
Abstract
Objective
To establish whether maternal serum first trimester concentrations of PAPP-A and free hCGβ are altered in pregnancies that subsequently are diagnosed by an oral glucose tolerance test (OGTT) with gestational diabetes mellitus (GDM).
Methods
Over the period 2009 and 2011, the results for women who had first trimester screening for aneuploidy were matched with those having an oral glucose tolerance test at 22–26 weeks for suspected GDM. Free hCGβ, PAPP-A and NT MoMs were compared amongst the group having an OGTT with confirmed GDM and those in which GDM was not confirmed. A second comparison group consisted of all non-aneuploidy singleton pregnancies in which no OGTT was performed.
Results
During the three-year period, 27,660 singleton pregnancies were screened of which 7429 cases had an OGTT of which 870 cases were classed as GDM by WHO criteria. There was a significant 7–9% reduction in both PAPP-A and free hCGβ MoM in the GDM group compared with either the OGTT non-GDM group or the remaining pregnancies with no known risk factors for evidence of GDM. There was no difference in the NT measurements.
Conclusions
First trimester concentrations of PAPP-A and free hCGβ are reduced in pregnancies that subsequently are diagnosed with GDM and may be useful in further screening algorithms for this disorder although the sensitivity alone is quite poor.
Introduction
The first trimester combined test screens for trisomy 21 and other aneuploidy by measuring maternal serum pregnancy associated plasma protein A (PAPP-A), free-β human chorionic gonadotropin (free hCGβ) and ultrasound foetal nuchal translucency. The marker results are then combined in a screening algorithm to produce a likelihood ratio which is multiplied by the a priori maternal age-related risk, resulting in an individual pregnancy specific risk.1,2 This test has been demonstrated to realize detection rates of 90% and above with false positive rates of 5%.3–5
The biochemical variables PAPP-A and free hCGβ are known to be influenced by a number of maternal or pregnancy variables such as gestational age, maternal weight, ethnicity and smoking status and correction for these variables is taken into account when calculating the multiple of the median (MoM) prior to use in the risk algorithm. 6 We have previously shown in three studies that pre-existing insulin-dependent diabetes mellitus (Type 1 diabetes) in pregnant patients may result in a reduction of these markers.7–9 The impact on PAPP-A has been confirmed in two other studies10,11 but refuted in one study 12 which found an insignificant decrease in a smaller number of cases of Type 1, but found a significant reduction in a similar number of cases of Type 2 diabetes.
Gestational diabetes mellitus (GDM) has been shown to be associated with increased risk of adverse pregnancy outcome in the Hyperglycemia and Adverse Pregnancy Outcome (HAPO) study. 13 Low concentrations of PAPP-A have also associated with poor obstetric outcomes such as low birth weight, pre-term delivery, spontaneous foetal loss, small for gestational age and pre-eclampsia.7,14–17 Few studies have looked at biochemical screening markers in instances of confirmed GDM. One study, of a small number of cases, 7 showed a significant reduction in both concentrations of PAPP-A and free hCGβ, whilst other studies12,18 found either no significant effect or found a significant reduction only for PAPP-A. 19
The current study aims to investigate whether the presence of confirmed GDM has any impact on the first trimester aneuploidy screening markers foetal nuchal translucency (NT), maternal serum free hCGβ or PAPP-A.
