
Abstract
Background and Aims
Serum zinc, copper and selenium are measured in patients prior to commencing on parenteral nutrition; however, their interpretation can be difficult due to acute phase reactions. We assessed (i) the relationship of raised C-reactive protein with trace elements and albumin (ii) benefits of measuring trace elements when C-reactive protein is raised in patients requiring short-term parenteral nutrition.
Methods
Samples were collected for zinc, copper, selenium and albumin at baseline and then every two weeks and correlated with C-reactive protein results in patients on parenteral nutrition. Results were categorized into four groups based on the C-reactive protein concentrations: (i) <20 mg/L, (ii) 20–39 mg/L, (iii) 40–79 mg/L and (iv) ≥80 mg/L.
Results
In 166 patients, zinc, selenium and albumin correlated (Spearman’s) negatively with C-reactive protein; r = −0.26, P < 0.001 (95% CI −0.40 to −0.11), r = −0.44, P < 0.001 (−0.56 to −0.29) and r = −0.22 P = 0.005 (−0.36 to −0.07), respectively. Copper did not correlate with C-reactive protein (r = 0.09, P = 0.25 [−0.07 to 0.25]). Comparison of trace elements between the four groups showed no difference in zinc and copper (both P > 0.05), whereas selenium and albumin were lower in the group with C-reactive protein > 40 mg/L (P < 0.05).
Conclusion
In patients on short-term parenteral nutrition, measurement of C-reactive protein is essential when interpreting zinc and selenium but not copper results. Routine measurement of trace elements prior to commencing parenteral nutrition has to be considered on an individual basis in patients with inflammation.
Introduction
Parenteral nutrition (PN) is considered in patients when oral/enteral nutritional (EN) intake is inadequate or contraindicated. The biochemical monitoring of patients on PN in England and Wales is based on the recommendations in the National Institute for Health and Care Excellence (NICE) 2006 guidelines. 1 Zinc (Zn), copper (Cu) and selenium (Se) are essential trace elements (TE), and the biochemical evidence of deficiencies are common among patients on PN. 2 Hence, it is recommended that serum Zn, Cu and Se concentrations are measured at baseline and then every two to four weeks while on PN. 1
In blood, Zn is bound to albumin (around 80%), alpha-2 macroglobulin (20%), and a small amount present as amino acid complexes. 3 Zn is a component of many enzymes and protein structures and is essential for normal growth, metabolism, healing processes and immunity. 4 Concentrations of Zn may be increased by fasting and decreases after major surgery, acute phase response, steroid therapy and pregnancy. Zn shows diurnal variation (peak in the mornings) while also being dependent on albumin concentrations. 5 Zn deficiency may occur due to insufficient intakes or increased losses and also in patients on PN with inadequate supplementation. Marginal variations in serum Zn are therefore hard to interpret, although concentrations below 7–8 μmol/L usually indicate marked deficiency and may lead to skin disease and immunological defects.6,7 Other than by clinical assessment, there is no convenient way of assessing intracellular Zn status 8 and supplementing with high doses may reduce immune response. 7
Cu is a constituent of many oxidative enzymes and is raised during an acute phase response to trauma or infection, steroid therapy, certain tumours and pregnancy; it may be low because of dietary deficiency, PN administration, chronic liver disease or Wilson disease. 8 Cu deficiency may result in neutropenia, anaemia, skeletal abnormalities, reduced pigmentation of skin and hair and various neurological manifestations, 9 whereas high Cu concentrations are associated with liver toxicity. 10
Se is a component of selenocysteine, which has a role in antioxidant enzymes and metabolism. 11 Se deficiency may manifest as cardiomyopathy (Keshan syndrome), skeletal muscle myopathy,12,13 macrocytic anaemia 14 and abnormalities in nails and hair. 13 C-reactive protein (CRP) is used as an indicator of infection and inflammation.15,16 Serum albumin should not be considered as an indicator of nutritional status as it is affected by other factors including inflammation, hydration status, capillary permeability and hepatic failure. However, serum albumin concentration has been shown to be an indicator of morbidity and mortality. 16
Interpreting TE results can be challenging in hospitalized patients requiring PN since, the acute phase reaction may lead to a decrease in measurable serum total Zn, Se and albumin concentrations and an increase in Cu concentrations. 17 Measurement of CRP along with TE and albumin and plotting the trend may be helpful in interpretation. Moreover, the relatively long turnaround time may limit the value of TE measurement in patients on short-term PN. The aims of this study were to assess (i) the relationship between raised CRP with TE and albumin in patients on PN (ii) benefits of measuring TE when CRP is raised in patients requiring short-term PN.
