
Abstract
Background
Enzyme matrix metalloproteinase-9 is a member of the matrix metalloproteinase family, which is critical to normal tissue remodelling during embryogenesis and wound healing. In patients with endometriosis, increased expression and activity of matrix metalloproteinase-9 have been observed in ectopic endometrium, but the plasma and peritoneal fluid concentrations of matrix metalloproteinase-9 in patients with endometriosis and their relation to disease severity have not been clear. The aim of the study was to investigate the concentrations of matrix metalloproteinase-9 in plasma and peritoneal fluid of patients with endometriosis.
Methods
A prospective case–control study was conducted in Jinan Military General Hospital between January 2010 and December 2013. Fifty patients with proven endometriosis and 26 endometriosis-free controls were enrolled in this study. Patients with endometriosis were evaluated and divided into moderate/severe endometriosis group (stage I–II, n = 26) and minimal/mild endometriosis group (stage III–IV, n = 24) according to the revised criteria of the American Society for Reproductive Medicine. Blood samples and peritoneal fluid were obtained from both patients and controls. Matrix metalloproteinase-9 was measured using enzyme-linked immunosorbent assay in plasma and peritoneal fluid. The concentration of matrix metalloproteinase-9 between different groups was compared and its correlation to disease severity was analysed.
Results
Plasma and peritoneal fluid concentrations of matrix metalloproteinase-9 in patients with endometriosis were higher than that in controls. In addition, those patients with moderate/severe endometriosis had significantly higher plasma and peritoneal fluid concentrations of matrix metalloproteinase-9 compared to those with minimal/mild endometriosis. Matrix metalloproteinase-9 concentrations in plasma and peritoneal fluid were both positively correlated with severity of endometriosis and plasma matrix metalloproteinase-9 concentrations had a positive correlation with peritoneal fluid matrix metalloproteinase-9 concentrations in patients with endometriosis.
Conclusions
Increased concentrations of plasma and peritoneal fluid concentrations of matrix metalloproteinase-9 appear to be associated with disease severity of endometriosis and may serve as an alternative biomarker to determine disease severity of endometriosis.
Introduction
Endometriosis is a common gynaecological disease characterized by ectopic presence of endometrial tissue (stroma and glands) outside the uterine cavity, which is estimated to affect about 5–10% of females of reproductive age.1,2 The most frequent sites of endometriosis involvement are the pelvic peritoneum and the ovaries. Common symptoms of females with endometriosis are chronic pelvic pain, dyspareunia and infertility. 1 Although endometriosis is designated a benign disorder, it has been gradually recognized that it has some characteristics similar to those of malignancies, such as the ability to invade and metastasize.3,4 Despite extensive research having been carried out, the exact cause of this disease still remains elusive.
So far, the preferred ‘gold standard’ method to diagnose endometriosis is laparoscopy; however, it is an invasive technique that requires general anaesthesia and may cause injury. As regards the diagnosis of retroperitoneal and deep infiltrating lesions, this technique is limited. 5 A promising non-surgical diagnostic approach is the use of pelvic magnetic resonance imaging (MRI), which can evaluate areas otherwise inaccessible by laparoscopy and detect deep pelvic endometriosis because of its multiplanar capacity and excellent tissue characterization. 6 But this method is also limited due to its high financial cost and low sensitivity and specificity. 7 Therefore, it would be attractive to have a new non-invasive method that can precisely reflect disease severity and progression for diagnosis in earlier time period of endometriosis.
Ectopic endometrial tissue formation is mediated by various factors which could facilitate cellular adhesion and infiltration, among which the matrix metalloproteinases (MMPs) are involved. Although MMPs are critical to normal tissue remodelling during embryogenesis and wound healing, aberrant expression of MMPs is associated with invasive and destructive diseases, playing a pivotal role in the destruction and turnover of the extracellular matrix (ECM). 8 In sites of endometriosis, the environment of ectopic endometrial growth contains a complex mixture of steroids and pro-inflammatory cytokines, which appear to affect MMP expression. 9 Numerous studies have demonstrated the altered expression of MMPs at ectopic sites and even in the eutopic endometrium of females with endometriosis 10 or in an animal model of endometriosis. 11 Increased expression and activity of MMPs, including MMP-9, have been observed in the ectopic endometrium. 12 While in those females without endometriosis, the expression of MMPs is lower. 13
Although several members of the MMP family have been described, MMP-9 has been most consistently detected in malignant tissues and is associated with tumour aggressiveness and metastatic potential.14–16 Chung et al. 16 demonstrated MMP-9 mRNA concentration in ectopic endometrium which was significantly higher when compared with eutopic endometrium from females with or without endometriosis. Li et al. 17 detected in both eutopic and ectopic endometrium of females with endometriosis, the expression of MMP-9 was significantly greater than that in the normal endometrium of healthy controls. All these studies suggest that MMP-9 may play an important role in the pathogenesis of endometriosis.