Materials and methods
Study population
In Barking Havering and Redbridge University Hospitals NHS Trust (BHRUT), all pregnant women are offered first trimester (11 weeks+0 days to 13 weeks+6 days) screening for trisomy 21 and trisomy 13/18 by the combined test.3,5 Free hCGβ and PAPP-A are measured by a KRYPTOR Analyzer (Brahms AG, Hennigsdorf, Germany) – a random access immunoassay analyser, using time-resolved amplified cryptate emission (TRACE) technology, which provides an accurate and highly reproducible result within 20 min. Foetal NT and crown-rump-length are measured by standardized techniques by sonographers who had completed the certificate of competence in the first trimester scan issued by the Fetal Medicine Foundation (FMF). Demographic characteristics, ultrasound findings and the results of biochemical testing are entered into a computer database (ViewPoint) at the time of assessment. Data on pregnancy outcome, subsequently obtained from the maternity unit, are also entered into the database. A search was made of the database to identify women with normal singleton pregnancies who had had first trimester combined screening within BHRUT during the period of investigation from 1 October 2008 to 30 September 2011. Exclusion criteria were women with pre-existing diabetes, a foetal birth weight of equal to or less than the 5th centile for gestational age at delivery and pregnancies with foetal death at any time after initial first trimester screening.
Women were considered to be at risk for GDM 20 based upon the following clinical criteria: a body mass index above 30 kg/m2; a previous macrosomic baby weighing 4.5 kg or above; previous gestational diabetes; family history of diabetes (first-degree relative with diabetes); family origin with a high prevalence of diabetes, i.e. South Asian, black Caribbean or Middle Eastern. Those at risk were offered an oral glucose tolerance test (OGTT) between 22 and 26 weeks of gestation. A diagnosis of GDM was made based on WHO criteria, in which the plasma glucose concentration at 2 h after the oral administration of a 75 g glucose load was 7.8 mmol/L or greater. 21 Plasma glucose was measured in the routine clinical biochemistry laboratory on an Olympus 2700 utilizing a liquid-based hexokinase method. Patient records from routine clinical biochemistry examinations were stored in the routine pathology computer database (WinPath). A search was made of the database to identify results of OGTT tests performed on women registered to the various antenatal clinics within BHRUT during the period of investigation from 1 January 2009 to 31 December 2011.
Records from the ViewPoint database and the WinPath database were merged using a locally developed record linkage algorithm which utilized matching on patient data of birth, first name, surname, hospital number, sample date of the first trimester screening test and sample date of the OGTT. Institutional review board approval was given for use of these datasets.
Statistical analysis
Crown-rump length (CRL) was used to provide an accurate gestational age in all pregnancies and was compared between groups using the Mann-Whitney U-test. PAPP-A and free hCGβ concentrations were converted to MoMs, which standardize the markers for gestational age, maternal weight, smoking status, ethnic origin, parity and assisted conception using methods outlined previously. 6 NT was assessed as NT MoM using a previously established median equation. Analysis of PAPP-A, free hCGβ MoMs and NT MoM was carried out in the log10 domain, where their distributions are Gaussian, but reported in the original scale. Statistical comparison of marker levels between groups were performed using Student's unpaired two-sample t-tests. Receiver operator curve (ROC) analysis was performed to assess and potential value of individual markers in predicting GDM. Study group characteristics were compared using the Mann-Whitney U-test for continuous data and the Chi-squared test for categorical data. ROC analysis was performed in Analyse-it, all other analyses were carried out in R.
Results
Study population
During the three-year study period BHRUT recorded 30,128 births. During the same period the clinical biochemistry laboratory performed 11,885 pregnancy OGTT of which 1649 were classified as GDM or at risk for GDM using the WHO criteria. From the ViewPoint database we identified 27,485 complete first trimester screening records of singleton normal outcome pregnancies. Using record linkage we generated 7429 records in which there was both a first trimester screening record and results from the OGTT. Of the 4456 OGTT results unmatched to screening records, 2236 were unable to be matched on date of birth, hospital number and name, 1782 had no first trimester screening either due to having second trimester screening, booking too late for screening or declined screening and 438 were repeat OGTT in which case only the first was used. In 20,056 of those with first trimester screening, there was either no match or the OGTT was not performed. Of the linked records there were 870 cases with GDM and 6559 records with no evidence of GDM. These two groups became the primary comparison group. The unmatched records from the first trimester screening database became a secondary comparison group. The study population is summarized in Figure 1. Table 1 shows the maternal characteristics of the populations with GDM, the population with negative OGTT, and those which were normal pregnancies without a diagnosis of GDM or an OGTT (secondary comparison group).
