
Abstract
Background
Using an online survey, we collected data to present a picture of how clinical authorization is performed in the UK.
Methods
A 21-question survey was uploaded to www.surveymonkey.com, and responses were invited via the mail base of the Association for Clinical Biochemistry and Laboratory Medicine. The questionnaire examined the intensity and function of the duty biochemist role and how different types of authorization are used to handle and release results.
Results
Of 70 responses received, 60 were suitable for analysis. Responses were received from every region of the UK. A typical duty biochemist shift started on average at 8:50, and finished at 17:25. The mean duration was 8 h 58 min. Clinical scientists are the most abundantly represented group on duty biochemist rotas. Higher banded clinical scientists and chemical pathologists covered out-of-hours shifts. Results were handled differently depending on the level of abnormality and the requesting area. Normal results tended to be released either directly from the analyser or after technical then autoauthorization (90%). A greater preference for clinical authorization was seen for abnormal and critical results originating from outpatients (49% and 69%, respectively) or general practice (51% and 71%) than for inpatients (33% and 53%) or A&E (25% and 37%).
Conclusions
The handling and authorization of biochemistry results varies greatly between laboratories. The role is clearly heterogeneous in the UK. Guidance from the Association for Clinical Biochemistry and Royal College of Pathologists may help to clarify the essential roles of the duty biochemist.
Introduction
Authorization is integral to the provision of clinical biochemistry services to clinicians. It serves to provide confidence in the veracity of results and in its different forms, including technical authorization, ensures the prompt telephoning or communication of critical results to clinical areas so that they can be acted upon. While there is agreement that authorization is important, there is great debate about the best method of its delivery. The amount of scrutiny depends on the clinical area responsible for the request and the level of abnormality. Based on these parameters, the authorization process may or may not include a combination of technical, clinical or autoauthorization. Currently, individual laboratories have different approaches to the challenge of authorization as there is no comprehensive guidance available.
The best practice guidelines issued by the Association for Clinical Biochemistry and Laboratory Medicine (ACB) acknowledges the impossibility of clinically authorizing every result generated. 1 In view of this obstacle, the ACB advocates the development of local laboratory protocols to select the most appropriate results to be clinically authorized. However, the document does not address other forms of authorization.
In contrast, the most relevant guidance available from the Royal College of Pathologists provides only a basic framework to inform the handling of results. 2 In addition to advising that results should be released in a timely manner, it suggests that urgent or abnormal results affecting patient management should be telephoned to the clinician concerned. The document goes further to discuss the provision of out-of-hours services, indicating that a process to identify and action critical results should be in place where appropriate. In both of these scenarios, the type and level of authorization to be employed is left open to interpretation.
Guidance from NHS England and the British Medical Association (BMA) acknowledge that the ordering clinician is traditionally responsible for acting upon abnormal results.3,4 The BMA, however, expects that life-threatening results are communicated promptly to the appropriate clinician, stating that the laboratory should phone out such results. The guidance does not address circumstances, where the ordering clinician is not identifiable or contactable, neither does it provide advice for managing an out-of-hours laboratory service.
The efficient running of a clinical biochemistry laboratory depends on striking the correct balance between the different authorization tools available. It is impractical and time consuming to clinically authorize every result, but equally the use of technical- and autoauthorization (autoauthorization is defined as the release of results to the clinical area without being reviewed by a person) alone may be over-sensitive to abnormal results and may inappropriately result in larger volume of calls placed to clinicians, 5 preventing the focus of clinical attention on the neediest of patients.
Using a national survey, we have collected information on the workload and roles of duty biochemists undertaking clinical authorization. We have also examined the bespoke use of the different types of authorization to handle patient results in individual laboratories and have collated this data to present a picture of current practice across the United Kingdom.
Method
A 21-question survey was designed and encompassed two distinct parts. The first part, containing 10 questions, sought to define the demographics of the respondent as well as information about the duty biochemist’s rota and responsibilities. The second part, containing 11 questions, focused on the results handling process, tasks undertaken by the duty biochemist on a routine basis and the respondent’s opinion about the role of duty biochemist. The questions and format of the survey are provided as supplementary Figure 1.
The questionnaire was converted to an online format (www.surveymonkey.com), and a web link to the survey was distributed on the ACB mail base, inviting as many responses as possible. Responses collected from 19 October 2015 to 21 December 2015 were analysed. The survey link was closed down on 12 January 2016.
