
Abstract
Introduction
Our dried blood spot vitamin D testing service enables members of the public to assess their vitamin D status. Vitamin D has become popular with the media and the general public. We noticed that our direct access service had a higher rate of high to toxic 25-hydroxyvitamin D levels compared with our GP population and we wanted to know why.
Methods
Between January 2013 and September 2015 we contacted all direct access users who had 25-hydroxyvitamin D >220 nmol/L measured using LC/MS/MS. We investigated the amount, type and length of supplementation used and whether or not users were medically supervised.
Results
A total of 372 service users had 25-hydroxyvitamin D concentrations >220 nmol/L. Of 14,806 direct access samples received, 372 (2.5%) were from users with 25-hydroxyvitamin D concentrations ranging from 221 to 1235 nmol/L. Only 0.06% of GP patients had results >220 nmol/L over the same time frame. There were 361 direct access users regularly supplementing, taking between 1000 to 120,000 IU/day. Two users took bolus doses of 300,000 and 900,000 IU. Only 23 users taking supplements (6.4%) were under medical supervision. There were 28 users with levels >500 nmol/L, but only one was under medical supervision. The internet was the main source of supplements (74%).
Conclusions
The proportion of high to toxic concentrations of vitamin D was higher in direct access users than in the GP population. Many people were taking more than the Institute of Medicine's recommendation of 10,000 IU/day, yet only a few were being medically supervised. Clinicians should be aware that patients may be self-administering very high concentrations of vitamin D, especially when investigating unexplained hypercalcaemia.
Introduction
The concentration at which vitamin D toxicity can occur has been a contentious issue for many years, as indeed is the concentration at which a person can be considered to have an adequate concentration of vitamin D and how much vitamin D can be safely taken. This has resulted in multiple guidelines with varying recommendations.1–9 However, reports of vitamin D toxicity can be regularly seen in the literature,10–14 and this is a very real, and often avoidable, problem.
Hypervitaminosis D can lead to hypercalcaemia as a result of increased intestinal calcium absorption and bone resorption, which can ultimately lead to kidney injury. 15 The effects of long-term high-dose vitamin D supplementation are not well known; however, it appears that not only is hypercalcaemia and hypercalciuria a risk but other detrimental side-effects such as increased falls 16 are being acknowledged with some suggesting that there may be a U-shaped curve for 25-hydroxyvitamin D concentrations.2,17,18
Vieth stated that hypercalcaemia due to vitamin D intoxication is always associated with 25-hydroxyvitamin D concentration >220 nmol/L, 19 although more recently other reports have revised this concentration upwards to 250 or 375 nmol/L.20,21 We therefore contacted members of the public using our vitamin D direct to the public blood spot testing service who had a result >220 nmol/L, to establish what supplementation regimes were being followed causing them to have such high concentrations. In particular, we wanted to find out if people were being medically supervised, how much they were taking, what brand and formulation they were taking, how long they were supplementing for, and where they had obtained their supplements from. This is the first time, to the best of our knowledge, that such a cohort of people has been interviewed. It is important to know what sort of supplement regimes that members of the public are following and how this can lead to high concentrations of 25-hydroxyvitamin D.
Methods
Direct to the public vitamin D testing service
We introduced a direct to the public vitamin D blood spot testing service in July 2011. Members of the public can purchase a blood spot testing kit from us via our website or via a healthcare practitioner that they are using (e.g. nutritionist, osteopath and pharmacist). The user receives the kit in the post, takes the sample and sends a blood spot card back to the laboratory. After analysis, a PDF report is generated stating the total 25-hydroxyvitamin D results as well as a breakdown of the component concentrations of 25-hydroxyvitamin D2 and 25-hydroxyvitamin D3. In addition, the vitamin D status of the user is highlighted and the reference ranges supplied. PDF reports are then sent out to the user, normally via email. If the total 25-hydroxyvitamin D is >220 nmol/L, users are contacted via telephone first to discuss the implications of their high result, before the PDF report is issued. This service is available both nationally and internationally.