Summary of the study population. Study group characteristics. Significance tests compare GDM group or OGTT non-GDM group with the no-OGTT non-GDM group. Significance *P < 0.05 **P < 0.001 (two-sample t-test, Mann-Whitney U-test or Chi-squared test).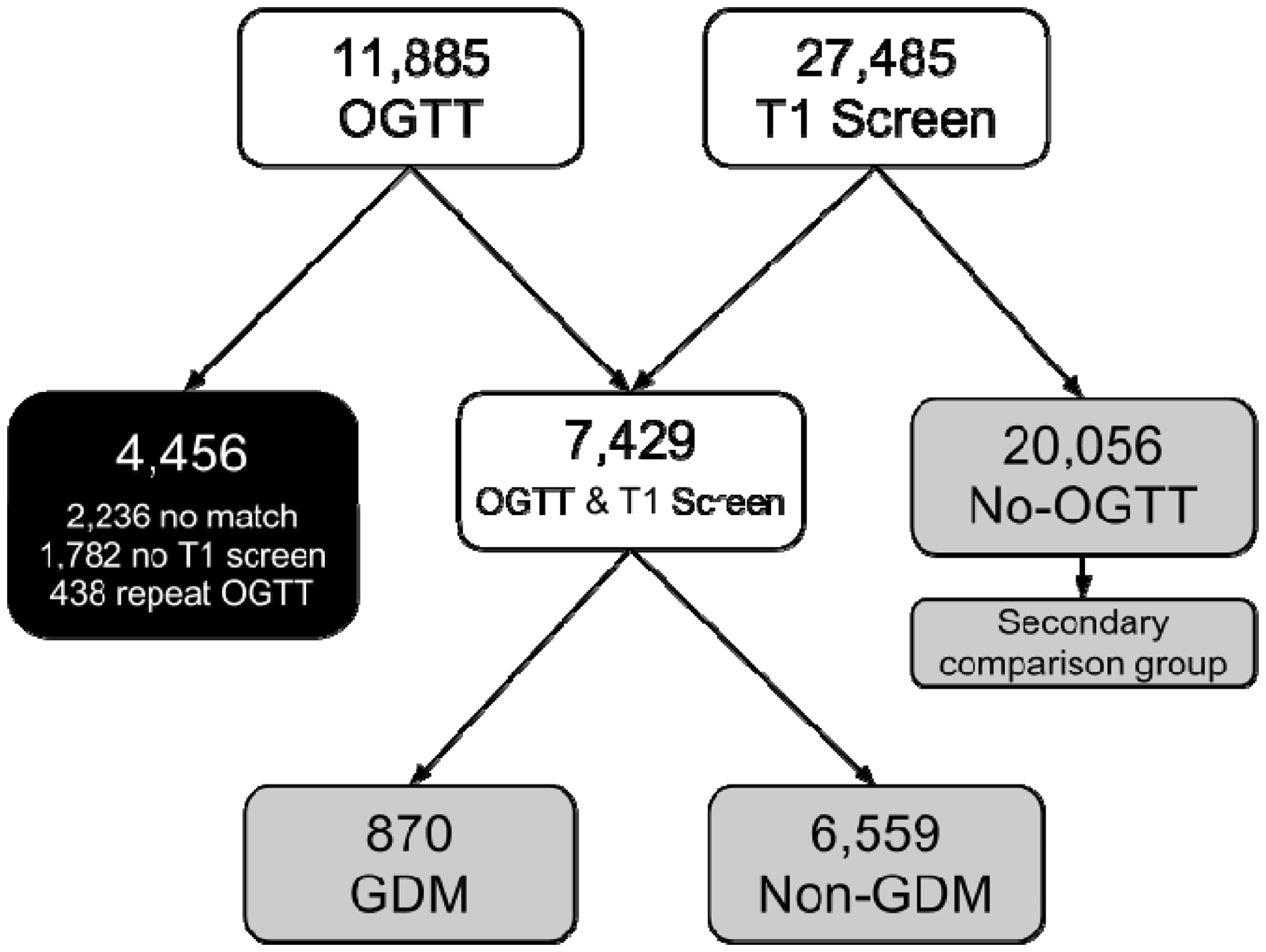
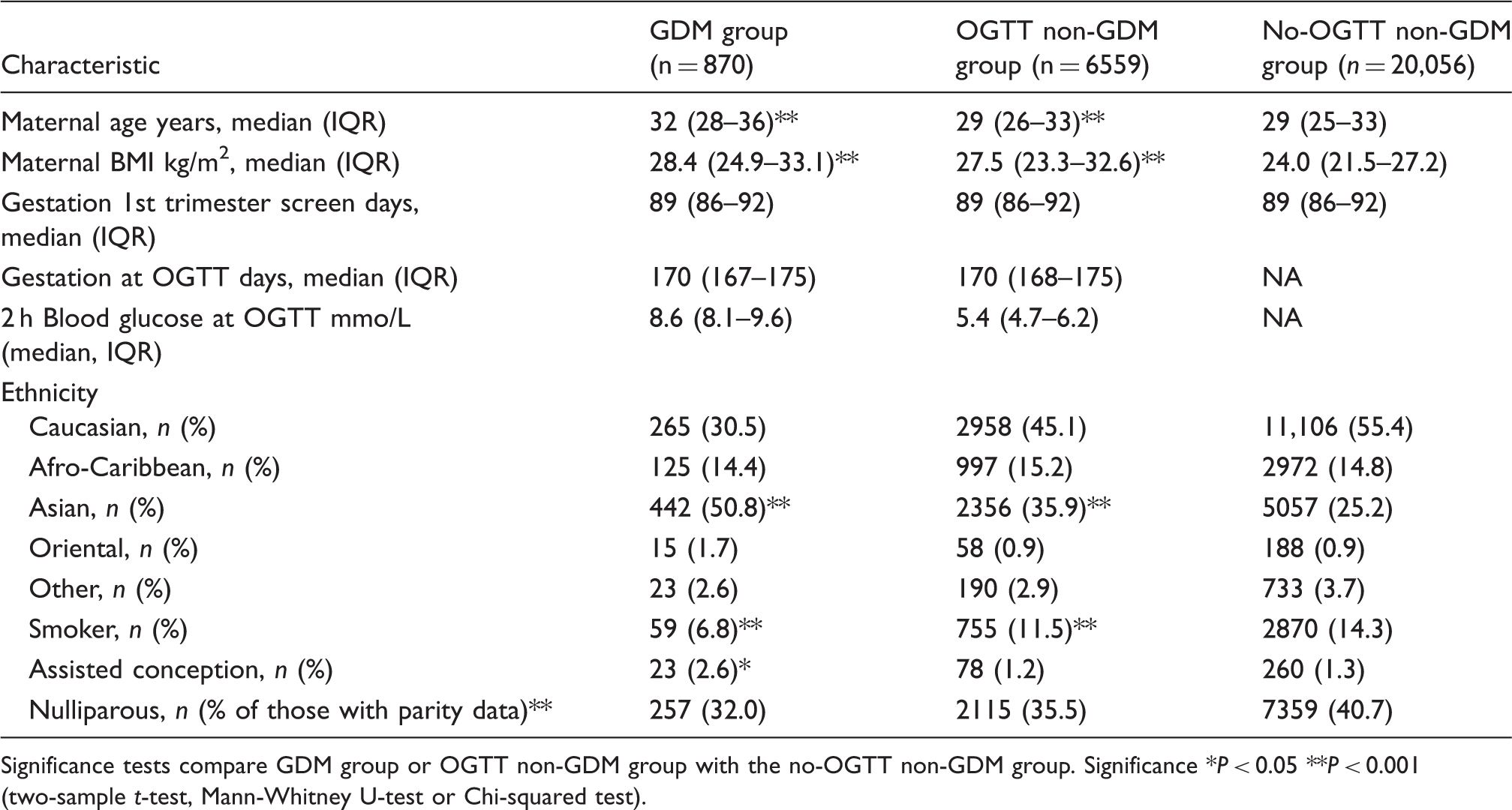
Compared with the secondary comparison group, the group diagnosed with GDM had a significantly higher median age which was not reflected in the group having OGTT but not diagnosed with GDM; however, this group did have a narrower distribution which made the test significant. There were also differences for BMI, as would be expected in that the group selected for OGTT would have been preselected because of increased BMI. Similarly, both OGTT groups had higher proportion of Asians amongst those diagnosed with GDM; this was an even higher proportion – again reflecting the preselecting criteria for OGTT. There was also