Results have been reported as mean (± standard deviation) for parametric data, median (interquartile range) for non-parametric data, and n (%) for discrete or categorical data unless otherwise stated. Data distribution was assessed using the Shapiro-Wilk Test. In cases where ranges were provided in place of discrete data, the mean of the range was used in the analysis. For example, if the response to the number of hospitals covered by the duty biochemist was recorded as 2–4, then 3 was taken forward in analysis. All graphs and figures have been produced using Prism Graphpad 6.
Results
Summary of responses and the duty biochemist rota
There were 70 responses to the online survey, of which 60 were included in analysis of the objective data. Seven responses were excluded as they were duplicates from laboratories already represented in the data. One response was excluded, because it was from a laboratory in Australia, and two were excluded as they did not contain meaningful answers. Questions 19 to 21 elicited subjective information, for which 68 out of the 70 responses were analysed.
Forty-nine respondents represented laboratories in England, 18 of which were situated in London and the Southeast. Six laboratories in Wales, three from Scotland and two in Northern Island were also represented. A more detailed breakdown by region is shown in Figure 1.
Cartographical representation of respondent locations (n = 60). London and the South East: 18; South West: 4; East of England: 4; West Midlands: 6; East Midlands: 4; Yorkshire and the Humber: 4; North West: 5; North East: 4; Scotland: 3; Northern Ireland: 2; Wales: 6.
The majority of respondents were clinical scientists ranging from bands 7 to 9, who accounted for 42 responses (70%). One response (1.7%) was completed by a biomedical scientist, nine (15%) and three (5%) were from chemical pathology consultants and registrars respectively, and the final five (8.3%) were chemical pathology (metabolic medicine) registrars. The median (interquartile range) start time for a duty biochemist day shift was 9:00 (8:56–9:00), finishing at 17:30 (17:00–17:30) corresponding to median duration of 8.5 h (8.5–9 h). The median number of people on the duty biochemist rota was 4 (2–7), undertaking a median of 5 (4–9) daytime shifts per month. The mean number of hospitals covered during a duty biochemist shift was 2.15 (±1.30). The mean number of duty biochemists working at one time during the day was 1.30 (range 0.5–3). This correlated to an average of 1.81 hospitals covered by an individual duty biochemist.
One laboratory did not have a formal duty biochemist role, with a set start and finish time. The service at this location was run by one chemical pathology consultant and one part-time clinical scientist. In this laboratory, results marked for clinical authorization or input were released to the clinical area and simultaneously placed in a queue (a list of results) to be reviewed and actioned at the earliest opportunity.
Personnel represented on rotas
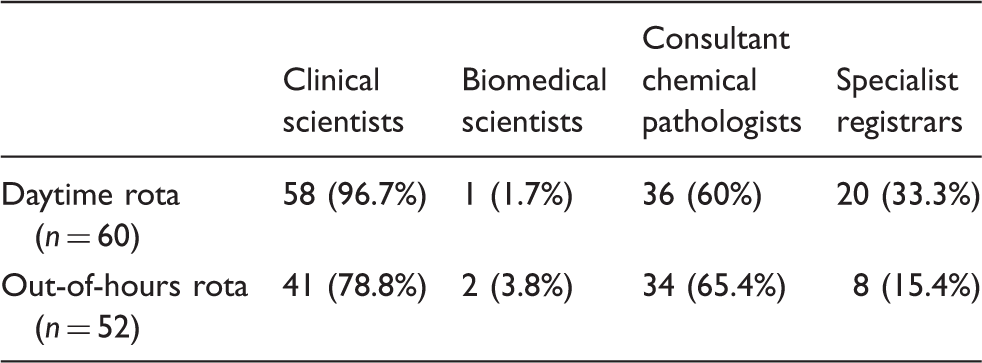
Fifty-eight (96.7%) laboratories recorded clinical scientists on their daytime duty biochemist rota, of which 22 used band 7s, 28 had band 8As, 25 had both band 8Bs and 8Cs, 20 had band 8Ds and 10 recorded band 9s. Biomedical scientists were represented on the rota in 1 (1.7%) laboratory, consultant chemical pathologists were counted on 36 (60%) and registrars on 20 (33.3%) rotas. When examined in greater detail, the majority of laboratory daytime rotas were staffed with consultant chemical pathologists and clinical scientists as reported by 34 (56.7%) respondents. Twenty-two (36.7%) used clinical scientists alone and in contrast, only two (3.3%) laboratories had rotas staffed with consultant chemical pathologists alone.
