
Abstract
Background
Calprotectin is an antimicrobial, calcium and zinc-binding heterocomplex protein and has been proposed as a marker to rule out inflammatory conditions. The aim of this study was to evaluate the role of calprotectin in the diagnosis of polycystic ovary syndrome and to investigate the association between calprotectin and insulin resistance.
Methods
A total of 41 females with polycystic ovary syndrome and 54 age-matched without polycystic ovary syndrome were eligible for the study. Serum concentration of calprotectin was determined using enzyme-linked immunosorbent assay. Clinical characteristics, hormone and metabolic parameters were evaluated in each subject. The predictive value of serum calprotectin was assessed using receiver operating characteristic curves. Correlations between the serum calprotectin concentrations and insulin resistance were examined using Spearman’s correlation.
Results
We found that the serum calprotectin concentrations were significantly higher in polycystic ovary syndrome compared with the non-polycystic ovary syndrome group (P < 0.001). The area under the receiver operating characteristic curve assay yielded a satisfactory result of 0.88 (95% confidence interval 0.81–0.95; P < 0.001). The optimum cut-off was 2.4 µg/mL with a 85.2% specificity and 75.6% sensitivity for polycystic ovary syndrome diagnosis. A significant positive correlation was found between the serum calprotectin and insulin resistance.
Conclusions
These results suggest that calprotectin might be a useful adjunct in the diagnosis of polycystic ovary syndrome, especially those with insulin resistance.
Introduction
Polycystic ovary syndrome (PCOS) is one of the most common endocrine abnormalities among premenopausal females, yet its diagnosis remains one of the most challenging issues in endocrinology and reproductive medicine. 1 It is a metabolic disorder characterized by a high percentage of cases by insulin resistance, which means that patients are at a high risk of developing type 2 diabetes or metabolic syndrome.2–4 There exist, however, no universal diagnostic criteria for PCOS; 5 consequently, the reported prevalence of the disease varies from 2.2 to 26% of premenopausal females. 6 The pathogenesis of PCOS remains largely unknown, but it has been attributed mainly to disordered folliculogenesis causing oligo-ovulatory cycles 7 or impaired folliculogenesis with increased preantral and small antral follicle counts, resulting in high anti-Müllerian hormone concentrations.8,9 Therefore, there is a need for independent or supplementary biomarkers for PCOS.
Calprotectin, also called S100A8/S100A9, is a newly identified calcium-binding protein, closely correlated with inflammation 10 that originates from neutrophils and macrophages. It has various biological functions, including suppression of cell proliferation, apoptosis induction, immune regulation and participation in inflammatory reactions.11–13 Interestingly, it has been reported that calprotectin is secreted during degranulation and can be found in the maternal serum. It is abundant in the cytosol of neutrophils and can also be found in lower concentrations in monocytes, tissue macrophages and eosinophils.14,15 Calprotectin is a factor which blocks the intake of metal ions (zinc, manganese and iron), essential for the proliferation of pathogens. 16 Feng et al. 17 found that the placental expression of calprotectin was increased near the end of the third trimester of pregnancy, and they attributed this effect to endothelial damaged by tissue hypoxia. Recently, it has been demonstrated that serum calprotectin is increased in patients with papillary thyroid carcinoma 18 and in neuroinflammation in diabetic peripheral neuropathy. 19 However, the role of calprotectin in the pathogenesis of PCOS is still incompletely understood.
In the current study, we evaluated the role of calprotectin as a diagnostic marker for PCOS. We also investigated serum calprotectin concentrations in relation to insulin resistance in PCOS.
Materials and methods
Study population
In total, 41 females with newly diagnosed PCOS and 54 healthy individuals aged 18–45 were consecutively enrolled from the outpatients of Obstetrics and Gynecology Hospital of Fudan University, China, between April 2013 and December 2014. Healthy individuals without PCOS acted as the control group; none showed any signs of infection or infectious diseases, and none were pregnant. We made further subgroupings based on the presence of insulin resistance defined as a homeostasis model assessment (HOMA) index of ≥2.4. 20 All the subjects included in the study had no medical history or evidence of diabetes, hypertension, hyperprolactinemia, thyroid disease, Cushing’s syndrome or congenital adrenal hyperplasia. Subjects taking drugs such as insulin-sensitizing drugs, oral contraceptives, corticosteroids, anti-androgens and gonadotropin-releasing hormone agonists or antagonists were excluded from the study. Subjects without a menstrual cycle were also excluded. Before enrolment, all subjects provided written informed consent. This study was approved by The Ethics Committee and Institutional Review Board of Obstetrics and Gynecology Hospital of Fudan University, China (Protocol number 52/10).