25-hydroxyvitamin D analysis
25-hydroxyvitamin D2 and D3 were analysed in dried blood spots by tandem mass spectrometry after derivatization and liquid–liquid extraction, using in house calibrators and quality control material. The 25-hydroxyvitamin D was extracted from the filter paper by sonicating in water containing deuterated 25-hydroxyvitamin D2 and D3 internal standard. The dried blood spot method was aligned with our serum 25-hydroxyvitamin D2 and D3 method which resulted in blood spot vitamin D concentrations that were the equivalent of serum concentrations. The methods were aligned by assigning values to the in-house calibrators based on the plasma 25-hydroxyvitamin D concentrations obtained from the whole blood used to make the calibrators.
Serum samples were analysed by tandem mass spectrometry after liquid–liquid extraction using Waters suggested sample preparation and mass spectrometer parameters. The serum method used commercially available calibrators and internal quality control material. An external quality assurance scheme (DEQAS) was participated in for the serum assay, and paired blood spot and serum samples were also used as part of the quality control process for the blood spot assay.
The following reference ranges were used and relate to total 25-hydroxyvitamin D concentrations: severely deficient <15 nmol/L, deficient 15–30 nmol/L, insufficient 30.1–50 nmol/L, adequate 50.1–220 nmol/L, high to toxic 220.1–500 nmol/L, toxic >500 nmol/L.
Population selection and telephone interview
Between January 2013 and September 2015, all users of our direct to the public vitamin D testing service whose total 25-hydroxyvitamin D concentrations were >220 nmol/L were contacted by telephone. This was to appropriately inform users of their potentially toxic result and suggest how to respond to it. After explaining the reason for the phone call, users were asked if they were happy to discuss their supplementation regime in more detail. If so, we ascertained the extent of medical supervision and vitamin D supplementation, formulation, brand, source of supplements and finally the length of time supplemented for. If further information was volunteered (e.g. reason for supplementation, additional supplements being taken), this was also recorded. The option of confirming their result using a serum sample at no charge was also offered. This option was given as some users had said that general practitioners (GPs) wanted to confirm vitamin D results but were unable to do so with their local service. Other users questioned the dried blood spot result, and so we confirmed the result using paired serum and dried blood spot samples. This option was available to all users of the service if required, not just those who had a high result.
All users were encouraged to discuss their results with their GP and advised to immediately stop all supplements containing vitamin D, unless these had been prescribed to them. Telephone interviews lasted between 5 and 30 min.
Data analysis
The results of the telephone interview were tabulated along with any previous results on the patient and the initial high result. The age and sex of the patient and the date the sample was taken were also recorded. Trends relating to whether or not patients were under medical supervision, the amount of supplements taken, formulation of supplements and where the supplement was obtained were identified. General themes relating to reasons for supplementing and what other supplements were taken were also identified. Brands of supplements were checked to see if they existed as some users had difficulty recalling the brand of vitamin D they were taking. If the quoted brand could not be found, this was recorded as being an unverified brand.
Daily supplementation rates
Not all patients were taking daily supplements, but their equivalent daily supplementation rate was calculated based on the information provided. For example, if patients were taking a weekly supplement, the amount of supplement taken was divided by seven to provide a daily supplement rate. Some patients changed their regimes over time, and so their most recent regime leading to the elevated result was taken as the daily supplementation rate and the length of time supplemented for was taken as the time being on the latest dose. The data relating to supplementation patterns and length supplemented for were self-reported and unconfirmed.
Results
Population
Between January 2013 and September 2015, we analysed 14,806 blood spot samples. Of these, 454 (3.1%) samples had 25-hydroxyvitamin D >220 nmol/L. These samples came from 372 users. The age range of this group went from 19 weeks to 87 years, with a median age of 48 years, and 51% were women. There were 14 people who were aged 16 years or less. In comparison, for the same period we analysed 99,122 serum samples from our local GP population and 0.06% (n = 63) were found to have a 25-hydroxyvitamin D > 220 nmol/L.