Number of laboratories that staff duty biochemist rota with professionals by classification represented as number (percentage).
Results handling
Breakdown of responses demonstrating how results are handled according to clinical area and level of abnormality.
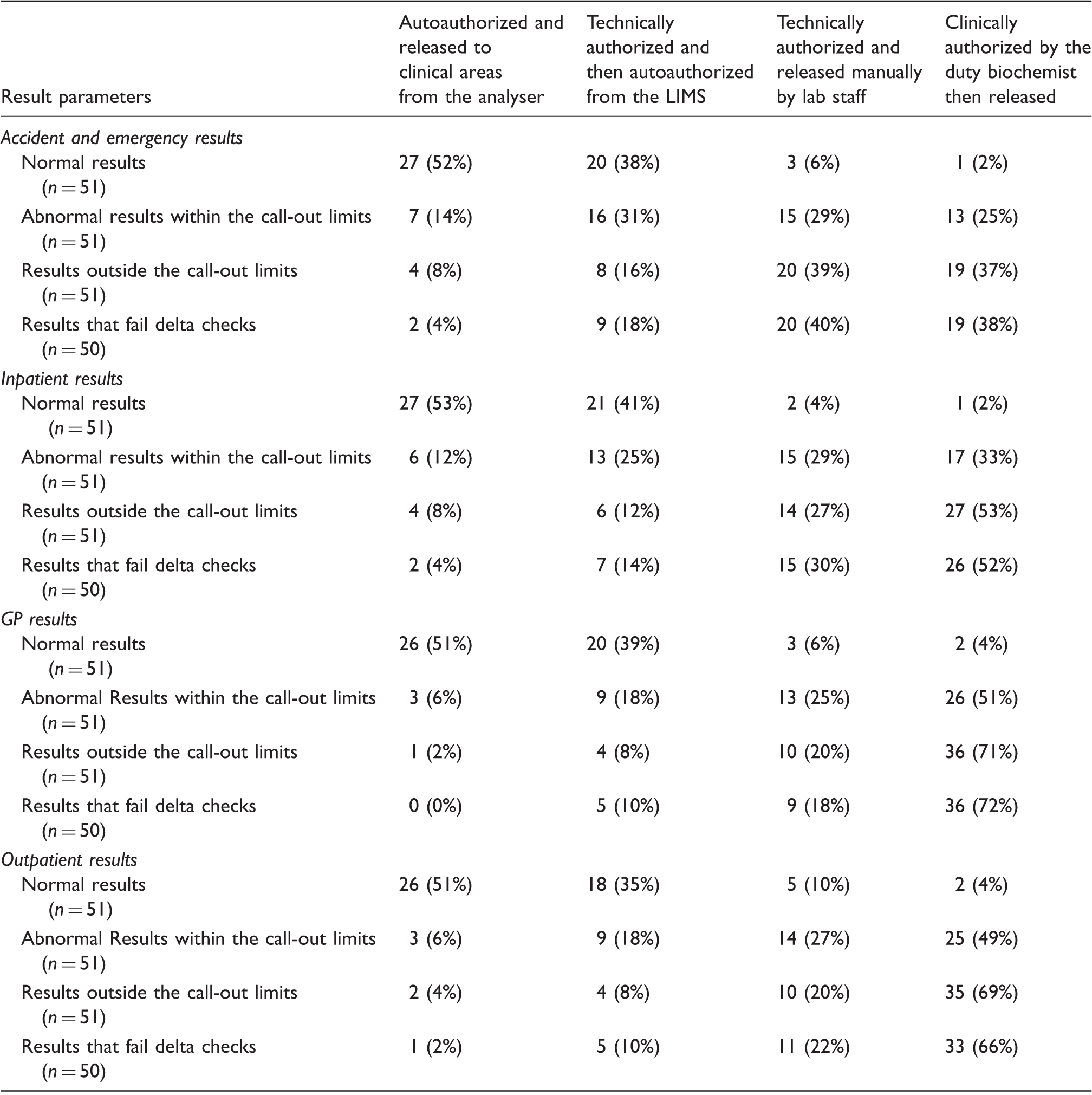
Note: Data are represented as number (%).