Materials and methods
A total of 166 consecutive adult patients referred to the PN team were included. Indication for PN was either type 1 or 2 intestinal failure (IF). The study was approved by the local Clinical Effectiveness Committee (CASS AP 2977) and research ethics committee approval was not required. The data were collected retrospectively from electronic patient records and patients’ notes. Home PN patients were excluded as they are referred to regional IF centres from our institution and are not followed up by our PN team.
All the patients were monitored according to the NICE guidelines. 1 Baseline serum for CRP, albumin (SST tubes, BD Vacutainer®) Zn, Cu and Se (metal-free tubes, BD Vacutainer®) was collected simultaneously before starting PN. As recommended, CRP and albumin concentrations were monitored at baseline and two to three times a week until stable; Zn, Cu and Se concentrations were measured at baseline and then every two weeks depending on results and duration of PN administration. The Zn, Cu and Se contents in the PN bag were 100 µM, 20 µM, 0.4 µM, respectively (added as Additrace® [Fresenius Kabi UK]). The amount of Zn and Se in the PN bag can be increased to a total of 400 µM and 1 µM, respectively, or more as necessary depending on the blood test results. Cu cannot be increased further because of risk of precipitation in the bags.
CRP was measured turbidimetrically and albumin was measured using bromocresol green (BCG) on an Advia 2400 Chemistry analyser (Siemens Healthcare Diagnostics, Frimley, UK). Zn, Cu and Se were measured by inductively coupled plasma mass spectrometry (ThermoFisher Scientific, Series XII) in our supra-regional assay and advisory services designated laboratory for TE. Gallium (50 ppb) was used as the internal standard. Owing to potential interference from polyatomics (e.g. 66Zn + 12C) during Se (as 78Se) analysis, all three elements were simultaneously measured in the samples using collision cell technology which markedly improves measurement specificity. Limits of detection, based on analysing a set of tubes containing diluent only, were 0.2 µM, 0.04 µM and 0.03 µM for Zn, Cu and Se, respectively. IQC and EQA were acceptable throughout, the laboratory is CPA accredited.
Statistical analysis was performed using Analyse-It® (version 2.21, Leeds, UK) software. Normality of distribution was assessed using Shapiro–Wilk W test. A P < 0.05 was considered significant. All data are reported as median with interquartile ranges (IQR). Spearman’s rank test was used for correlation assessment. Baseline Zn, Cu, Se and albumin concentrations were categorized into four groups based on the CRP concentrations (i) <20 mg/L, (ii) 20–39 mg/L, (iii) 40–79 mg/L and (iv) ≥80 mg/L. Kruskal–Wallis ANOVA with pair-wise Mann-Whitney U test with Bonferroni correction were used to compare the four groups. The difference between baseline and day-15 TE concentrations was calculated. The changes in Zn, Cu and Se were correlated with a change in CRP.
Results
The study included 166 patients (72 females) aged 54 (41–67) years (median [IQR]). The duration of PN administration was 9 (6–16) days. The percentage of patients admitted as medical, elective surgical and non-elective surgical were 28, 24 and 48, respectively. In total, 62% were from intensive care units (ICUs) (25% medical, 75% surgical). Zn, Cu, Se, albumin and CRP were available in 160, 157, 144, 166 and 166 patients, respectively.
Scatter plots between CRP and baseline Zn, Cu and Se concentrations are shown (Figure 1). Baseline Zn, Se and albumin correlated negatively with CRP with Spearman r (r) = −0.26, P < 0.001 (95% CI −0.40 to −0.11), r = −0.44, P < 0.001 (95% CI −0.56 to −0.29) and r = −0.22, P = 0.005 (95% CI −0.36 to −0.07), respectively. Baseline Cu did not correlate with CRP where r was 0.09, P = 0.25 (95% CI −0.07 to 0.25).