Dried blood spot 25-hydroxyvitamin D results
The results ranged from 221 to 1235 nmol/L with a median concentration of 274 nmol/L. The majority of results were less than 375 nmol/L (83%, n = 310). There were 32 people who had a 25-hydroxyvitamin D concentration >500 nmol/L, but only one of these had a result >1000 nmol/L.
There were 35 users over the time frame who chose to confirm their results by sending us a paired blood spot and plasma sample, and the results showed very good agreement between the two sample types and methodologies (Figure 1).
Relationship between paired plasma and blood spot samples for measurement of 25-hydroxyvitamin D.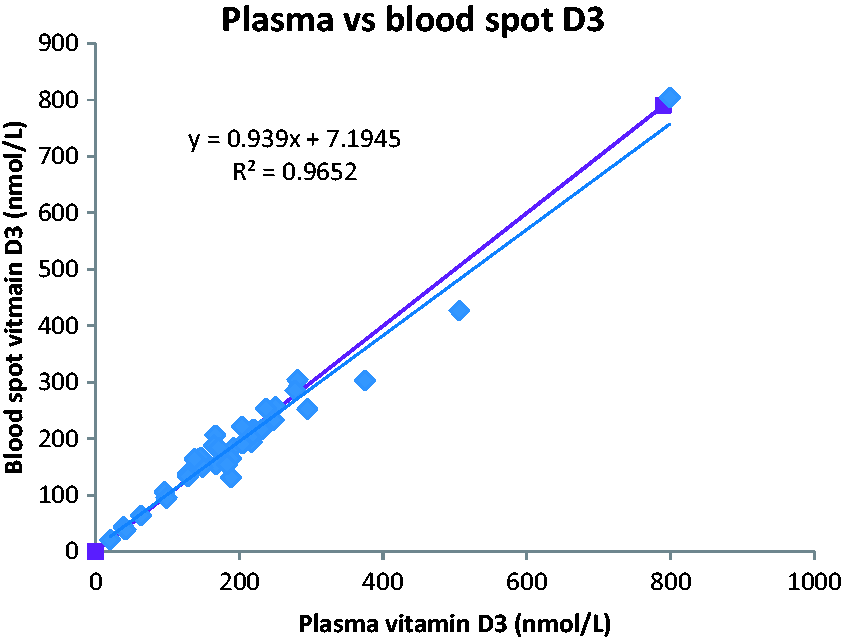
We had previously received a dried blood spot from 153 of the users who were found to have a 25-hydroxyvitamin D concentration >220 nmol/L when using the direct to the public service. The majority (n = 109; 71%) had received a previous adequate result, ranging from 50 nmol/L to 217 nmol/L. The people who had previously been deemed less than adequate had results ranging from 11 nmol/L to 49 nmol/L.
Supplementation patterns
Of the 372 users who had results >220 nmol/L, three could not be contacted and five did not wish to discuss their results. The data from the remaining 364 users are discussed below.
Daily supplementation
Daily supplementation patterns in users who achieved a 25-hydroxyvitamin D result >220 nmol/L and who could recall how much they were supplementing with and the range of concentrations found with those supplementation rates.