LIMS: laboratory information management system.
Normal results (n = 51) were handled homogenously regardless of the requesting clinical area, with 86% to 94% of laboratories releasing either from the analyser after autoauthorization or autoauthorization following technical authorization. Only 2–4% of laboratories clinically authorized normal results.
Abnormal results within the call-out limits (n = 51) (call-out limits were defined as a preagreed trigger level at which a result is urgently telephoned to the requestor) were less commonly released from the analyser after autoauthorization, with 6–14% of laboratories adopting this approach. When originating from A&E or inpatient clinical areas, abnormal results were not clinically authorized in 75% and 67% of laboratories. When originating from outpatients or GP practices, a large proportion of laboratories opted for clinical authorization (49% and 51%, respectively).
Critical results outside of the call-out limits (n = 51) and results failing delta checks (n = 50) were mostly manually released after technical authorization if the requests were from A&E (39% and 40%, respectively). When originating from inpatients, there was a shift towards clinical authorization with 53% and 52% of laboratories opting for this approach. A greater reliance on clinical authorization was observed for critical results and results failing delta checks when the requests originated from outpatients or a GP setting, with 68–72% of laboratories sending these results to the duty biochemist.
Breakdown of responses identifying whether results are retrospectively or prospectively reviewed by the duty biochemist according to the requesting clinical area.
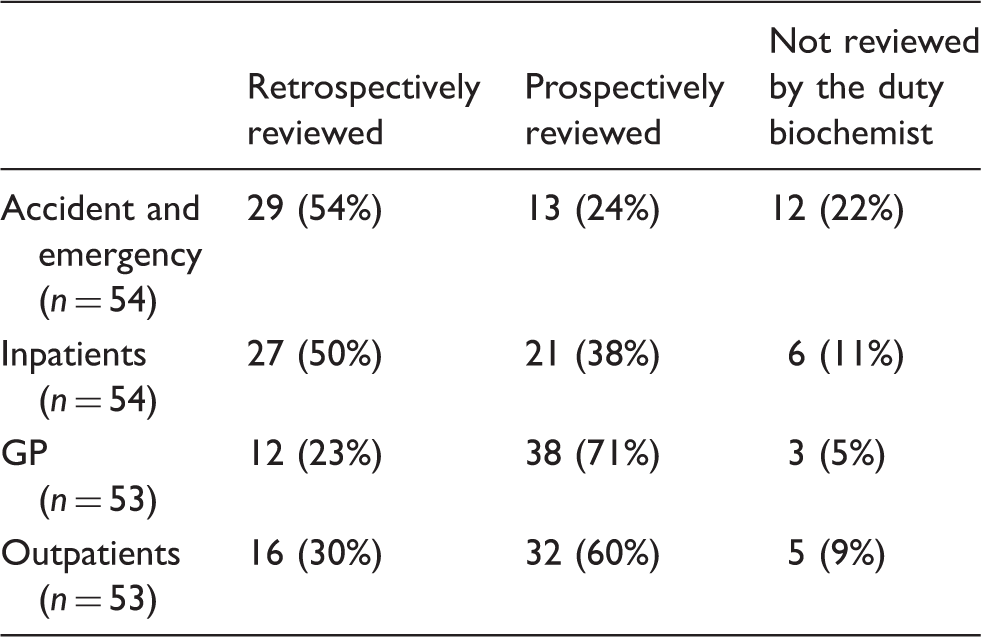
Note: Data are represented as number (%).
The most commonly used laboratory information management system was Clinisys Winpath, implemented in 11 (19.3%) of the laboratories that answered (n = 51). The next most widely used software was Telepath, found in seven (13.7%) laboratories, followed closely by Clinisys Labcentre which was mentioned by six (11.8%) respondents. The remaining brands of software used can be found in Figure 2.