Polycystic ovarian syndrome was diagnosed according to the criteria developed by the PCOS Consensus Workshop Group in 2003 as follows. 21 (1) Polycystic ovaries identified by ultrasound (≥12 small follicles with the diameter of 2–9 mm in at least on ovary, and/or ovary volume >10 mL. (2) Clinical or biochemical evidence of excessive testosterone (testosterone ≥2.55 nmol/L). (3) Anovulatory menstrual disorder. Two of above criteria with exclusion of other causes were sufficient to diagnose PCOS.
Biochemical analyses and hormone assays
A double-blind procedure is used in this study. A detailed clinical history was taken, and physical examination was performed for all participants. Body mass index (BMI) was also calculated. Routine laboratory investigations included fasting serum glucose and insulin, luteinizing hormone (LH), follicle-stimulating hormone (FSH), dehydroepiandrosterone sulfate (DHEAS) and sex hormone-binding globulin (SHBG) concentrations. Insulin resistance was determined by the HOMA index (=fasting glucose (mg/dL) × fasting insulin (μU/mL)/405). 22 All sampling procedures were performed in the early follicular phase (days 2–5 of the menstrual cycle) in the morning after an overnight fast for 12 h. The concentrations of serum calprotectin were assessed using the enzyme-linked immunosorbent assay (ELISA). The human calprotectin ELISA kit was obtained from Shanghai Langka Co., Ltd (Shanghai, China). Assay procedures were done as per manufacturer’s instructions. The intra- and inter-assay coefficients of variation were <8% and <10%, respectively. The linear range for calprotectin was 0.1–100 µg/mL.
Statistical analysis
Data are presented as mean ± SD unless otherwise indicated and was analysed by Student t test. Serum calprotectin concentrations were used to draw receiver operating characteristic (ROC) curves (medclac v9.2.0.1; Belgium), and the specificity, sensitivity and area under the ROC curve (AUC) were determined. The AUCs were used to estimate model performance. Correlation analysis was performed using Spearman’s correlation coefficient by rank. A P value < 0.05 was considered statistically significant. All statistical analyses were performed using Prism version 5 (GraphPad Software, Inc.).
Results
Demographic, clinical and biochemical characteristics
Main clinical and hormonal features in females with PCOS and in females without PCOS.
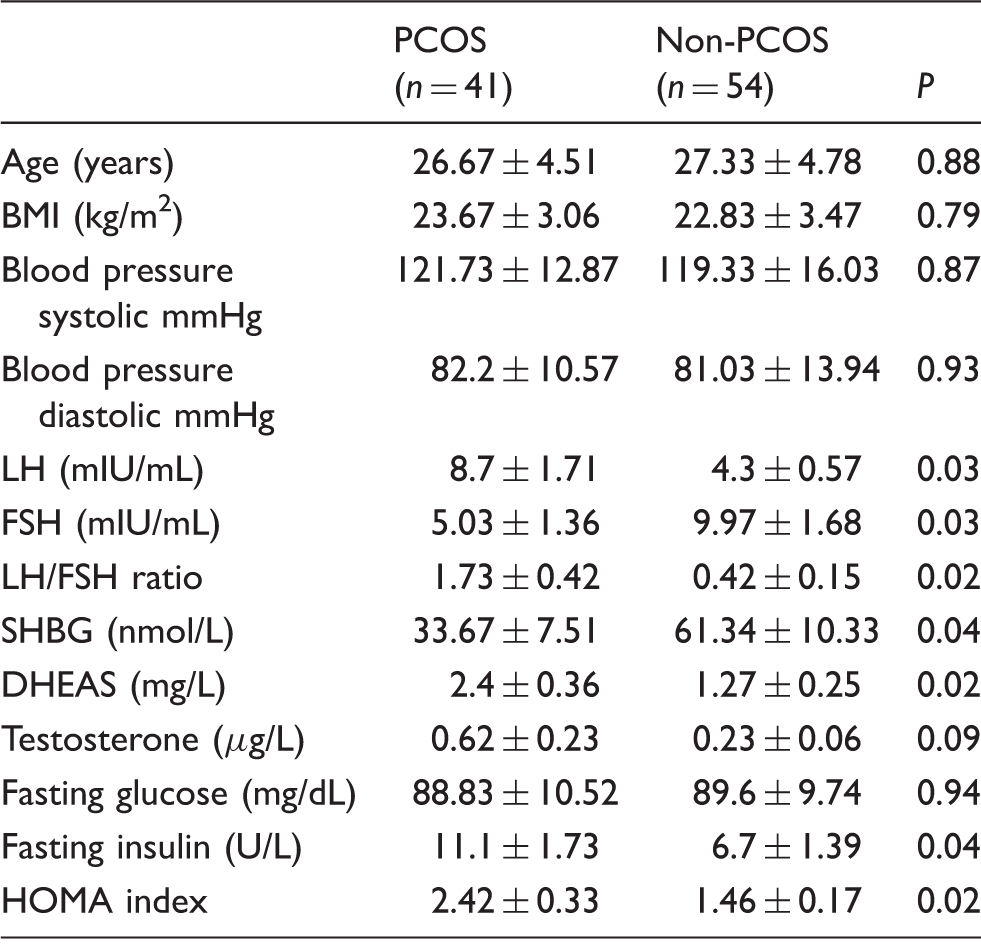
Note: Results are average ± SD.