Extensive investigations in serum/plasma, urine, peritoneal fluid (PF) and/or follicular fluid (FF) biomarkers for endometriosis have been carried out in females with endometriosis, 18 including measurement of MMP-2 activity in FF and serum 19 ; however, there have been no detailed data on the association of circulating and PF concentrations of MMP-9 with disease severity of endometriosis thus far. The present study aimed to determine the MMP-9 concentrations in plasma and PF of females with endometriosis and to correlate concentrations of MMP-9 with severity of disease.
Patients and methods
Study population
This study was approved by the Ethics Review Committee of Jinan Military General Hospital and conducted in accordance with the Declaration of Helsinki. Written informed consent was obtained from all subjects before participating in the study. A total of 78 patients admitted to the Reproductive Medicine Centre of Jinan Military General Hospital were enrolled in the study between January 2010 and December 2013. Reasons for admission included diagnostic or therapeutic laparoscopy because of infertility, pelvic pain, suspected endometriosis, benign adnexal masses, leiomyoma uteri or ovarian cysts. Inclusion criteria were as follows: (1) reproductive age (18–45 years) with regular menstrual cycles (28–30 days), (2) no previous gynaecological operations and (3) absence of any endocrine, chronic autoimmune diseases and cardiovascular diseases. Exclusion criteria were as follows: (1) evidence of postmenopausal follicle-stimulating hormone (FSH) concentrations, (2) pregnancy, (3) suspicion of malignant disease, (4) presence of any non-endometriotic cyst, (5) history of oral contraceptive use, any other hormone therapy or operation within previous six months and (6) any other condition known to influence MMP-9 concentration (smoking, high alcohol intake, elicit drugs and known infections).Two patients were excluded due to diagnosis of serous cystadenoma. Seventy-six remaining patients were recruited for the study.
Among the 76 patients, 50 were confirmed with pelvic endometriosis by the existence of visible peritoneal endometriotic lesions and were designated group A. Twenty-six patients without any signs of endometriosis presented at laparoscopy were designated group B (recruited as controls). For the 50 females with proven endometriosis (group A), the extent and stage were further evaluated according to the revised criteria of the American Society for Reproductive Medicine (ASRM) 20 and thereby divided into two subgroups: minimal/mild endometriosis (stage I–II) group (n = 26) and moderate/severe endometriosis (stage III–IV) group (n = 24). General information such as age, body mass index (BMI), gravidity, parity, existence and duration of infertility and existence of dysmenorrhoea were collected and evaluated.
Laboratory methods
Venous blood samples were collected into heparin tubes from all patients before induction of anaesthesia for laparoscopy procedure. The blood samples were centrifuged to remove cells debris, and the plasma was stored at −20℃ until measurement. In addition, the PF samples were collected from pelvis before any manipulation. Any blood contaminated fluids were excluded. The PF samples were centrifuged, and the supernatant was stored at −20℃ until utilized. Quantitative measurement of plasma and PF MMP-9 was analysed with a commercially available enzyme-linked immunosorbent assay (ELISA) kit (Quantikine, R&D Systems, Minneapolis, MN, USA) according to manufacturer’s instructions. The manufacturer-reported precision was 1.9–2.9% for intraassay coefficient of variation (CV) and 6.9–7.9% for interassay CV. The sensitivity (minimum detectable concentration) of the assay was 0.156 ng/mL. The ELISA was conducted using an Infinite M200 PRO automated microplate reader at wavelength of 540 nm (Tecan Group Ltd., Männedorf, Switzerland).
Statistical analysis
Statistical analysis was performed using Statistical Package for Social Sciences (SPSS) software, version 16.0 for Windows. Data are presented as mean ± standard deviation (SD), median (interquartile range) or n when appropriate. Kolmogorov-Smirnov test was performed to analyse the data normality; unpaired t test or Mann-Whitney U test was used to assess significance in clinical characteristics between endometriosis patients and controls, as appropriate. Differences between plasma and PF MMP-9 concentrations in patients with stages I–II and III–IV were compared using unpaired t test. Differences between MMP-9 concentrations in plasma and PF were analysed using the Wilcoxon signed-rank test for paired samples. Spearman’s rank correlation was used to determine the correlation among the concentration of MMP-9 in plasma and PF and endometriosis severity. Multinomial logistic analysis was used to assess the independent predictors of endometriosis severity. P < 0.05 (α = 0.05) was considered statistically significant for differences and correlations. Test power (1 − β) was calculated with the formula
Results
Baseline characteristics of the study groups
The baseline clinical parameters of endometriosis patients and controls.