Breakdown showing frequency of specific software used by individual laboratories.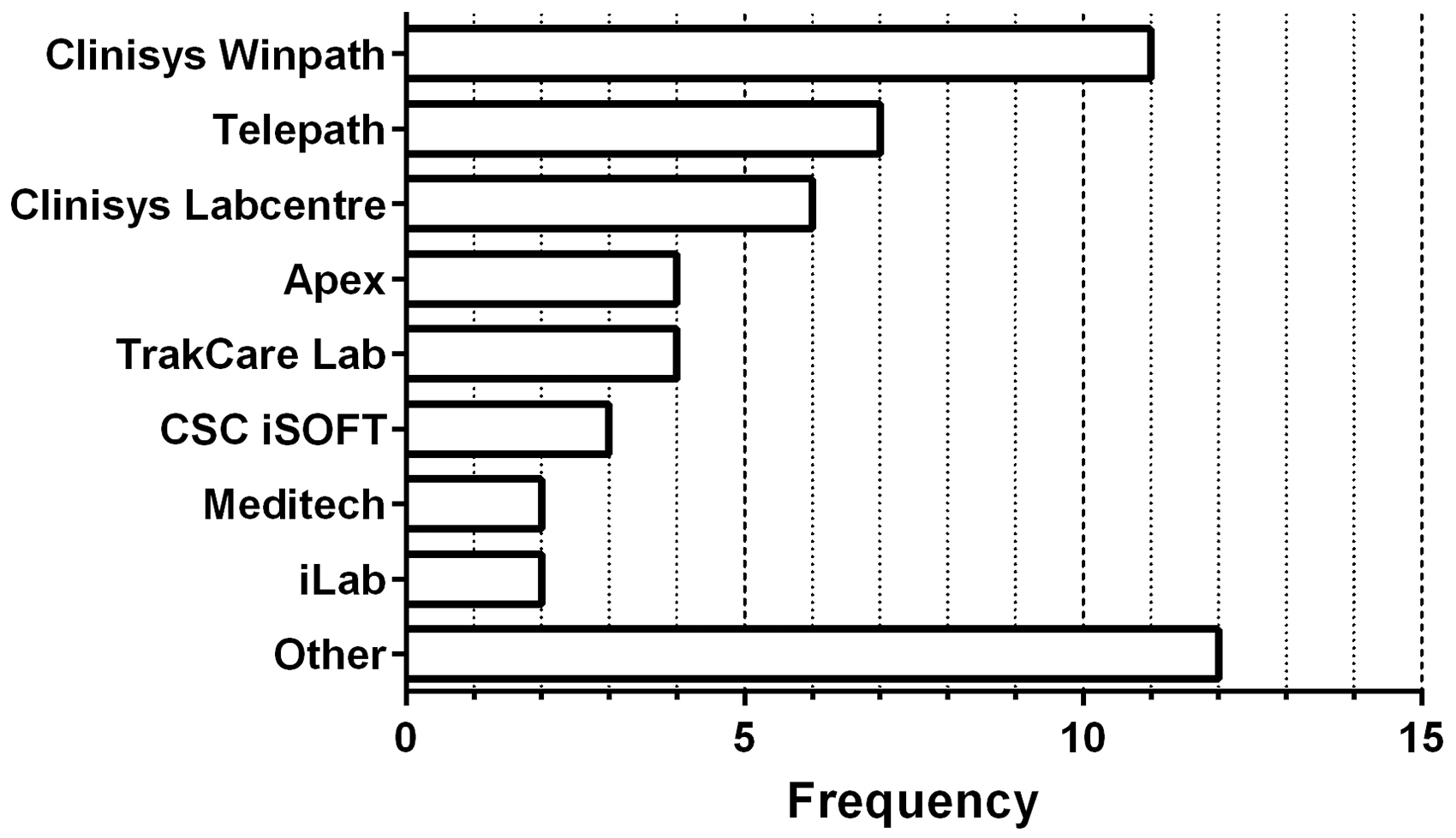
Queues of results sent to the duty biochemist in 22 (39.3%) responses involved separation of results according to groupings of tests including endocrine, tumour markers, proteins, etc. Many centres separate their queues using multiple criteria, which were not mutually exclusive. Often, there was segregation of GP results as reported in 12 (21.4%) responses and outpatient results in 11 (19.6%) laboratories. One group of nine (16.1%) laboratories created specific queues for individual hospitals served, while another group of nine (16.1%) separated results according to whether they were requested as urgent or routine. Nine (16.1%) different respondents did not separate results, reviewing them all as one large queue.