BMI: body mass index; LH: luteinizing hormone; FSH: follicle-stimulating hormone; DHEAS: dehydroepiandrosterone sulfate; SHBG: sex hormone-binding globulin; HOMA index: homeostasis model assessment (HOMA) index.
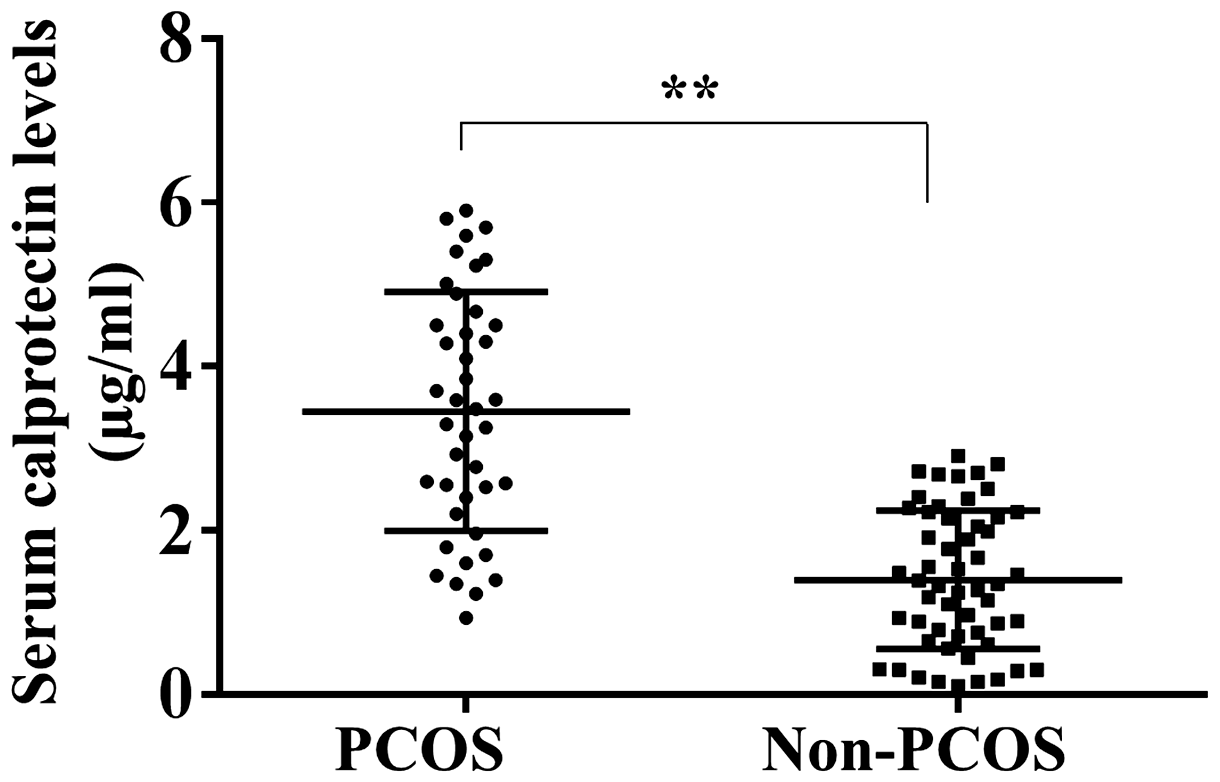
Serum calprotectin concentration in PCOS and non-PCOS groups. Calprotectin concentrations were measured in serum from patients with PCOS (n = 41) and without PCOS (n = 54). Data are presented as mean ± SD. **, P < 0.01.