Concentrations of plasma and PF MMP-9 in patients with endometriosis
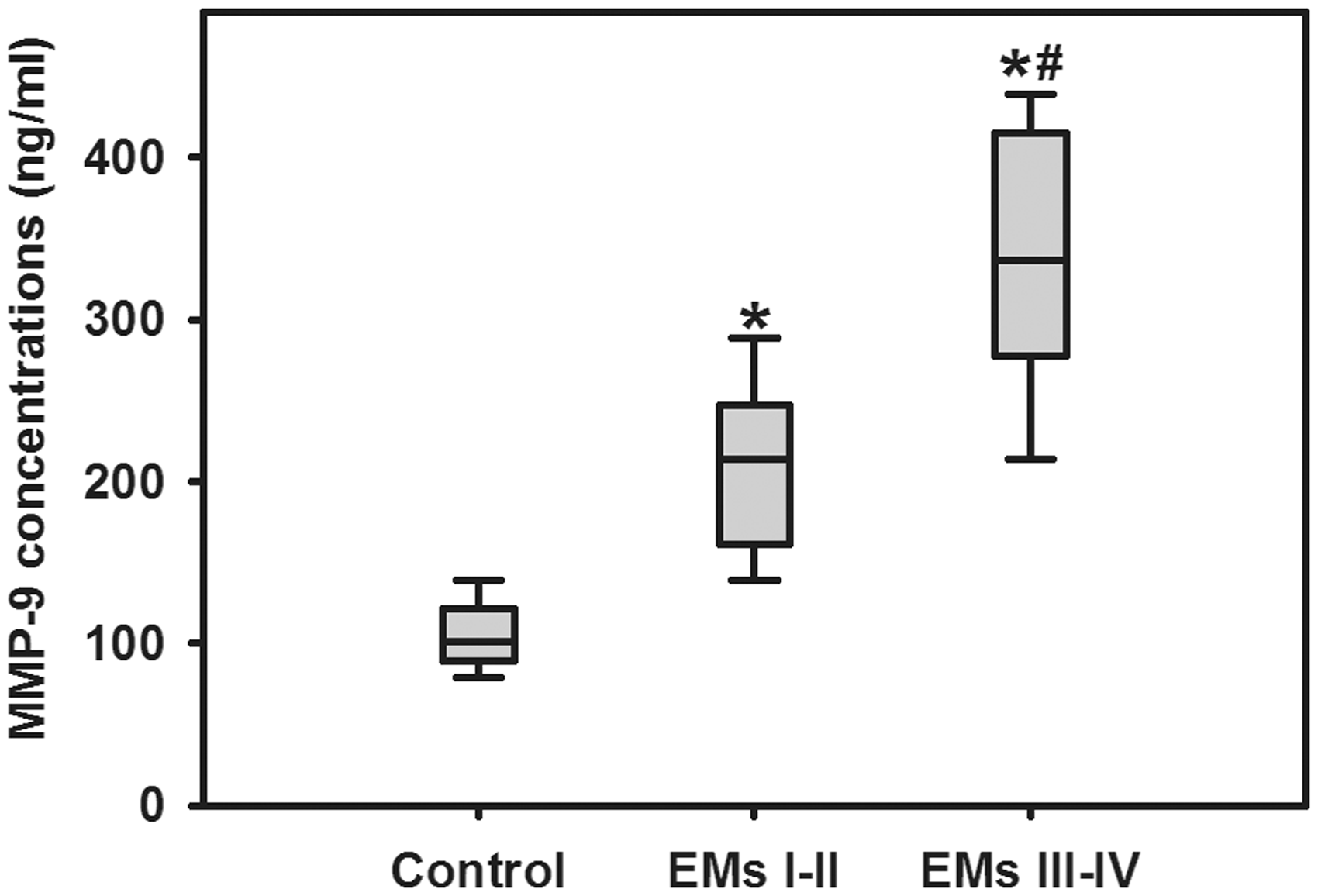
Concentrations of MMP-9 in plasma of endometriosis and control groups are illustrated in Figure 1. Significantly higher plasma MMP-9 concentrations were detected in moderate/severe endometriosis group compared to minimal/mild endometriosis (74.9 ± 18.1 vs. 37.7 ± 10.6 ng/mL; P < 0.01) and non-endometriosis controls (74.9 ± 18.1 vs. 12.2 ± 6.1 ng/mL; P < 0.01), and the average plasma MMP-9 concentrations in minimal/mild endometriosis females were also higher than that of controls (37.7 ± 10.6 vs. 12.2 ± 6.1 ng/mL; P < 0.01). MMP-9 concentrations in PF of non-endometriosis controls and endometriosis at different stages are shown in Figure 2. MMP-9 concentrations were 211.4 ± 52.1 ng/mL in females with minimal/mild endometriosis vs. 332.1 ± 78.9 ng/mL in those with moderate/severe endometriosis (P < 0.01) and 107.1 ± 20.7 ng/mL in non-endometriosis controls (P < 0.01). The average PF MMP-9 concentrations in minimal/mild endometriosis were also greater than that of controls (P < 0.01). Additionally, MMP-9 concentrations in PF were substantially higher than that in paired plasma samples (P < 0.01).
