
Abstract
Aim
The aim of the study was to review the clinical validation process of out of hours critical biochemistry results by a clinical biochemist and its effect on primary care services.
Methods
A prospective study was conducted of all critical results for primary care patients who were analysed out of hours. The nine-month study period was conducted between June 2013 and February 2014. The data collected include patients’ age, clinical details, critical results and the urgency of result communicated. The patients’ subsequent attendance rate at the emergency department in the local hospital was reviewed.
Results
A total of 311 out of hours critical results were identified in the laboratory. After clinical validation, 110 (35.4%) results were telephoned urgently and 155 (49.8%) results were deferred to the next day. Forty-six (14.8%) results were not telephoned. Following the urgent result communication, 53/110 (48.2%) patients attended the hospital emergency department within 24 h and 17/110 (15.5%) had their repeat blood test by their general practitioner surgery within 48 h. When the result was telephoned during working hours the next day, only 15/155 (9.7%) attended the hospital acute services within 48 h and 16/155 (10.3%) had repeat blood test at their general practitioner surgery.
Conclusion
In our practice, the clinical validation of out of hours critical results by a clinical biochemist is associated with a reduction in the number of results telephoned when compared against the critical limits list recommended by the Royal College of Pathologists and may focus out of hours clinical activity on more suitable patients.
Introduction
A critical biochemical result reflects a significant pathophysiological state in a patient, which may require urgent intervention. The Royal College of Pathologists (RCPath) has published a document stating the critical limits for communicating results to the requesting primary care physician 1 and also included a time interval for this activity in their list of Key Performance Indicators (KPI). 2 It is relatively easy to communicate with clinicians during the core working hours. However, when critical results become available for outpatients and primary care patients out of hours (OOH), the laboratory can only communicate with an on-call clinician who in most cases is completely unfamiliar with the patient. This is not an infrequent scenario as blood samples from primary care may arrive in the laboratory late in the afternoon and be analysed in the early hours of the evening.
The action limits for critical results communication are agreed by local laboratories and primary care services. The RCPath has published illustrative critical result limits 1 which can be adapted to local requirements. In the UK, critical results are telephoned either by biomedical scientists (BMS) who are not clinically trained or by clinical biochemists (CB) with either scientific or medical background. Clinical validation of the results by the latter group includes a clinical judgement based on patient demographics, clinical details, sample timing and previous results. This process is valuable as not all the initial results require urgent clinical action; for example, hyperkalaemia in a sample that has been delayed in transit or a high but stable creatinine concentration in a patient with chronic renal failure. This will result in a proportion of such critical results being communicated the following day rather than OOH.
Aim
The aim of the study was to review our current clinical validation process of OOH critical biochemistry results and its effect on primary care services.
Background
The Blood Sciences laboratory in Leeds Teaching Hospitals provides a 24 h service, seven days a week, for primary care and two major teaching hospitals covering a population of approximately 800,000. It is a longstanding practice in our laboratory that all the OOH critical results identified by the BMS are reviewed by the on-call CB who validates the results clinically and decides on the urgency of communication. All the urgent results are phoned to the local call system (Local Care Direct) that coordinates the OOH primary care service. If the CB regards the results as non-urgent, the call out is deferred to next day when general practitioner (GP) surgeries are open. The purpose of this study was to evaluate the impact of clinical validation of results during OOH. The OOH system reflects the daytime practice of clinical validation which is staffed by a CB.
Methods
The study involved prospective collection of all OOH (i.e. 17:00 to 09:00 on week days and 13:00 to 09:00 on weekends) critical results from primary care for the period of nine months between June 2013 and February 2014. The action limits for critical results were as defined by the RCPath document 1 and the limit for paracetamol was derived from local agreements. The collected data included patient age, clinical details, critical results and the urgency of the result communicated to the GP. The patient details for this study were obtained one month after result communication through the hospital electronic patient records and the laboratory information system (Telepath®, UK) to identify further management of individual patients. The outcome of the result communicated to primary care was defined as (1) no action taken, (2) repeat test by the GP within 48 h or (3) urgent attendance to the local hospital within 24 h of result communication.