ROC analysis of calprotectin values in PCOS and controls
The value of calprotectin in the identification of patients with PCOS was analysed using ROC analysis. The ROC curve of the serum calprotectin concentrations for discriminating PCOS from controls is shown in Figure 2. The area under the ROC curve yielded a satisfactory result of 0.88 (95% confidence interval, 0.81–0.95; P < 0.001). The best compromise between specificity (85.2%) and sensitivity (75.6%) for a PCOS diagnosis was obtained with a cut-off value of 2.4 µg/mL.
ROC curve for evaluating the diagnostic role of calprotectin on PCOS. Serum calprotectin concentrations in PCOS and non-PCOS were used to draw ROC curve, and the specificity, sensitivity and AUC were determined.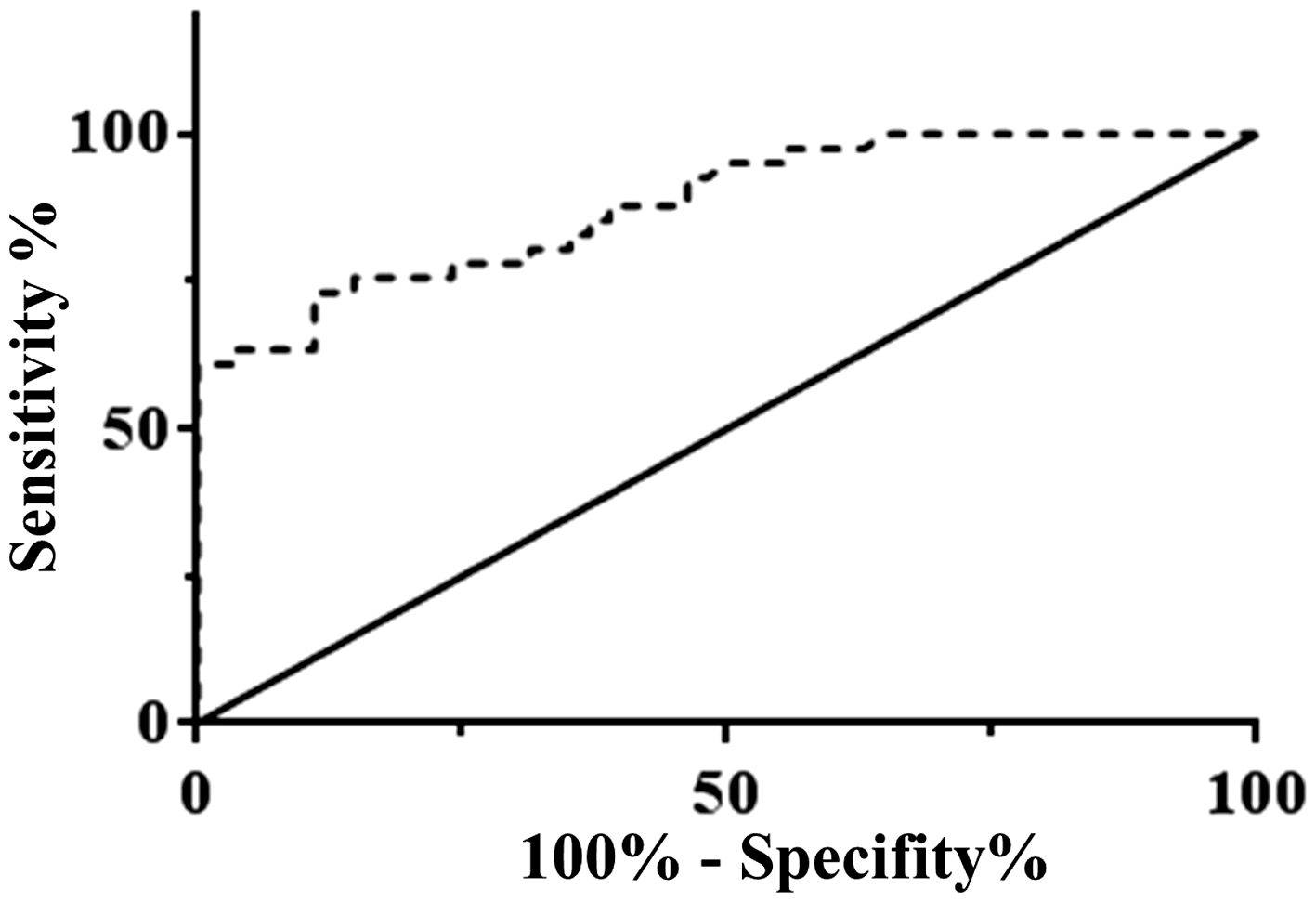
Calprotectin concentrations is associated with insulin resistance
A biomarker should have a significant relationship to clinical symptoms. Since insulin resistance is an important feature of PCOS, we further evaluated whether serum calprotectin concentrations correlated with insulin resistance. We found a significant higher calprotectin concentration in PCOS patients with (n = 23) insulin resistance than PCOS patients without IR (n = 18) (P < 0.001) (Figure 3(a)). Moreover, we analysed the correlation between the HOMA index and the serum concentrations of calprotectin in PCOS patients. A significant positive correlation between the HOMA index and the concentrations of calprotectin (γ = 0.89, P < 0.01) was found (Figure 3(b)).