a significantly higher proportion of women with assisted conception in those diagnosed with GDM, possibly related to the increased median maternal age in the assisted conception group (35 years versus 30 years; P < 0.0001).
Of the group with GDM, 12% were treated with insulin and 88% were treated with life style advice.
Screening markers
There was no significant difference in CRL between those with GDM confirmed by OGTT (median CRL 64.5 mm (IQR 58.8–70.0 mm)) and those without GDM confirmed by OGTT (64.8 mm (59.4–70.3 mm)) or the secondary comparison group (64.6 mm (58.9–70.4 mm)). Figure 2 shows that there was a significant reduction in mean marker log10 MoM for PAPP-A (MoM 0.91, P < 0.0001) and free hCGβ (MoM 0.93, P < 0.001) in the GDM confirmed by OGTT group compared with those without GDM confirmed by OGTT or the secondary comparison group (all MoM of 1.00). There was no evidence of different NT MoM between the three groups. ROC analysis showed that both serum markers were weak but significant (P < 0.001) predictors of GDM with an area under the curve of 0.54 (95% confidence interval: 0.52–0.56) for free hCGβ MoM and 0.55 (95% confidence interval: 0.53–0.57) for PAPP-A MoM.
Comparison of median marker MoMs in the group with GDM (grey circles), OGTT non-GDM (open triangles) and no-OGTT non-GDM group (filled squares). 95% confidence intervals are shown.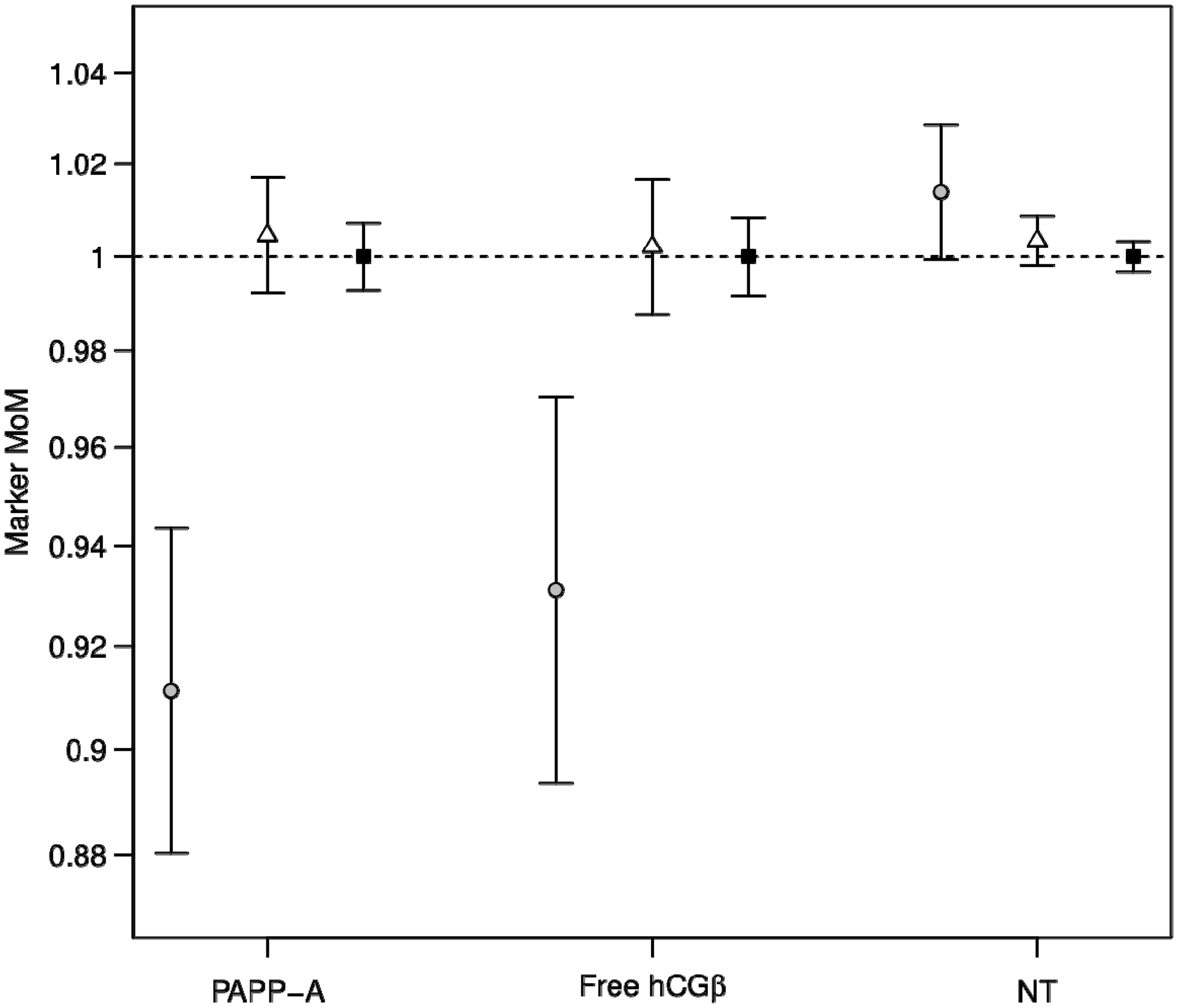
Although we have no data available for the 1 h glucose concentration, we tried to evaluate whether classification based on new diagnostic criteria from the HAPO study 13 of a fasting glucose concentration (⩾5.1 mmol/L) or the 2 h concentration (≥8.5 mmol/L) would have made any difference to the outcome. Using these two criteria would have identified 1006 women rather than 870 as GDM. Analysis of the MoM PAPP-A showed once more a significant reduction with a mean of 0.90 for GDM compared with 1.00 for controls (P < 0.0001) and a similar reduction for free hCGβ of 0.94 for GDM compared with 1.00 for controls (P < 0.001).
When we compared basal glucose concentrations in the GDM group and the non-GDM group in the log transformed domain there was no correlation between glucose and free hCGβ MoM, but there was a significant correlation between glucose and PAPP-A MoM thus:
For the GDM group this showed a correlation (Pearson's r) of −0.117 P < 0.001 and for the non-GDM group this showed a correlation of −0.0737, P < 0.0001. Comparing the 2 h glucose concentrations showed a similar negative correlation that was also significant in both groups. For the GDM group this showed a correlation of −0.0684 P < 0.05 and for the non-GDM group this showed a correlation of −0.0363, P < 0.01.
Discussion
Summary of published data on first trimester biochemical marker concentrations in pregnancies that subsequently were diagnosed as GDM.