Enzyme matrix metalloproteinase (MMP)-9 concentrations in the plasma of patients with minimal/mild endometriosis (EMs I–II), moderate/severe endometriosis (EMs III–IV) and non-endometriosis (control). Enzyme matrix metalloproteinase (MMP)-9 concentrations in the peritoneal fluid (PF) of patients with minimal/mild endometriosis (EMs I–II), moderate/severe endometriosis (EMs III–IV), and non-endometriosis (control).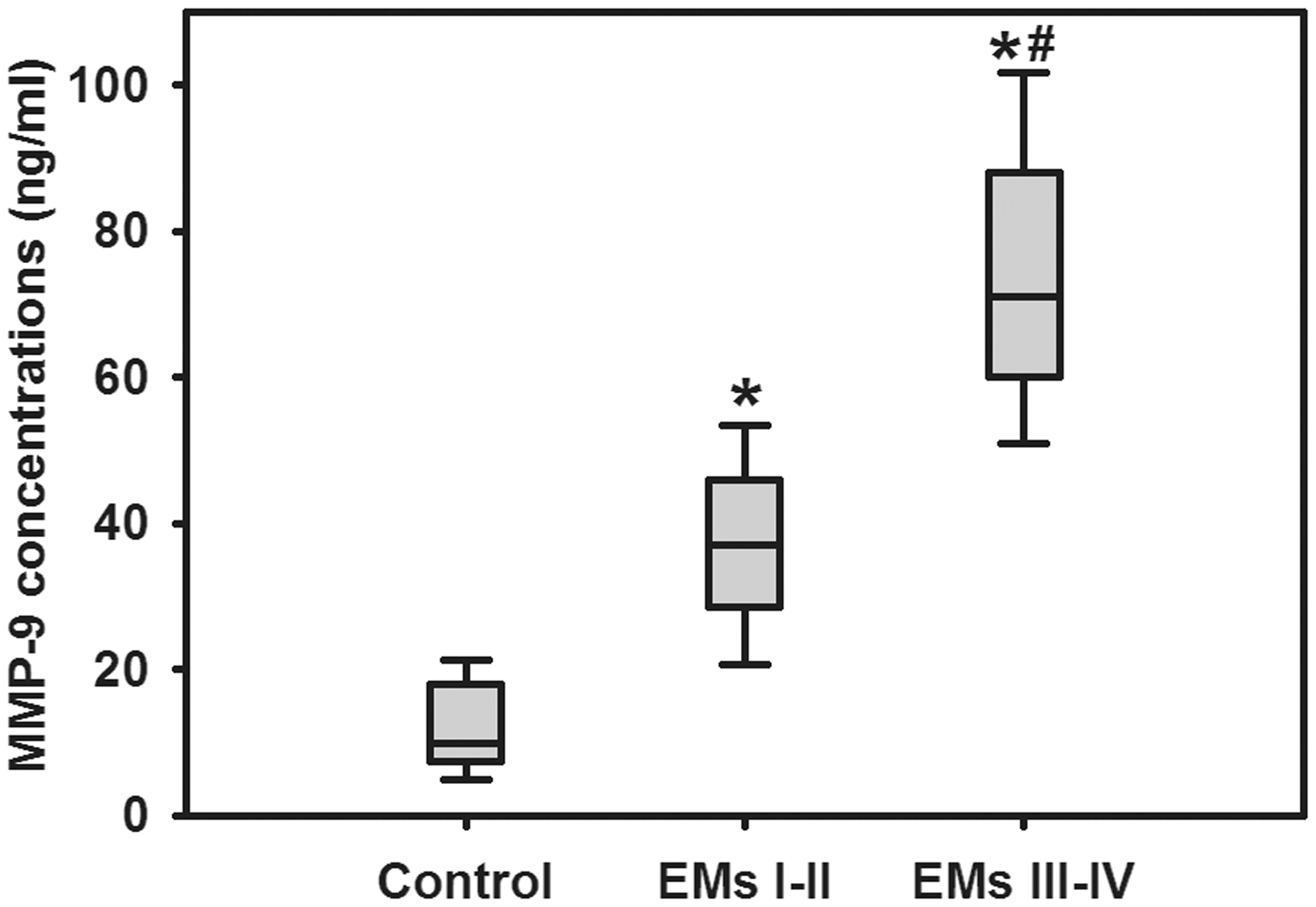