The relationship between serum calprotectin concentrations and insulin resistance. Calprotectin concentrations in PCOS patients classified according to insulin resistance. (a) Median serum calprotectin concentrations in PCOS patients with (n = 23) or without IR (n = 18). (b) The correlations between HOMA index and the concentrations of calprotectin in PCOS patients with IR were examined using Spearman’s correlation coefficient by rank. Data are presented as the mean ± SD. **P < 0.01.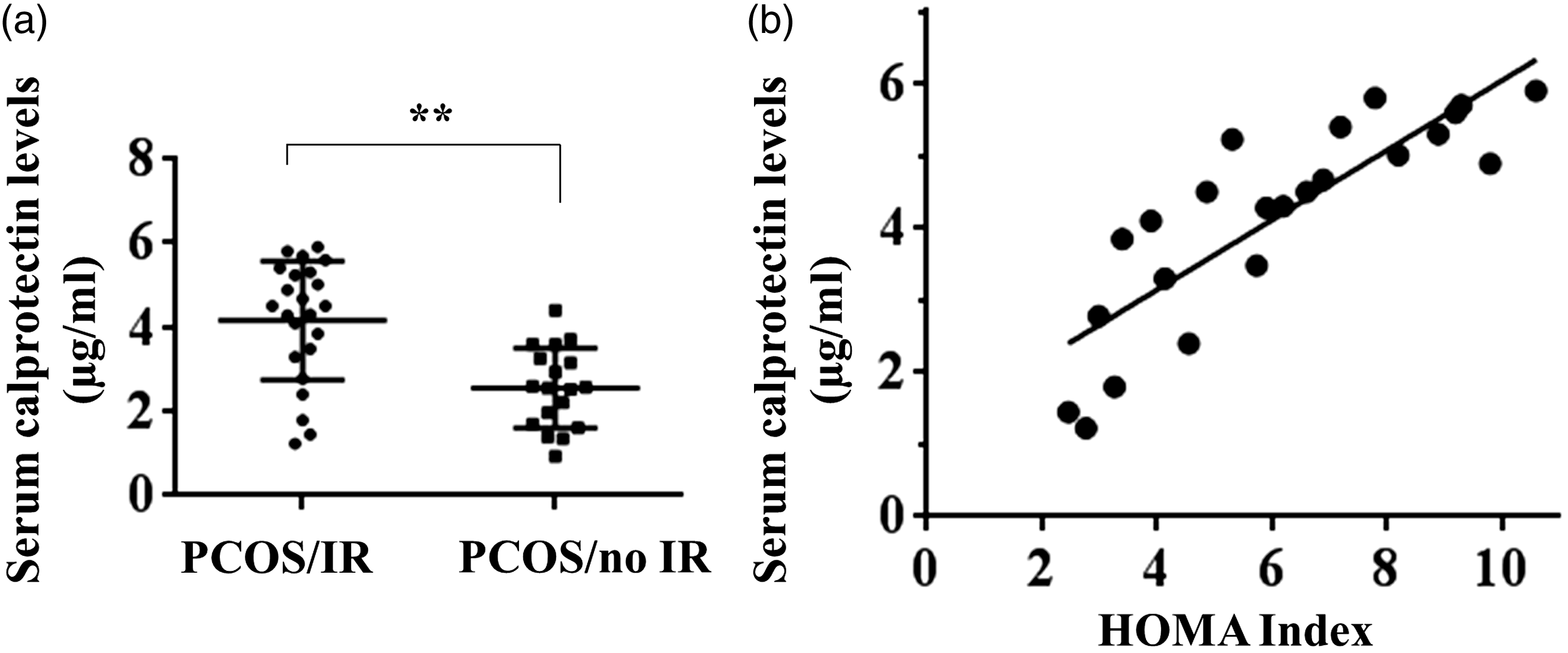
Discussion
In this study, we reported for the first time, to our knowledge, that serum calprotectin concentration might be a useful adjunct in the diagnosis of PCOS with good sensitivity and specificity. Another important observation in the present study was that calprotectin concentrations correlated with insulin resistance in PCOS patients.