Duty biochemist tasks
From a total of 55 respondents who answered the question, 54 (98.2%) described providing phone advice to hospital staff and GPs as routine tasks for the duty biochemist. Forty-five (81.8%) reported vetting send-away tests as part of their role, and 39 (71.0%) regularly reported and released other test results, for example CSF xanthochromia, HBA1c, protein electrophoresis and macroprolactin. Ringing out abnormal blood results constituted a routine role for 38 (69.1%) individuals when acting on GP results and 31 (56.4%) respondents when the request originated from the hospital. One respondent did not have a formal duty biochemist system, and therefore did not record any routine tasks.
When questioned about the three most time-consuming tasks, 35 (63.6%) of the 55 respondents identified authorizing or validating results. Communicating abnormal results and managing phone calls were both cited by 14 (25.5%) respondents. Twelve (22.8%) felt that providing advice to clinical areas and providing advice to the laboratory were time intensive. Ten (18.2%) recorded reviewing send-aways, five (9.1%) mentioned appending comments to results and four (7.3%) felt that correcting errors was amongst the most time-consuming tasks.
Forty-nine individuals answered the final question regarding their opinion about the ideal role of the duty biochemist. Forty-two (85.7%) regarded vetting send-aways as an important job. Thirty-eight (77.6%) felt that providing advice was integral to the role, and reviewing results was recorded by 26 (53.1%).
Discussion
The results of this survey demonstrate that the duty biochemist position is employed extensively throughout the UK. There is a demand for clinical authorization during both working hours and out of hours, with the majority of laboratories maintaining rotas for all hours of the day. With reduced primary and secondary care provisions during unsociable hours, the value of an out-of-hours service should not be understated. Evidence suggests that the presence of an out-of-hours duty biochemist reduces the number of call-outs made for results that exceed call-out limits. 5 This has the net effect of focussing resources on the sickest of patients and easing the workload that would otherwise engage emergency out-of-hours services. Despite suggestions that approximately 10% of deferred out-of-hours results required acute attention within 48 h, 5 there is a distinct absence of safety data fully assessing the risk of harm to individuals whose results are deferred. A careful balance is required between the risk of harm, and the risk of causing false alarm through over-sensitivity, seen when laboratory staff directly call-out critical results. 6
Considerable variation is evident in the way that the duty biochemist role is staffed and managed; however, certain trends have emerged. Clinical scientists are found on nearly all of the daytime and the majority of the out-of-hours duty biochemist rotas. There is a shift towards utilizing more senior bands during unsocial hours, with the majority of daytime clinical scientists being between 7 and 8c, compared with more than half being bands 8c to 9 at night. This is likely to reflect the need for greater experience associated with seniority, which is required when providing laboratory advice or making unilateral decisions regarding whether or not to telephone abnormal results. In keeping with this trend, we observed a greater proportion of consultant chemical pathologists on out-of-hours rotas than on daytime rotas, likely drawing on their clinical experience.
In comparison, biomedical scientists were less well represented on both daytime and nighttime rotas, with a greater presence on the nighttime rota. Whether the biomedical scientists are concurrently working in the laboratory at the time that they are acting as duty biochemist remains unclear, as does their banding. However, the prospect of staff adopting simultaneously a laboratory role and that of the duty biochemist potentially removes the additional step of informing another person of the critical result. This permits faster transmission of the result to the emergency out-of-hours services and reduces the resources needed to run a clinical chemistry laboratory. It is nevertheless necessary to elucidate whether the laboratories that use this system have observed any increase in adverse events and whether there is a mechanism for escalation or seeking further advice if required.
Our data are limited by the under-representation of biomedical scientists in our responding population. This sampling bias is likely to be the result of solely disseminating the survey on the ACB mail base, which is populated principally by clinical scientists and chemical pathologists. The majority of responses were received from London and the southeast, leaving other regions of the UK relatively under-represented.
Our study has acquired an understanding of the way that results with different requesting locations and varying degrees of abnormality are authorized and released. As expected, normal results were largely released without clinical input. A distinct dichotomy was seen in the processing of abnormal results exceeding the call-out trigger limits. At least two-thirds of results originating from A&E and inpatients were released to clinical areas without clinical authorization. In contrast, approximately half of abnormal results originating from outpatients or GP practices were clinically authorized. This approach facilitates faster release of results to the clinical areas where fast turn-around times are the most valuable, by reducing the number of steps prior to release and arguably excluding the most time-consuming step of clinical authorization. Conversely, results from outpatients and GPs are more closely scrutinized, potentially reducing the time taken to act on results which would otherwise have been reviewed by the requesting clinician on another day.