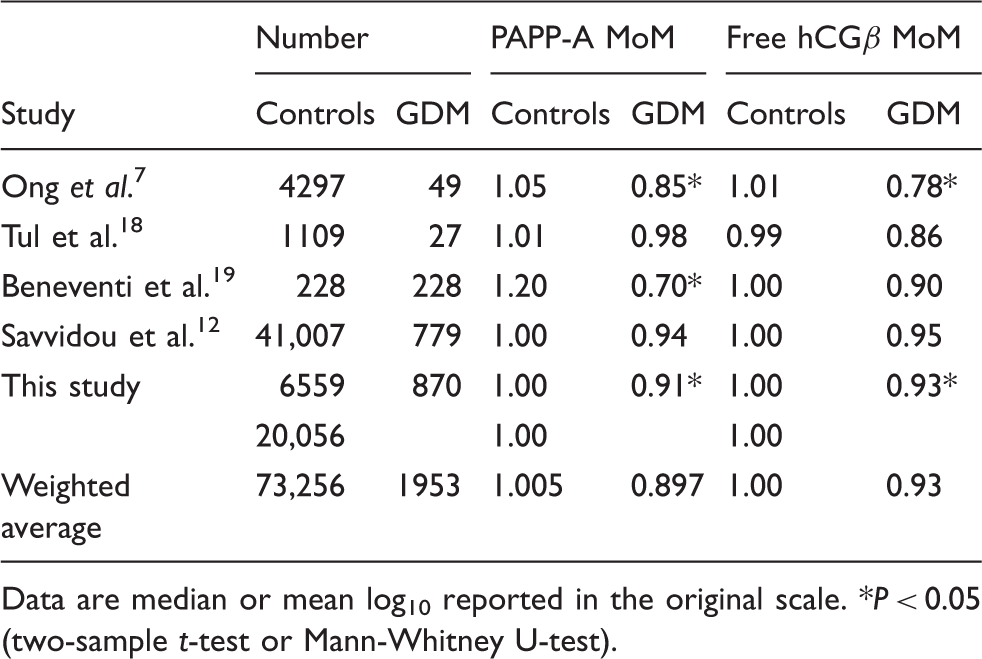
Data are median or mean log10 reported in the original scale. *P < 0.05 (two-sample t-test or Mann-Whitney U-test).
Of the studies in Table 2, the study by Savvidou 12 is of comparable power in terms of cases affected by GDM – although the selection of cases diagnosed as GDM was different in that all women were initially selected for OGTT based on a random glucose sample taken at 24–28 weeks and if 6.7 mmol/L or greater, then an OGTT was performed. There was no indication that the glucose sample was a fasting sample and women did not appear to be selected for OGTT based on predisposing risk factors which are the selection criteria recommended by NICE. 20 The results from both show that PAPP-A concentrations are reduced in GDM – although not significantly in the Savvidou study, 12 perhaps due to differing selection criteria. Our results also show a significant inverse correlation of PAPP-A MoM with both fasting glucose and 2 h post-OGTT glucose concentrations further indicating the importance and significance of glycaemic control around 22–26 weeks in relation to first trimester PAPP-A concentrations. Whilst a single glucose concentration in the context of an OGTT does not reflect glycaemic control per se, it may nevertheless suggest poor control. Age may also be relevant in GDM; further clarification of the association between age in the GDM cohort and aneuploidy markers would be warranted. An increased incidence of Down's syndrome may be associated with impaired glucose tolerance; however, more data are required to investigate whether there are more cases of Down's in the cohorts with GDM. Limitations of the study should be stated.