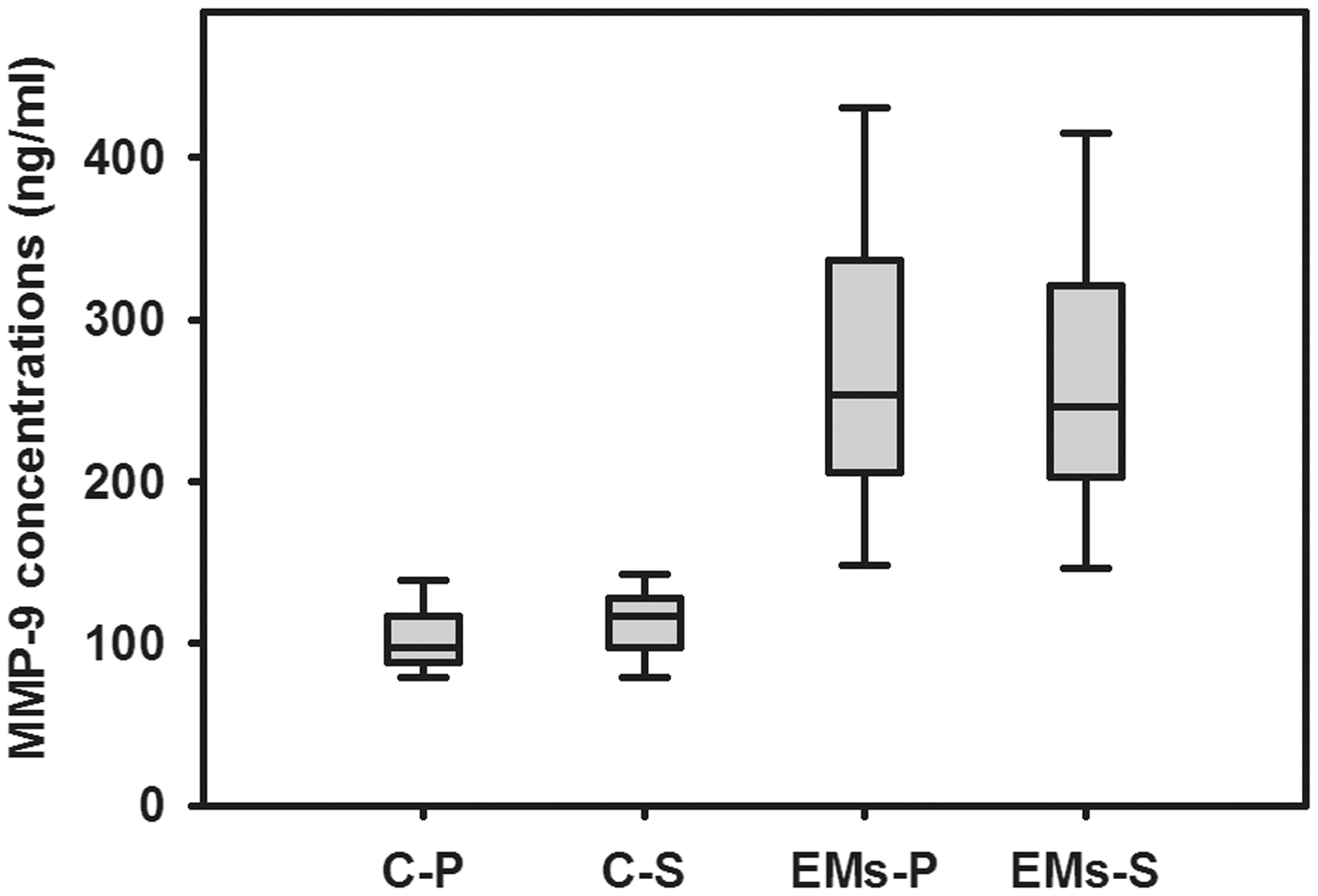
To clarify whether the concentrations of MMP-9 in plasma and PF would be affected by the menstrual cycle, we analysed the concentrations of MMP-9 in the proliferative and secretory phase of the menstrual cycle in both groups A and B, as illustrated in Figures 3 and 4. MMP-9 concentrations did not correlate with the menstrual cycle phase either in endometriosis (A) or control group (B).