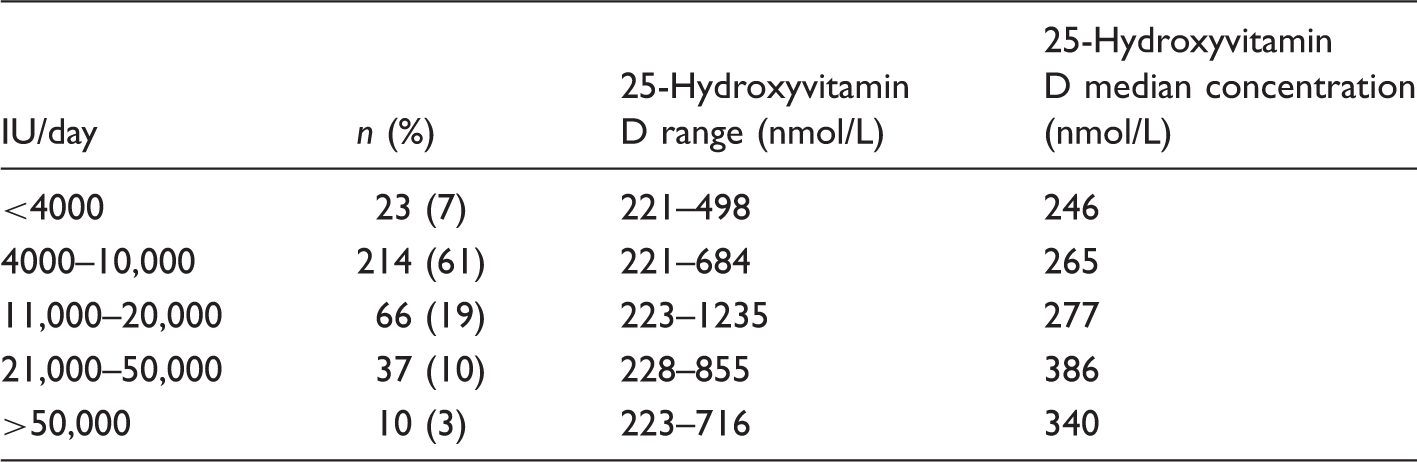
There were 14 users of the dried blood spot service who were aged 16 years or less and who achieved a high 25-hydroxyvitamin D concentration in the time frame. One user’s mother was unable to recall the amount she was supplementing her child with and another did not wish to discuss the results. For the rest of the children, supplements taken ranged from 1000 to 5000 IU/day and 25-hydroxyvitamin D concentrations ranged from 221 to 498 nmol/L. None of the children were under medical supervision.
Some users also stated that they had recently been on holiday/sunbathing/using sun beds near the time they took the test.
Brand
Of the 363 users who had taken supplements, 292 (80%) gave a brand when asked. Nine brands could not be verified and in five cases the website that the supplements were obtained from were stated as the brand even though these websites did not manufacture vitamin D supplements. The remaining 278 members of the public used a total of 55 different brands with the most popular being Healthy Origins with 77 (27.7%) people using it. Solgar, Credence and Nutri Advanced were other popular brands with >5% of people with high results taking them.
Formulation
The range of formulations described by 342 members of the public covered capsules (including gel capsules and soft gels), drops, powder, spray, under tongue lozenge and tablets. There were 21 users who did not state what formulation their supplements came in. The most popular formulation was capsule with 200 (58.5%) people taking their supplements in this form.
Where the supplements were sourced
The source the supplements were obtained from could be recalled by 337 users. The most popular route for obtaining supplements was via the internet (248 users, 74%). Other sources included health shops, healthcare practitioners, pharmacies and shops.
Length of time supplemented for
Many people could only give rough estimates for how long they had supplemented for. A total of 345 people gave a figure, including the two who took bolus doses. Some people only started supplementing after receiving a 25-hydroxyvitamin D result from their GP or our service.
The supplementation time in the 345 users varied from eight days to ‘years’. One person stated that they had been taking 5700 IU/day for 10 years and their 25-hydroxyvitamin D was 360.5 nmol/L. The user who supplemented for the shortest stated time of eight days had taken 50,000 IU every day, resulting in a 25-hydroxyvitamin D concentration of 238.1 nmol/L. Another user who had been supplementing for 10 days had a 25-hydroxyvitamin D concentration of 450.2 nmol/L having supplemented with 20,000 IU/day because they were ‘experimenting’. Another user had a ‘tingling forehead’ and so took 26,000 IU/day for 12 days which resulted in a 25-hydroxyvitamin D concentration of 284 nmol/L. The user with the highest daily supplementation rate took 120,000 IU a day for one month, resulting in a concentration of 715.5 nmol/L. The member of the public with the highest concentration seen of 1234.6 nmol/L had been most recently supplementing with 20,000 IU/day for nine months and prior to that had been taking 40,000 IU/day for four to five months.