(a) A scatter plot between C-reactive protein and baseline zinc concentrations (n = 160); (b) a scatter plot between C-reactive protein and baseline Copper concentrations (n = 157); (c) A scatter plot between C-reactive protein and baseline Selenium concentrations (n = 144).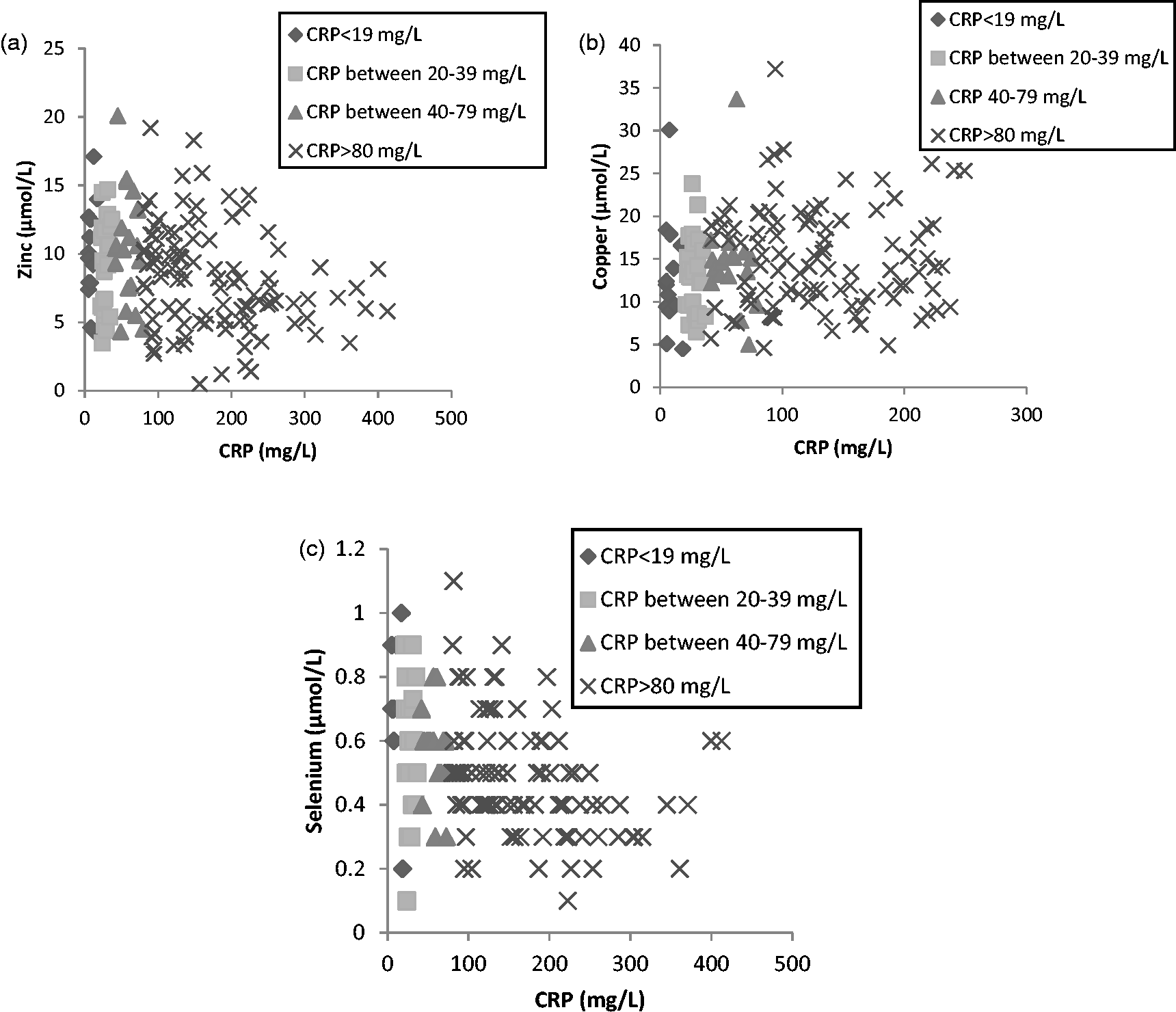
Four groups of baseline Zn, Cu, Se and albumin categorized on CRP concentrations.