Enzyme matrix metalloproteinase (MMP)-9 concentrations in the plasma of patients with endometriosis and controls as a function of the menstrual cycle stage. C-P and C-S denote controls in the proliferative and secretory phase of the menstrual cycle, respectively; EMs-P and EMs-S denote patients with endometriosis in the proliferative and secretory phase of the menstrual cycle, respectively. Enzyme matrix metalloproteinase (MMP)-9 concentrations in the PF of patients with endometriosis and controls as a function of the menstrual cycle stage. C-P, C-S, EMs-P and EMs-S denote the same as in Figure 3.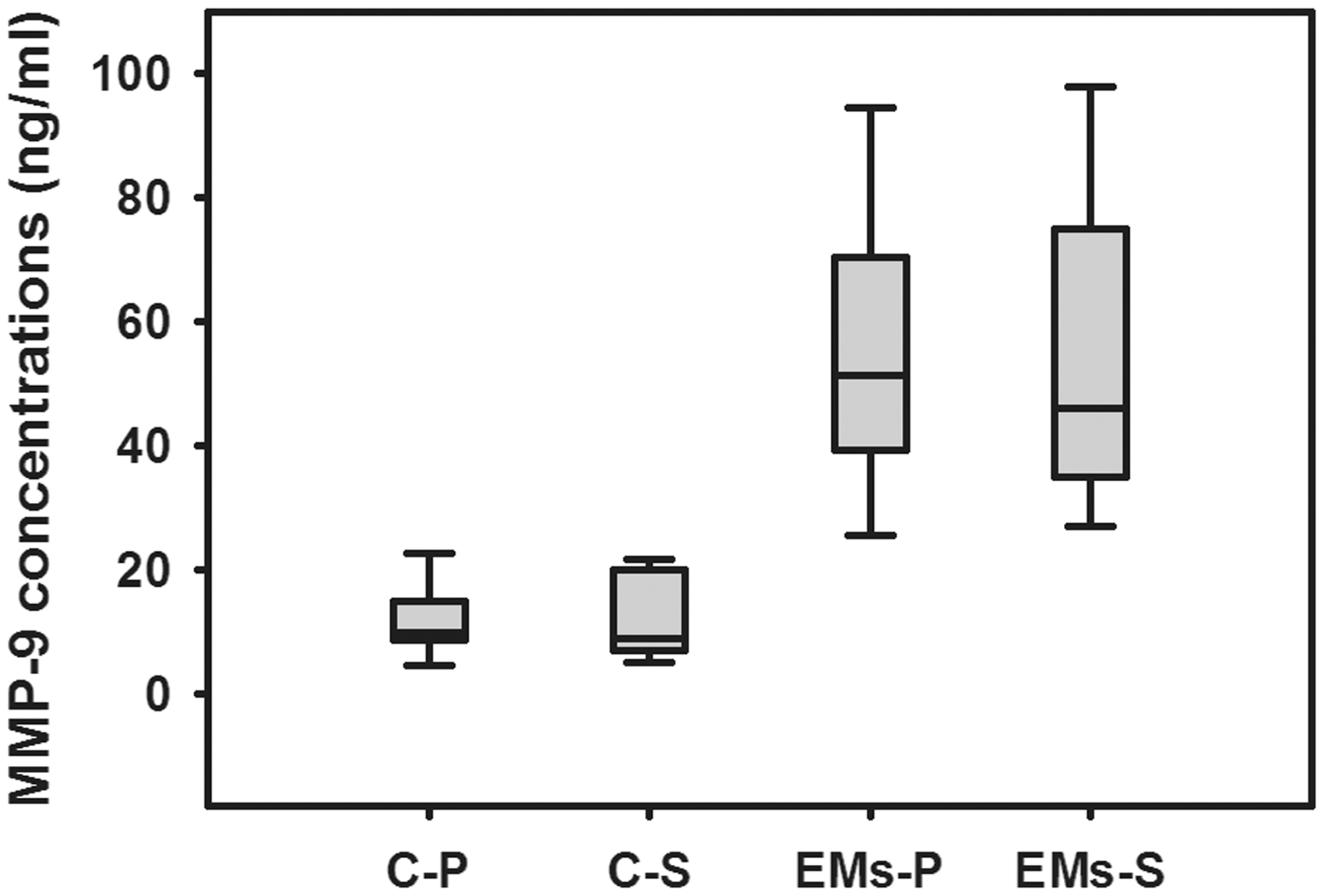
Association of MMP-9 concentrations in plasma and PF with endometriosis severity
In the correlation analysis, Spearman’s rank correlation analysis showed that MMP-9 concentrations in plasma and PF were both positively correlated with severity of endometriosis (r = 0.56, P < 0.001 and r = 0.63, P < 0.001, respectively). After adjusting for other variables such as age and BMI, multinomial logistic regression analysis showed that MMP-9 concentrations in plasma and PF were still both positively correlated with the stage of the disease (chi-square = 9.7, P = 0.004 and chi-square = 11.5, P = 0.003, respectively).We also analysed the association of MMP-9 concentrations in plasma and PF of endometriosis females; the results showed that plasma MMP-9 concentrations had a positive correlation with PF MMP-9 concentrations (r = 0.61, P < 0.001) (Figure 5).