Extent of medical supervision
Out of the 361 users who were taking regular supplementation, only 23 (6.3%) were under medical supervision. Of the 28 users whose results were >500 nmol/L, only one was under medical supervision. Just seven (6.2%) users out of the 113 taking >10,000 IU/day were under medical supervision. There were 14 patients who had started supplementing on the advice of a GP after having a previous low 25-hydroxyvitamin D result. Two of these patients had a falsely low 25-hydroxyvitamin D measured by their local lab (one NHS laboratory in the UK, one in the Czech Republic) and were prescribed high-dose supplementation by their GP. When the sample was retested by a mass spectrometric method, the patients were actually found to have toxic concentrations. Another member of the public was prescribed Osteofos for their osteoporosis, and their dietician had then added in vitamin D drops of 4000 IU/day. Six other patients had an initial prescription from the GP, which they then topped up with over-the-counter supplements. One person was taking at least 50,000 IU/day (often up to 100,000 IU) against the advice of their medical consultant.
Reasons for supplementation
Reasons why members of the public using our direct to the public vitamin D blood spot testing service decide to take vitamin D supplements.
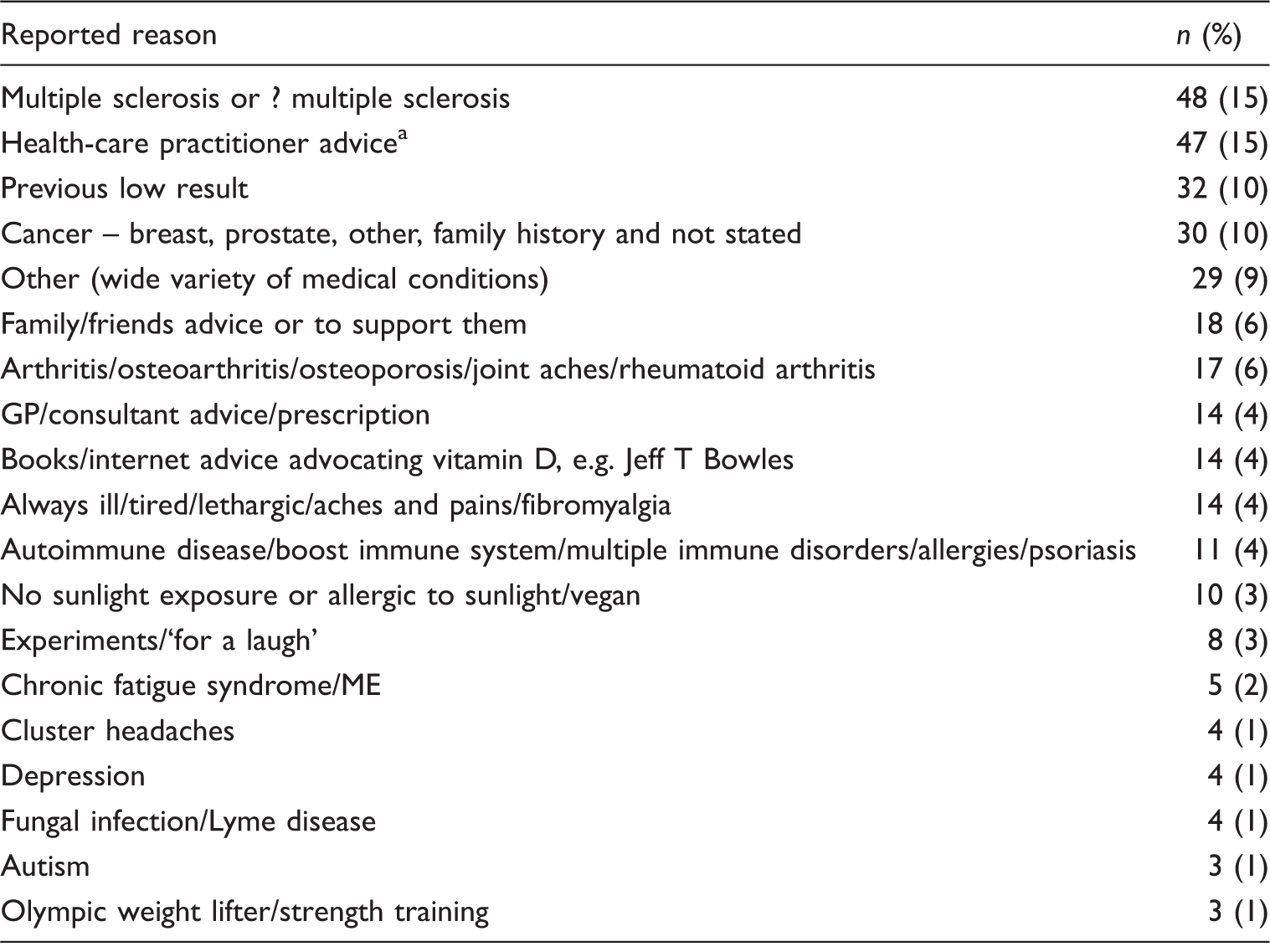
Health-care practitioner covers osteopath, nutritionist, dietician.
Although not directly asked, many people with severe diseases reported that their conditions had improved after they had started taking vitamin D supplements, while other people felt that there had not been any improvement. Many people (n = 45) stated that they were co-administering vitamin K2 as they had read or been told that taking vitamin K2 would minimize any side-effects, namely hypercalcaemia, caused by taking high doses of vitamin D. Often people remarked that they were also taking other supplements as well and in particular magnesium.
Several people wanted to tell us that they felt our NHS reference ranges were inappropriate, and some had disease-specific reference ranges that they were aiming for. For example, some patients with multiple sclerosis were following the ‘overcoming multiple sclerosis programme’ (http://www.overcomingmultiplesclerosis.org), which recommends aiming for a 25-hydroxyvitamin D concentration of 150–225 nmol/L.
