mutations in glucose sensing or in transcription factors which regulate insulin production or secretion from the pancreatic beta cells) may affect one in six women who fulfil the criteria for GDM. 49 Mutations in glucokinase (MODY2) which cause lifelong mild fasting hyperglycaemia are particularly likely to present during pregnancy but are not usually associated with complications in later life. 50 Unfortunately, although patients with glucokinase mutations may have a high fasting glucose with a low OGTT glucose increment, there is currently no consensus for screening for MODY in pregnancy. 49 Women with MODY2 mutations may require more aggressive treatment during pregnancy than patients with GDM but rarely require treatment in later life as the risk of complications such as retinopathy is low. Although MODY screening is costly, the risk of misdiagnosis is also costly, resulting in decades of unnecessary treatments for presumed T2DM. 50
Conclusions
GDM is a common pregnancy disorder which is generally managed with diet, exercise, metformin or insulin treatment and which usually resolves after delivery of the infant. Identifying and treating GDM improves maternal and fetal outcomes, and allows for health promotion to reduce the risk of diabetes in later life. However, there remains considerable controversy about the optimal method of identification and diagnosis of women with GDM. The NICE-2015 criteria are based upon cost-effectiveness, while the WHO-2013 recommendations are based upon identification of pregnancies at risk of peripartum complications. The Carpenter–Coustan criteria were devised to identify women at risk of diabetes in later life. These issues of cost-effectiveness and short- and long-term risks are all important, and an ideal set of diagnostic criteria would encompass all three aspects. Despite these discrepancies, it is imperative that older diagnostic thresholds are updated (fasting glucose >6–7 mmol/L is too high) to reflect the recent changes in guidelines and evidence.
A further issue is the nature and performance of screening or diagnostic testing for GDM. Pregnancy offers unique challenges for diagnostic testing as test performance may depend upon the gestational stage and red cell turnover. Current guidelines (NICE and WHO) have moved away from the GCT and towards the 75 g OGTT, performed in most women at 24–28 weeks’ gestation. However, the possibility of early hyperglycaemia due to undiagnosed overt diabetes, MODY diabetes or early onset GDM should also be considered.
Footnotes
Acknowledgements
This article was prepared at the invitation of the Clinical Sciences Reviews Committee of the Association for Clinical Biochemistry and Laboratory Medicine.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
Not applicable.
Guarantor
CLM.
Contributorship
CLM wrote the manuscript.