Correlation between enzyme matrix metalloproteinase (MMP)-9 concentrations in plasma and peritoneal fluid (PF) of patients with endometriosis (r = 0.61, P < 0.001).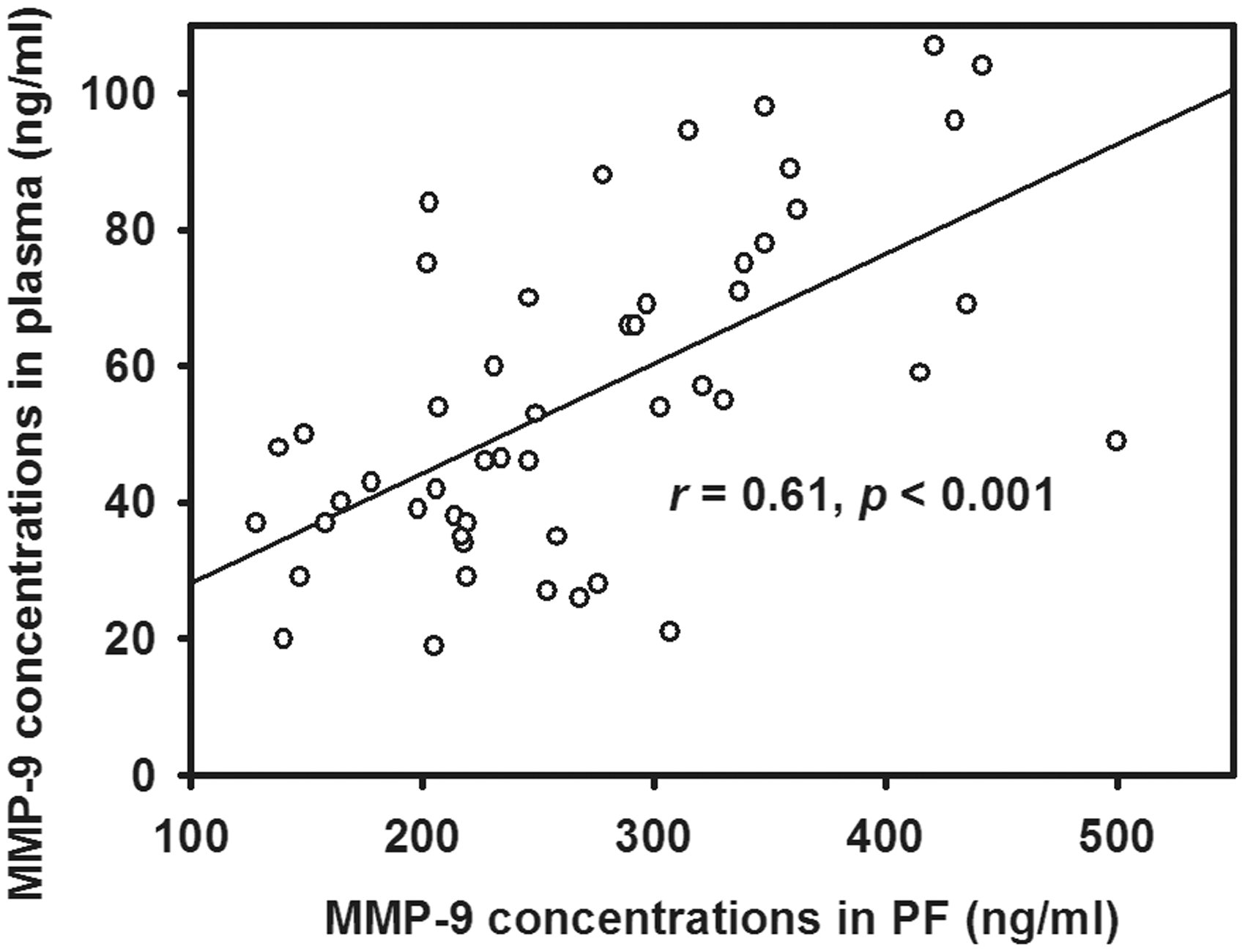
Discussion
In the present study, we demonstrated that females with endometriosis had significantly elevated plasma and PF MMP-9 concentrations compared to non-endometriosis controls, and this elevation did not correlate with the menstrual cycle phase. Besides, plasma and PF concentrations of MMP-9 were both significantly higher in those females with advanced stages of endometriosis (moderate/severe endometriosis) compared to those in the early stages (minimal/mild endometriosis). To the best of our knowledge, this study is the first to show that MMP-9 has been detected in both plasma and PF obtained from females with endometriosis, and that MMP-9 concentrations are positively correlated with the severity of disease; this correlation remained significant after the adjustment of potential confounders such as age and BMI. Our findings suggest enhanced local and systemic production of MMP-9 in endometriosis, but it should be noted that the concentration of MMP-9 in PF was a great deal higher than that in paired plasma samples. The mechanism of this increase may be attributed to either local secretion of MMP-9 residing in ECM, increased MMP-9 synthesis or both. The MMP-9 in PF may originate from endometrial cells of the local tissues because MMP-9 is endogenously expressed in endometrium.16,17 Additionally, this observation indicates a significant elevation in the systemic and local expression of MMP-9 in females with advanced endometriosis, but the mechanism for this increase in plasma and PF of patients with endometriosis requires further investigation. It can possibly be attributed to two reasons: (1) greater tissue remodeling that may occur with disease progression, with a consequent higher local and systemically identifiable MMP-9 activity; (2) the inflammatory microenvironment in ectopic tissue may increase the production of MMP-9, which in turn facilitates invasion and progression of the disease, being positively correlated with the severity of endometriosis. 21
In a recent study by Malvezzi et al., 19 the authors compared the concentrations of MMP-2 and MMP-9 in the FF of infertile females with or without endometriosis; no difference was observed in MMP-2 or MMP-9 concentrations in FF among females with or without endometriosis or at different stage of endometriosis; however, significantly higher MMP-2 concentrations were detected in the serum of females with stage III/IV endometriosis compared to those with stage I/II endometriosis, which is consistent with our results. The data regarding the quantification of MMP-9 in serum were not presented in their study. In a study by Gerlach et al., 22 it was demonstrated that samples containing ethylenediaminetetraacetic acid as an anticoagulant or serum samples could artificially increase pro-MMP-9 and MMP-9 activity compared to the other collection methods (into citrate or heparin plasma samples), so that an accurate estimate of MMP-9 could not be obtained. This is why heparin plasma samples were used in the present study. Szamatowicz et al. 12 demonstrated for the first time that