Many of the people questioned were remarkably knowledgeable about vitamin D and often informed by websites. Some people felt very frustrated by the apparent lack of interest and importance placed on vitamin D by mainstream medical professionals, especially when many of them felt they had benefited from taking vitamin D.
Discussion
The prevalence of 25-hydroxyvitamin D results >220 nmol/L, measured by blood spot, in the population studied here was 3.1%, compared with 0.06% in our GP population measured by tandem mass spectrometry. Most of these high results were <375 nmol/L. However, 8.6% were >500 nmol/L, a concentration considered to be potentially toxic.2,7,13,22,23 We have no other evidence of toxicity in these patients; neither serum nor urine calcium was measured. Only one of the users whose concentration was >500 nmol/L was under medical supervision.
In view of the close agreement we found between paired blood spot and plasma samples, we think that the high prevalence of results >220 nmol/L reflects a genuine rather than methodological difference. The two populations are distinct. The population we studied, of ‘direct service users’, gave varied reasons for taking vitamin D supplements. Some had multiple sclerosis and reported that they were following the ‘overcoming multiple sclerosis’ programme, 24 which encourages people to aim for 25–hydroxyvitmain D concentrations >150 nmol/L. Although many of these patients felt they had gained benefit from having an ‘adequate’ concentration of vitamin D, the use of vitamin D in the treatment of multiple sclerosis is controversial.25,26 An additional two users had taken large bolus doses of vitamin D (300,000 and 900,000 IU) without medical supervision. Similar cases have been reported previously.15,27–30
The population we have studied may be more representative of the general public than a population of patients tested by their GPs. However, it is self-selecting because users have chosen to monitor their vitamin D concentrations at a financial cost to themselves. This population may be more likely to take vitamin D than the general public because they have chosen to have their concentrations measured. Additionally, the findings presented here apply specifically to the users found to have high concentrations, not the wider pool of users where 25-hydroxyvitmain D was <220 nmol/L.