Results
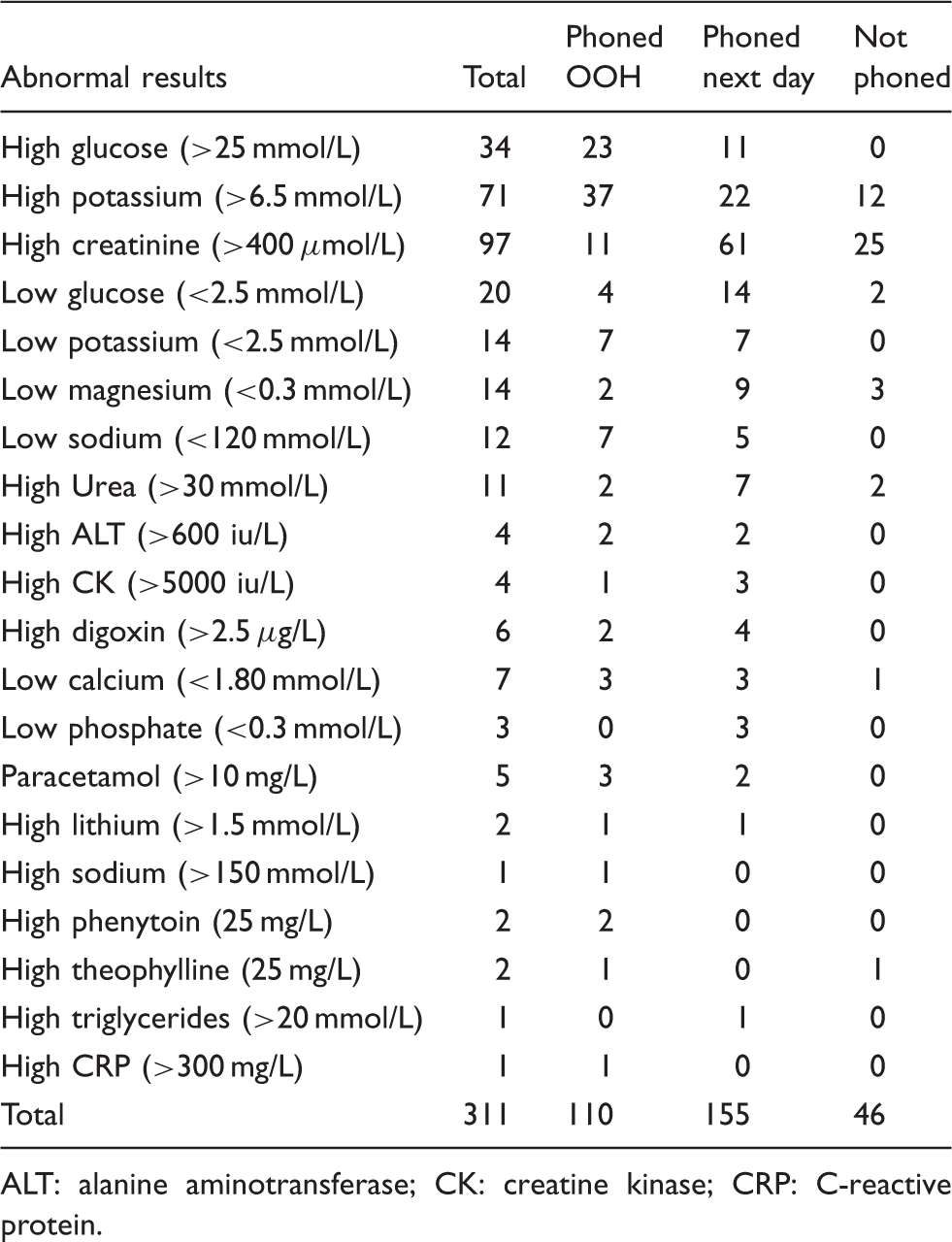
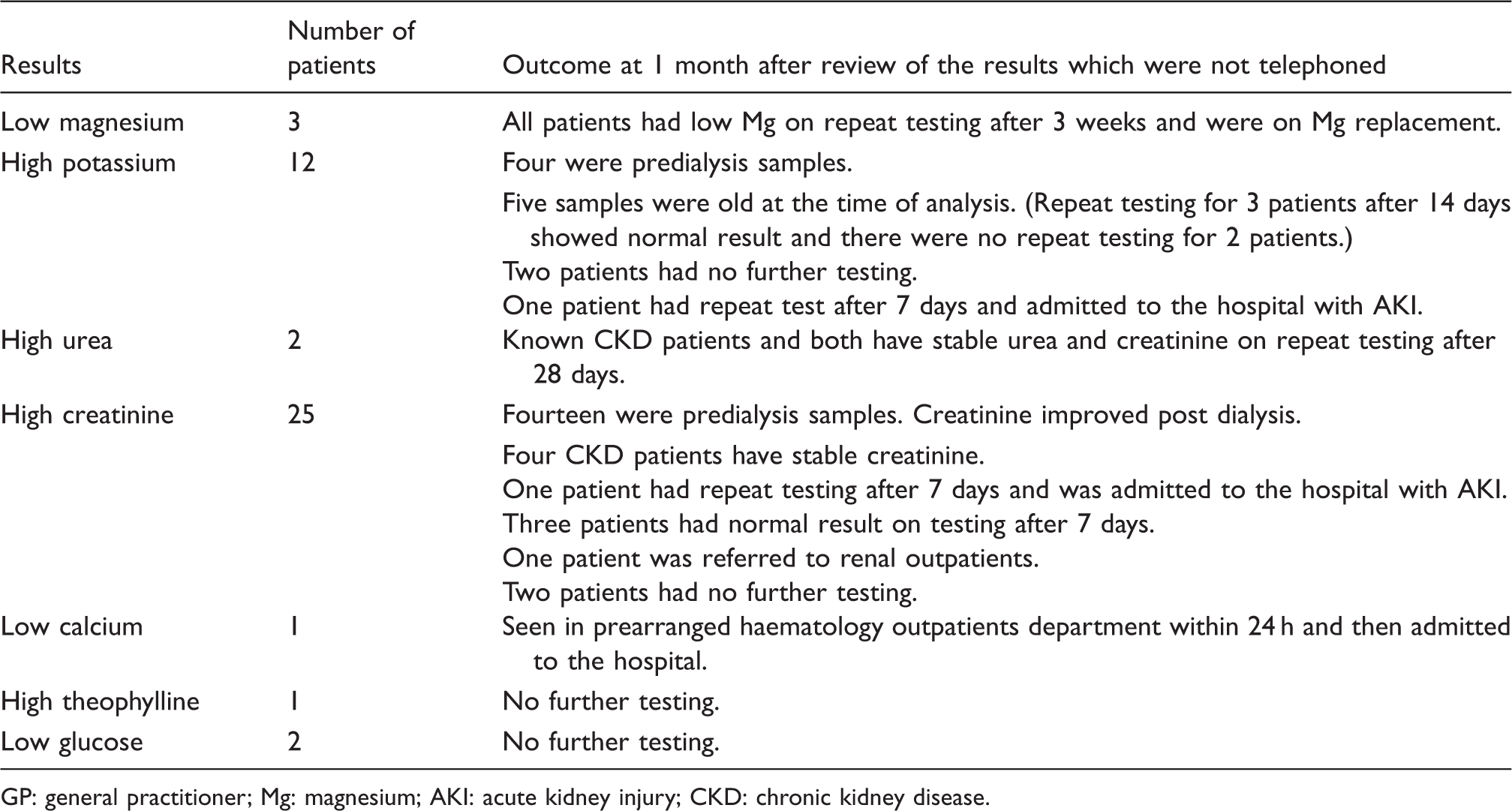
A total of 311 OOH critical biochemistry results from primary care were identified during the study period (Figure 1). After clinical validation, only 110 (35.4%) results were telephoned to Local Care Direct and 155 (49.8%) results were deferred to be telephoned the next day during normal working hours. Forty-six (14.8%) results were not communicated as these patients were known to have underlying disease accounting for the abnormality. The majority of critical results reviewed OOH were high creatinine (31.2%), high potassium (22.8%) and high glucose (10.9%). Details of all critical results reviewed are provided in Table 1. Following the urgent OOH critical result communication 53/110 (48.2%) patients attended the hospital emergency department (ED) within 24 h and 17/110 (15.5%) had a repeat blood test taken by their GP within 48 h. However, if the critical result was telephoned during working hours next day only 15/155 (9.7%) attended the hospital acute services within 24 h and 16/155 (10.3%) had repeat blood test at their GP surgery. Three out of 46 (14.8%) patients (Table 2) whose results were not telephoned were admitted to hospital later: two patients with worsening of acute kidney injury were admitted by the GP and one patient with hypocalcaemia was admitted the next day from haematology outpatients.