mean total MMP-9 concentrations in the PF of patients with mild or moderate endometriosis were higher than that of controls, but not active MMP-9 concentrations, this is similar to our observation. However, they did not analyse the correlation of PF concentrations with the disease severity of endometriosis. A further study tested the hypothesis that raised serum concentrations of MMPs might reflect the severity of endometriosis 23 ; they compared serum concentrations of MMP-9 and its tissue inhibitor TIMP-2 in infertile females with either mild (stage I, n = 15) or severe endometriosis (stage IV, n = 22). There was no difference in the concentrations of MMP-9 and TIMP-2 between the two groups, which is in contrast to our results. This discrepancy may be due to different sample types between the two studies, and/or divergence originating from the relatively small numbers of enrolled patients in both studies.
Therefore, in our hands measurements of plasma and PF concentrations of MMP-9 may serve as a biochemical parameter for determining disease severity and predicting the prognosis of endometriosis. However, we have been aware of several potential limitations existing in this study. First, as this was a cross-sectional study which included a relatively small number of subjects, it is impossible to determine whether a definite cause-and-effect relationship exists. Further longitudinal studies with a larger population sample are warranted to substantiate our results. Second, we did not analyse the relationship between MMP-9 concentrations in the plasma and PF and menstrual pain experienced by endometriosis patients. Further studies are needed to investigate the role of MMP-9 concentrations for predicting menstrual pain in patients with endometriosis.
In conclusion, this study revealed a significant elevation of MMP-9 concentrations in plasma and PF of patients with endometriosis compared to non-endometriosis controls and illustrated a pronounced positive correlation of plasma and PF MMP-9 concentrations with severity of the disease. This study is the first to show that plasma and/or PF MMP-9 may be used as a biomarker to predict the disease severity of endometriosis and MMP-9 concentrations in plasma were directly correlated with those in PF. Further larger population investigations are needed to define the mechanisms underlying this correlation.
Footnotes
Acknowledgements
We are grateful to the patients for donating their samples to our research studies, staff within the research and clinical teams at Reproductive Medicine Centre of Jinan Military General Hospital for help in obtaining and processing samples for funding this research.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by grant from PLA General Logistics Department of the Ministry of Health [No.13QNP030].
Ethical approval
The ethics committee of Jinan Military General Hospital approved this study (2013JMGH028).
Guarantor
TH.
Contributorship
HL and TH researched literature and conceived the study. JW, HW, NT, YL and YZ were involved in protocol development, gaining ethical approval, patient recruitment and data analysis. HL and TH wrote the first draft of the manuscript. All authors reviewed and edited the manuscript and approved the final version of the manuscript.