As a result of the HAPO study, there is considerable debate23–26 with respect to the definition of GDM, and recent proposals from the American Diabetes Association and the International Association of Diabetes and Pregnancy Study Groups have suggested 27 that the criteria be based on the 75 g OGTT but that GDM is defined by either a fasting glucose equal to or greater than 5.1 mmol/L or the 1 h glucose equal to or greater than 10.0 mmol/L or the 2 h glucose equal to or greater than 8.5 mmol/L. Although we have no data available for the 1 h glucose concentration we tried to evaluate whether classification based on the fasting glucose concentration or the 2 h concentration as indicated above would have made any difference to the outcome. Analysis of the PAPP-A MoM showed once more a significant reduction with a mean of 0.90 for GDM compared with 1.00 for controls (P < 0.0001) and a similar reduction for free hCGβ MoM of 0.94 for GDM compared with 1.00 for controls (P < 0.001). Thus, classification of GDM by either criterion still results in reduced concentrations of both maternal serum biochemical markers.
The HAPO study 13 found an association between hyperglycaemia and birth weight above the 90th centile and also between premature delivery, shoulder dystocia or birth injury, hyperbilirubinemia, pre-eclampsia and the need for intensive neonatal care. Clearly, maternal hyperglycaemia is associated with significant adverse pregnancy outcome. Other studies have shown that there is benefit in treating gestational diabetes.28–30 In addition, impaired glucose tolerance may be a risk factor for pregnancies with Down’s syndrome.31,32
There is currently no accepted method of screening for GDM. The UK NICE Guidelines 20 recommend that women with certain maternal clinical characteristics are offered an OGTT between 22 and 28 weeks in order to diagnose GDM. However, using such individual criteria results in a poor detection rate (60%) with a high false positive rate (35%). 33 More recently, two groups have developed predictive models for GDM based on patient characteristics and medical history. Van Leeuwen et al. 34 reported a risk model based on 995 women of which only 24 had GDM. Using such a strategy they were able to develop a model which identified 43% of women as requiring an OGTT and of these 75% of the women developing GDM were identified. Similarly, Nanda et al. 35 in a larger study produced a model which identified 60% of cases with GDM at a false positive rate of 20%.
Improvements in GDM screening may be possible by building upon the model of screening for aneuploidy by maternal history and characteristics and biomarkers, 36 which can now be applied to other pregnancy complications.37,38 Nanda et al. 35 and Ferreira et al. 39 include a variety of biochemical markers for GDM screening, such as sex hormone binding globulin (SHBG), total adiponectin and visfatin measured in maternal serum taken at the 11–13 week aneuploidy screening visit. In these studies, they found a 20% reduction in SHBG concentrations, a 30% reduction in adiponectin and a 30% increase in visfatin in pregnancies with GDM. Adding adiponectin and SHBG to the maternal/clinical characteristics algorithm, they found a 12% improvement in detection for GDM in women with no history of GDM and a smaller increase when adiponectin and visfatin were used. In neither model were PAPP-A or free hCGβ included.
Reduced concentrations of PAPP-A are an observation in pregnancies with Type 1 diabetes, and now also appear to be the case in GDM. In a group of diabetic and non-diabetic non-pregnant individuals, where PAPP-A has been suggested as a marker of acute coronary syndromes, there appears to be a distinct inverse relationship between PAPP-A and haemoglobin A1c. 40 It has been speculated that this could reflect an influence of glycaemic control on the regulation of PAPP-A expression. Whether this is a plausible mechanism during pregnancy requires further investigation.
Further studies are required in order to evaluate whether an algorithm incorporating PAPP-A and free hCGβ, along with SHBG and adiponectin and clinical prediction models would have a significant impact in screening for GDM. Certainly, in our practice the burden of GDM is high with over one-third of pregnancies requiring an OGTT and an incidence of GDM approaching 4% of pregnancies. Using proposed new criteria for the definition of GDM is only likely to increase the incidence of GDM further.
Footnotes
Declaration of conflicting interests
KS is a consultant for Brahms.
Funding
The Department has research funding from PerkinElmer.
Ethical approval
Not applicable.
Guarantor
KS.
Contributorship
KS designed the study, wrote the draft paper and contributed to the editorial process. NJC analysed the data, edited the draft paper and contributed to the editorial process.