We cannot comment on the toxicity of the concentrations of 25-hydroxyvitamin D observed or the toxicity of the amount of vitamin D taken by our users. This is a limitation of our study and further studies focusing on toxicity are warranted.
The Institute of Medicine’s (IOM) 2011 report on vitamin D2 generated debate as to whether their ‘no observed adverse effects concentration’ (NOAEL) of 10,000 IU/day and upper intake concentration of 4000 IU/day was too low.21,31 The Endocrine Society published their own guidelines in 2011 4 recommending higher cut-offs for adequacy compared with the IOM report (75 nmol/L vs. 50 nmol/L, respectively) and recommending an upper intake concentration of up to 10,000 IU/day in some groups, not to be exceeded without medical supervision. However, we found that just under one-third of our high-level population were regularly taking more than 10,000 IU/day and only 6% of those were doing so under medical supervision.
Nearly half of subjects with high results had previous 25-hydroxyvitamin D blood spot measurements with us of which three-quarters had an adequate result. The finding of an adequate result on supplementation therefore does not guarantee that future results will remain within that range. This is not just the case for people taking above 10,000 IU/day – we found users taking as little as 1000 IU/day with high concentrations.
We found a number of children who had high concentrations of 25-hydroxyvitamin D. Of the 12 children in our study where the amount of vitamin D supplementation was reported, six were exceeding the IOM’s guidelines and two were exceeding the Endocrine Society’s guidelines, and none were under medical supervision. Variability in regimens may have contributed to the variable responses seen to the concentrations of vitamin D taken. Worryingly, two children were reported to be taking 1000 IU/day, well within both sets of recommendations, but nevertheless had concentrations >300 nmol/L (308.5 and 497.5 nmol/L). Paediatric patients have become hypercalcaemic after receiving vitamin D well within the accepted guidelines. 32 A recent review by Vogiatzi et al. 15 describes how many studies have been undertaken in children following a variety of vitamin D dosing regimens within the IOM or Endocrine Society’s guidelines, and the majority of those studies reported no documented harm although some subjects did attain high concentrations of 25-hydroxyvitamin D.
Most of our users obtained vitamin D independently of medical professionals by purchasing unlicensed products. LeBlanc et al. 33 found variable potency of unlicensed vitamin D, ranging from 9% to 146%, compared with that quoted by the manufacturer, as well as variable potency within-batches and between-batches. This problem has been highlighted elsewhere,34,35 and may help to explain some of the variability we observed in concentration of 25-hydroxyvitamin D even when users were reportedly taking similar amounts of vitamin D.
Importantly, our study demonstrates how some members of the public approach vitamin D supplementation. This is increasing17,36 and 70% of patients do not report the use of alternative treatments to their doctors. 27 Our finding of potentially toxic vitamin D concentrations in some subjects underlines the importance for clinicians to consider the use of vitamin D supplementation in the differential diagnosis of hypercalcaemia.
Footnotes
Declaration of conflicting interests
Both authors run a clinical service in the United Kingdom for vitamin D to the general public.
Funding
This study was supported by Sandwell & West Birmingham Hospital NHS Trust, Department of Clinical Biochemistry.
Ethical approval
This work details results produced in our normal clinical practice. All data presented have been anonymized and ethical approval was not required.
Guarantor
JB.
Contributorship
RS sand JB designed the studies. RS undertook the research and wrote the paper. JB and RS edited the manuscript.