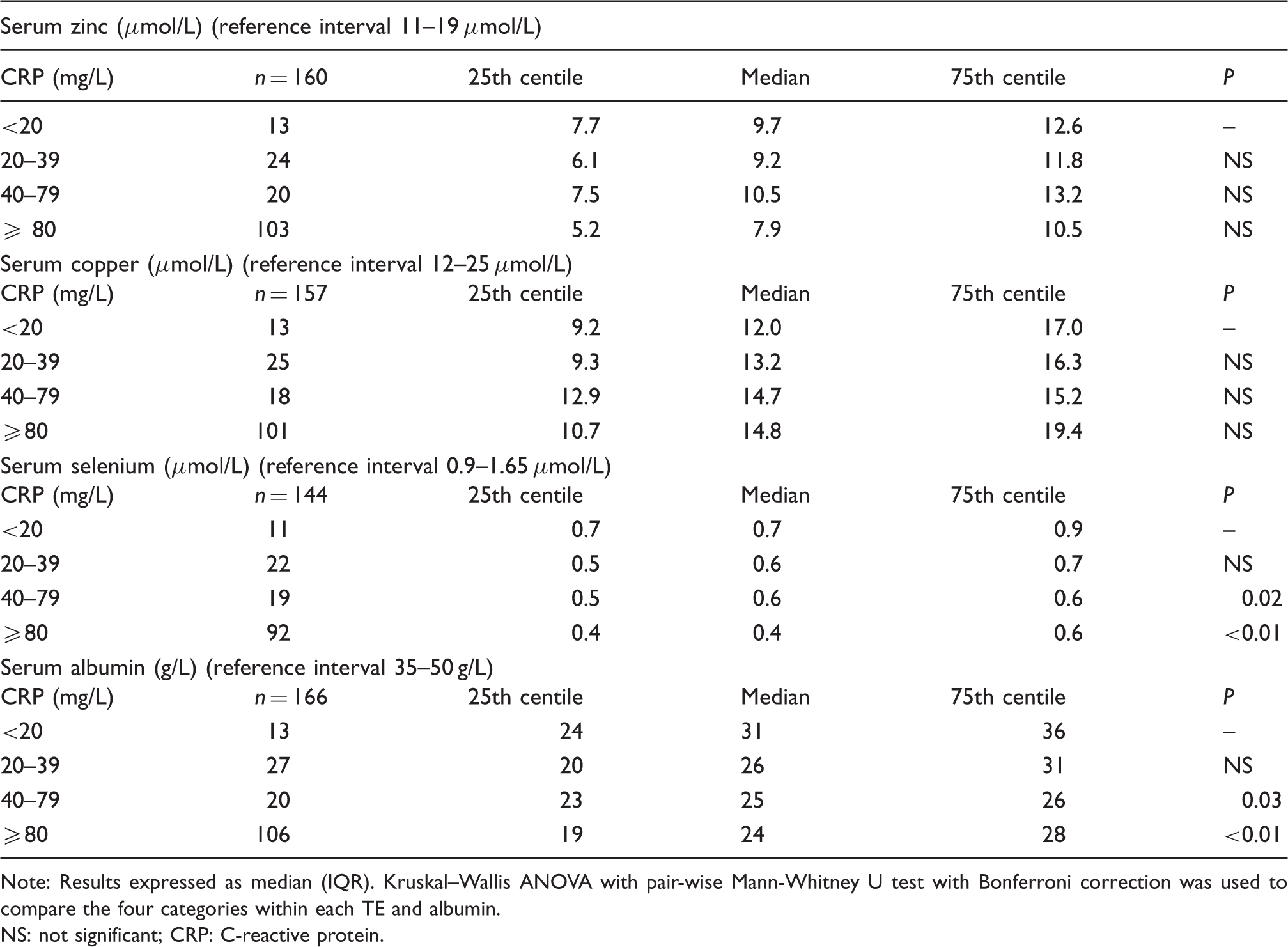
Note: Results expressed as median (IQR). Kruskal–Wallis ANOVA with pair-wise Mann-Whitney U test with Bonferroni correction was used to compare the four categories within each TE and albumin.
NS: not significant; CRP: C-reactive protein.
The study did not seek to correlate TE concentrations with specific clinical presentations and patients having higher requirements such as high-output fistulae, hemofiltration or dialysis.
Given the low number of patients (n = 47) on PN of greater than 14 days duration in our study, a repeat TE measurements was available only in a small proportion (n = 14) of the cohort. The difference between baseline and day-15 TE concentrations was calculated. The change in Zn and Se correlated negatively with change in CRP; r = −0.8727, P < 0.001 (95% CI −0.9679 to −0.5586) and r = −0.6886, P < 0.01 (95% CI −0.8965 to −0.2324), respectively. There was no correlation between changes in Cu and CRP.