Critical results and results which fail delta checks, originating from GPs or outpatients were similarly handled with approximately 70% being clinically authorized. A divergence was noted between such results originating from A&E and inpatients. Most laboratories favoured expedient publication of A&E results, with only 37–38% being reviewed by the duty biochemist. When these results originated from inpatients, there was shift towards clinical authorization, with approximately half of laboratories opting for this approach. This suggests that when results are abnormal beyond a threshold, the emphasis for inpatient results is to provide an extra level of safety rather than focussing on the quicker release of results. However, in most hospitals, despite the severity of the abnormality, the main objective is the timely release of results, where A&E is concerned. This approach has likely been informed by the national emphasis on meeting 4 h waiting time targets in A&E.
Our findings suggest that most respondents have adopted a targeted use of duty biochemist time by clinically authorizing selected results. While there is little value to be gained from reviewing normal results, clinically authorizing GP and outpatient results will help to identify high-risk patients within a shorter timeframe to ensure that they are assessed earlier than would otherwise be possible. Furthermore, clinical authorization is less likely to be employed, where the release of results is time sensitive. Unfortunately, our questions in this section were not designed to detect laboratories that release results prior to retrospective clinical authorization. A further limitation is the absence of data on the actual time taken to release results in each abnormality category, preventing us from quantifying the magnitude of the delay caused by clinical authorization.
Approximately 50% of laboratories reported that that A&E and inpatient results were retrospectively reviewed by the duty biochemist. In contrast, 71% of respondents recorded that GP results were prospectively reviewed. The reason for this large number is not immediately clear. It is possible many laboratories release GP results after review to allow them to append comments. We cannot exclude that respondents may have considered technical authorization as a form of prospective review when answering this question. We have also speculated, from our experience, that GP blood samples may be run overnight during quiescent periods, meaning that the results are held in a queue overnight to be reviewed and released by the duty biochemist the next morning. This presents a point of inquiry in any future survey.
One respondent to this survey informed us that no formal duty biochemist system existed at his hospital. Instead, he was available around the clock to provide advice and assistance on an ad hoc basis as required. From this example, it is clear that this type of arrangement may work in some hospitals while providing an excellent standard of care. We suspect that this system may be at risk of overwhelming the de facto duty biochemist if demand, such as that seen in large centres, is routinely very high.
Forty-nine respondents answered the last question to express their opinion of what the duty biochemist role should entail. An overwhelming number were clear that role should add value and should not include time-consuming and cost-ineffective tasks such as vetting routine send-away tests. Others suggested that the role should include providing guidance on specialist and uncommon tests, perhaps in the hope of avoiding unnecessary investigations which are a drain on resources. There was feeling that the duty biochemist’s skill set should be exploited, with a greater focus on providing clinical advice and proactively calling clinicians about extraordinary cases, where input would be valuable. A large number of responses indicated that reviewing results was a good a use of time, although some were keen to stress that only abnormal results should be reviewed and that interpretative comments are added where appropriate. There is, however, only limited evidence that interpretative comments influence patient management. 7
Conclusion
Our study has highlighted the variation in how laboratories are run across the United Kingdom and how results are handled. There is currently no comprehensive uniform guidance on how authorization should be conducted, or the minimum requirement expected of individuals who undertake the duty biochemist role. In this vacuum, specific guidelines from the Royal College of Pathologists or ACB may help to clarify the essential roles of the duty biochemist. This guidance should take into account that most chemical pathology laboratories are currently understaffed. 8 The trend of increasing general practitioner and hospital requesting will probably be associated with an increased requirement for clinical liaison, clinical advice and clinical audit. Accordingly, there is likely to be an increased demand on an already stretched service.
To obtain a fuller picture of the authorization process, a larger and more inclusive study is required. This should be designed to limit sampling bias by gaining representation of all categories of pathology staff. This would allow exploration of the responsibilities of individual roles including the professional limits on providing and standardization of interpretative comments. Regions within the UK should be proportionally represented according to the number of laboratories within their boundaries. Such a study should perhaps be in the form of a national audit.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
Not applicable.
Guarantor
JC.
Contributorship
JC conceived the study. SC, EW, SB, JAZ, TT and JC were involved in the survey design and data analysis. SC wrote the first draft of the manuscript. All authors reviewed and edited the manuscript and approved the final version of the manuscript.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.