Outcome of the out of hours (OOH) results reviewed. ED: emergency department; GP: general practitioner. Details of abnormal results reviewed. ALT: alanine aminotransferase; CK: creatine kinase; CRP: C-reactive protein. Outcome of the patients whose results were returned to the GP surgery without being phoned. GP: general practitioner; Mg: magnesium; AKI: acute kidney injury; CKD: chronic kidney disease.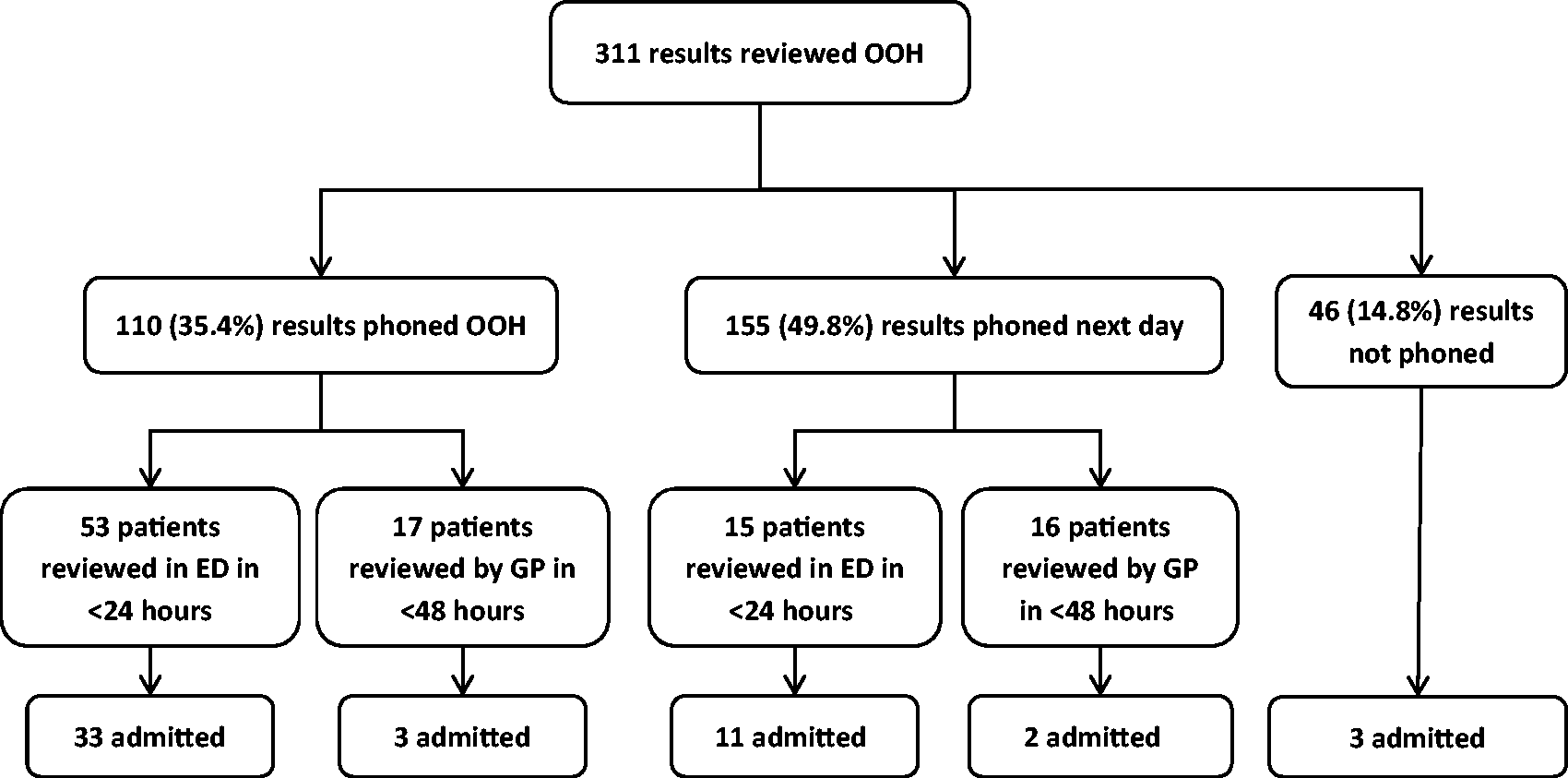
Outcome of 40 patients whose results were telephoned OOH but did not have a repeat test or review by the GP within 48 h.
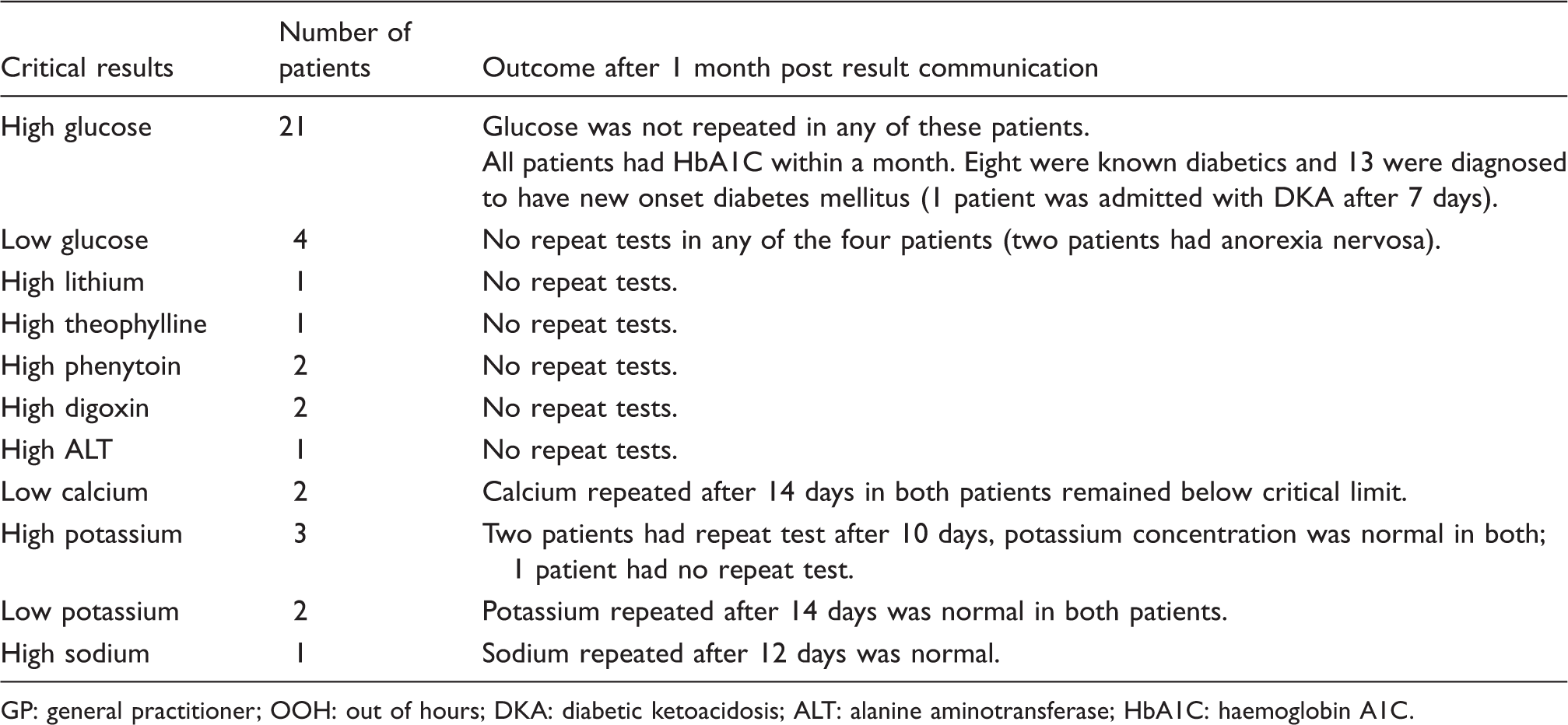
GP: general practitioner; OOH: out of hours; DKA: diabetic ketoacidosis; ALT: alanine aminotransferase; HbA1C: haemoglobin A1C.