Discussion
The relationship between TE and CRP is well documented, and we therefore focused on the clinical utility of TE measurement in hospitalized patients requiring short-term PN. Our study demonstrated lower concentrations of baseline Se and albumin with increasing CRP in patients before starting PN. Although baseline Zn concentration correlated negatively with CRP, there was no statistically significant difference in Zn concentration between the four groups defined on the basis of CRP concentration; this may reflect the small sample size. The change in Zn and Se in patients on PN over a period of 15 days correlated negatively with change in CRP. Baseline Cu concentrations (before starting PN) did not vary with CRP, and there was no correlation between change in Cu and CRP concentrations in patients on PN over 15 days. Our findings are in keeping with other reports including a recent study on TE and vitamin status which included patients with various clinical presentations.5,17
The interpretation of TE in patients on PN remains challenging. Most of our patients on PN were admitted for surgical procedures (72%) and nearly half of them had non-elective procedures, hence were likely to have higher CRP. Many medical patients were from ICU with high CRP. Moreover, inpatients especially postsurgery and from ICU may have variable fluid balance that changes frequently because of intravenous fluid infusion affecting albumin and other binding proteins. Previous data suggest that Zn and Se concentration fall by 40–50% following major surgery, whereas a rise in CRP to 20–30 mg/L leads to reduction in Zn and Se by 10%.5,18 Although Zn is bound to albumin, the fall in Zn concentration is much greater than the fall in albumin due to uptake of Zn into the liver. 19 Furthermore, intravenous Zn supplementation did not increase Zn concentration following surgery in one of the studies. 20 Forceville et al. 21 showed that the decrease in Se was proportional to the severity of inflammation in critically ill patients and hypothesized that it was due to Se uptake in the body tissues. Although our study did not show any significant change in Cu with a change in CRP, others have demonstrated an increase in serum Cu concentration following major trauma, surgery or infection, which was attributed to an increase in caeruloplasmin, a copper-binding protein. 22 Blood Zn, Se and Cu are poor indicators of their status in the body. 23 A previous report showed that only 6 out of 13 patients suspected of having micronutrient deficiencies clinically were confirmed on laboratory tests. 24
Albumin has a half-life of 14–20 days, hence is not sensitive to changes on a daily basis either because of nutrition or inflammation. As it is a negative acute phase reactant, it correlated negatively with CRP and was lower in the group with mortality within 30 days in our cohort which is similar to the findings in some studies that show patients with raised CRP along with low albumin for a period of time have poor prognosis. 25 Albumin measurement may be affected by inflammation status due to an increase in haptoglobin concentration that reacts with the BCG assay used in our study but not with modified bromocresol purple method. 26 Our study was limited by the majority of the patients being acutely ill and being on PN for a short duration (average of 15.7 days), which does not warrant multiple measurements of Zn, Cu and Se following supplementation. Second, none of the patients had CRP concentration within the healthy population reference interval (<5 mg/L). Nonetheless, the data presented here are representative of the patient cohort who are administered short-term PN in hospital. Studies on stable patients requiring longer term PN, i.e. home PN may inform better the benefit of routinely measuring and supplementing Zn, Cu and Se. Other limitations of our study include the lack of caeruloplasmin measurements to compare with changes in Cu concentration as well as not measuring prealbumin, which has been shown to be the better marker of nutritional status.27,28
The early supplementation of TE in patients presenting with burns or trauma and in severe sepsis has been shown to improve clinical outcomes (ICU survival, improve infectious complications and mortality) as well as shorten hospital stay and reduce costs. 10 Recently, Gagnon et al. 10 reviewed the quality and economic impact of TE monitoring in ICU. The study included those on TE supplementation with either EN (n = 166) or PN (n = 125). The authors demonstrated cost reduction in TE monitoring when done after day seven of TE supplementation. The European Society for Clinical Nutrition and Metabolism recommends that all PN prescriptions should include daily dose of TE to obtain a stable state, and it should be measured on a monthly basis in critically ill patients with prolonged hospital stay. 29 In our current clinical practice, TE measurement is requested in patients requiring PN only when the CRP is below 20 mg/L based on the recent study by Duncan et al. 17 In ICU patients, we routinely do not measure TE concentrations, but the PN prescriptions provide higher TE content than prescribed for the non-ICU patients. In our cohort, we calculate a saving of over £10,000 (based on a cost of approximately £60 for three TE measurements) by not measuring TE on patients with CRP ≥20 mg/L annually.
In conclusion, measurement of CRP is essential when interpreting Zn and Se results in patients on short-term PN. The routine measurement of TE prior to starting PN as proposed by NICE guidelines should be considered on an individual basis in patients with inflammation as the results may be difficult to interpret and have limited ability to inform TE supplementation doses especially in short-term PN.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
The study was approved by the King’s College Hospital Foundation Trust Clinical Effectiveness Committee (CASS AP 2977).
Guarantor
RPV.
Contributorship
Rashim Salota and Sohail Omar contributed equally to this manuscript .All authors have made substantial contributions to all of the following: (1) the conception and design of the study, or acquisition of data, or analysis and interpretation of data, (2) drafting the article or revising it critically for important intellectual content, (3) final approval of the version to be submitted.