It has been reported that calprotectin may be considered a promising early, sensitive and specific marker of sepsis. 23 In addition, Decembrino et al. 23 demonstrated that serum calprotectin concentrations are significantly higher in patients with and without neuropathy than healthy controls, suggesting that calprotectin may be a novel biomarker of neuroinflammation in diabetic peripheral neuropathy. 19 It has also been shown that serum calprotectin concentrations are increased in patients with papillary thyroid carcinoma, and the marker is positively correlated with total oxidant status and lipid hydroperoxide. 18 All these findings indicated that calprotectin could be a biomarker of a number of disease states. Interestingly, one study reported a significant increase in serum calprotectin in females with ovarian and uterine cancer, suggesting the involvement of an inflammatory process. 24 In agreement with previous results, we found that serum calprotectin was significantly elevated in the females with PCOS compared with non-PCOS controls. Since the inflammatory process is reported to be correlated with PCOS,25,26 it is reasonable to predict that elevated calprotectin might also be involved in this process. Indeed, accumulating data have demonstrated that calprotectin is present during the inflammatory response, and calprotectin measurements in stool and serum may provide a promising strategy to identify patients with spondyloarthritis at risk of bowel inflammation.27,28 Neutrophils are capable of controlling microbial infections via phagocytosis and production of antimicrobial factors. 29 It has been documented that calprotectin comprises about 50% of the neutrophil’s cytoplasmic protein content and is a critical component of the host nutrient withholding process termed nutritional immunity.13,30,31 Thus, the up-regulation of calprotectin in PCOS may be caused by the inflammatory response. Further, ROC curve analysis showed that serum calprotectin had a certain capability in predicting PCOS. These findings suggested that calprotectin might be a useful adjunct in the diagnosis of PCOS.
Insulin resistance is a key feature of PCOS, and it plays a major role in the development of the hyperandrogenism characteristics of PCOS. 32 Beyond representing the most frequent cause of hyperandrogenism and female infertility, PCOS puts young females at increased risks of diabetes and cardiovascular diseases. Conversion from normal glucose tolerance to abnormal glucose tolerance and from abnormal glucose tolerance to type 2 diabetes mellitus is increased two- to five-fold in the PCOS population.33,34 It is important to determine the insulin resistance status of females with and without PCOS, because it will influence the choice of treatment. In this study, we were able to analyse the prevalence of insulin resistance based on HOMA index in both the PCOS and the non-PCOS groups. In this way, it was shown that calprotectin concentrations were associated with insulin resistance in PCOS patients. As far as we know, this study is the first to determine the association of calprotectin with PCOS. Taken together, calprotectin might be a potential marker to identify PCOS with insulin resistance.
Our study is associated with a number of limitations. These findings are marker dependent, not assay dependent, and additional markers are needed to achieve clinical utility. Another limitation of our study was its cross-sectional design, which can be conducted as a prospective study on long-term effects of calprotectin in PCOS. Thus, large prospective longitudinal studies, ideally involving many ethnic groups, are needed to improve our understanding of the long-term health risks associated with PCOS.
In conclusion, we showed that serum calprotectin concentrations were significantly higher in the PCOS group compared with non-PCOS group. Our study suggested that serum calprotectin might be a useful adjunct in the diagnosis of PCOS and is associated with insulin resistance. These findings should be considered as preliminary, and prospective larger studies should be carried out to confirm these results.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
This work was supported by Health and Family Planning Scientific Research Project of Hubei Province (grant no. WJ2015MB207); Hubei Province Natural Science Fund Project (grant no. 2015CFC827).
Ethical approval
This study was approved by The Ethics Committee and Institutional Review Board of Obstetrics and Gynecology Hospital of Fudan University, China (Protocol number 52/10).
Guarantor
MJ.
Contributorship
SC, TD, JW, and PL did the experiments. SC and MJ designed the study and wrote the manuscript. All authors reviewed and edited the manuscript and approved the final version of the manuscript.