Discussion
Clinical validation of laboratory data is part of the post-analytical process. This process acts as a final quality control procedure and also permits a clinical oversight of the data, which may demonstrate disease patterns on which the CB can provide guidance and interpretation. It also serves to identify those patients with critically abnormal test results who may require immediate or early clinical intervention. We have shown in this report that communication of some critical results can be delayed to the following day. While the use of clinical staff to perform validation OOH might be considered a costly service, this needs to be balanced against reduced OOH care provider workload.
In our study, a larger proportion of patients were admitted OOH if the abnormal results were telephoned immediately rather than deferring until the following day (32.7% vs. 8.3%). This observational finding appears to support the role clinical validation in identifying those patients who require more immediate clinical action. However, we noted that some (3/46) patients were subsequently admitted when a decision had been taken not to phone results. Two of these patients had blood tests repeated after seven days at which point they were both admitted with acute kidney injury, while one was admitted with hypocalcaemia from a scheduled outpatient appointment. It is unclear whether earlier communication of the test results might have altered the clinical management of these patients.
Our study complements a study from Spain in which two adjacent laboratories had different practices. The laboratory without clinical validation communicated more results urgently (approximately four times higher) and caused more false alarms. 3 A systematic review by Liebow et al. 4 showed that an improvement in laboratory test handling for in-patients can be achieved with trained staff, dedicated call centres and use of information technology (IT) to improve communication. In practice, it is difficult to achieve good IT links across different organizations such as hospitals and primary care. The CB has a role in examining all the available patient data in order to risk stratify critical results and aid patient safety. This process is difficult to automate fully as shown by previous national audits. 5
The issue of laboratory liaison with primary care physicians has been noted in the UK by the Royal College of General Practitioners, which has highlighted the difficulties that laboratory staff may experience in contacting the appropriate primary care clinician. 6 This advice complements the RCPaths’ advice on OOH reporting to primary care 4 and also the standard set by Clinical Pathology Accreditation (UK) Ltd. 7 This study highlights the usefulness of this process. The professional bodies may be able to co-operate to develop further the mutual benefits of liaison between the laboratory and primary care.
Conclusion
Our observational study suggests that clinical interpretation of critical results can help differentiate those results that need immediate intervention from those which can be deferred until the next day. This process also reduces the number of results telephoned compared with the list recommended by the RCPath and may focus OOH clinical activity on more suitable patients. Further research is needed to demonstrate whether OOH clinical validation of results can reduce hospital admissions.
Footnotes
Acknowledgements
Dr M.P. Bosomworth, Dr M.J. Henderson and Dr D. Thompson for their valuable help with the data collection during the study period.
Declaration of conflicting interests
None declared.
Funding
None declared.
Ethical approval
Not required, study approval obtained from Leeds Teaching hospitals audit department.
Guarantor
JHB.
Contributorship
All authors have been involved in conceiving the study and writing the paper. All authors have reviewed the final manuscript.