
Abstract
Objective
The menstrual cycle-related changes in clinical laboratory values were analysed by use of data obtained in the Asian multicentre study aimed at derivation of common reference intervals for 85 major clinical laboratory tests.
Methods
Among 1876 healthy female volunteers, 893 had regular menstruation. They were classified into five groups according to dates between sample collection and the start of the last menstrual cycle: early follicular phase (1–6 days), late follicular phase (7–12 days), ovulatory phase (13–16 days), early luteal phase (17–22 days), and late luteal phase (23–31 days). Multiple linear regression analysis was performed to evaluate the menstrual cycle-related changes in test results. The magnitude was expressed as a standard deviation ratio of between-phase standard deviation to between-individual standard deviation based on nested ANOVA.
Results
Aside from obvious changes for four sex hormones (oestradiol, progesterone, follicle-stimulating hormone, and luteinizing hormone), we observed statistically significant menstrual cycle-related changes in the following tests (standard deviation ratio >0.15): Na, Cl, creatine kinase, C-reactive protein, serum amyloid A, carbohydrate antigen 125, and parathyroid hormone were higher during the early follicular phase, while insulin, total cholesterol, and white blood cell were higher during the luteal phase. Significant associations of those test items with the four sex hormones were revealed.
Conclusions
The menstrual cycle-related changes in laboratory test results were revealed in some commonly tested items other than sex hormones. The findings are of interest in understanding female physiology in relation to hormonal changes, but the magnitude of changes is rather small and not very relevant in interpreting test results.
Keywords
Introduction
In interpreting laboratory test results, it is important to consider biological sources of variations (SV) before considering pathological causes of changes in values.
Biological SVs are grouped into within-individual and between-individual SV. The former includes a host of factors such as posture, physical or emotional stress, and food intake, plus the menstrual cycle in female. Although menstrual cycle-related changes are well known for sex hormones, 1 there have been no clear-cut reports about other commonly measured laboratory tests. Munford reported in 2010 that serum total cholesterol, LDL-cholesterol, and triglycerides increase during the follicular phase while high-density lipoprotein (HDL)-cholesterol increases at the mid-cycle. 2 Garskins showed in 2012 that C-reactive protein (CRP) by high-sensitive assays is higher in females during the follicular phase. 3 In 2014, Schisterman published a review analysing menstrual cycle-dependent changes in various cardiometabolic biomarkers. However, the literature is somewhat contradictory about the magnitude and direction of the changes. 1
In 2009, we conducted a large-scale multicentre study for the derivation of common reference intervals (RI) in East and Southeast Asia, targeting 85 major laboratory tests including health screening items (general chemistry and complete blood count (CBC)), inflammatory markers, tumour markers, major hormones, and vitamins.4,5 Prior to donating blood, each volunteer answered a detailed questionnaire which included the date of onset of the last menstrual period.
In this study, we comprehensively analysed menstrual cycle-related changes for all the test items by use of multivariate analysis and discuss the implication of the findings in interpreting test results in females.
Materials and methods
Source data
The International Federation of Clinical Chemistry and Laboratory Medicine, the Committee on Reference Intervals and Decision Limits, and the Asian and Pacific Federation of Clinical Biochemistry, along with the Japan Society of Clinical Chemistry and the Japanese Society of Laboratory Medicine, conducted a multicentre study for derivation of common RIs.4,5 In this study, the results of 85 test items were analysed in relation to the time in the menstrual cycle and other SVs obtained from a questionnaire, which included age, sex, occupation, body height, body weight, body mass index (BMI), blood type, alcohol consumption, smoking status, exercise, physical activity concentration, menstrual cycle data, and food habits.
The volunteers participating in this study consider themselves to be healthy. Those volunteers who had any of the following were excluded: (1) BMI ≥ 28 kg/m2, (2) excessive daily consumption of alcohol (≥75 g ethanol), (3) smoking >20 cigarettes/day, (4) regular medication for chronic diseases, (5) hospitalization for any acute disease or surgery within the past two weeks, or (6) known carrier status for HBV, HCV, or HIV. Those who met the study conditions were 3314 volunteers (1438 males and 1876 females) between 20 and 65 years old. After they had fasted for 10 h or more, blood was collected after having relaxed for more than 20 min in sitting position.
Since the aim of this study is to clarify the menstrual cycle-related changes in laboratory data, we applied additional exclusion criteria to the 1876 females based on answers to the query items regarding menstruation in the questionnaire (the last period, regularity of the cycle, and average duration of each cycle) as follows: (1) postmenopausal state, (2) irregular menstrual cycles, (3) duration of menstrual cycle of ≤24 or ≥32 days, (4) no answer to the date of the last period, or (5) ≥32 days after onset of the last period. By this selection process, total of 893 female volunteers were eligible for the study.
This study was approved by the Ethical Committee of Yamaguchi University Graduate School of Medical Sciences as well as by each institutional research board of all the collaborating laboratories. The main incentive for the volunteers was free provision of results for all 85 analytes. All volunteers signed informed consent forms.
Measurements
Blood was collected into a vacuum blood collection tube containing a serum-separating agent. After the blood was centrifuged for 10 min at room temperature, serum was aliquoted and cryopreserved at ≤ −80℃. All collected samples were transferred to Beckman Coulter, Inc., Ariake Research Laboratory, Tokyo, Japan, and measured collectively.
List of test items and analytical methods.

Transf.: Logarithmic transformation was made in analysing test results of the corresponding item.
Detailed information on the measurements including assay precision was described elsewhere4,5 except for that of CBC, which was not included in the previous reports. Harmonization of CBC results among laboratories was achieved by use of a common calibrator (S-CAL) and the web-based monitoring system called Interlaboratory Quality Assurance Program (IQAP). 6
Statistical analyses
On the basis of the number of days between the date of blood collection and the date of the last menstrual period as answered in the questionnaire, the menstrual cycle was classified into five phases as follows: early follicular phase (1–6 days), late follicular phase (7–12 days), ovulatory phase (13–16 days), early luteal phase (17–22 days), and late luteal phase (23–31 days).
Statistical significance of differences in test results among the five menstrual phase groups was evaluated by the Kruskal–Wallis test. Three-level nested ANOVA (3N-ANOVA) was used to examine the magnitude of possible influence of three major SVs: country (Japan, Korea, China, Taiwan, Hong Kong, Viet Nam, Malaysia, and Indonesia), age (≤30, 31–40, and ≥41 years), and menstrual cycle (five phases as shown above).
Standard deviations (SD) were computed for differences among countries (SDcntr), among age groups (SDage), among menstrual phases (SDcycle), and the residual SD which corresponds to between-individual SD (SDindiv) adjusted for the effect of country, age, and menstrual cycle.7−10 The standard deviation ratio (SDR) of each factor relative to the SDindiv was computed as SDRcntr, SDRage, and SDRcycle. SDR >0.3 was adopted as a guide to judge the need for partitioning reference values. Among the five groups, there were no significant differences in age, height, weight, BMI, and waist circumference.
Multiple linear regression analysis (MRA) was performed with each of the 85 test items set as a target variable. Five dummy variables representing each country (Taiwan and Hong Kong were merged into China) were set as explanatory variables, with Japan as the reference category, age, BMI, and four dummy variables representing each menstrual phase with early follicular phase set as reference category. In the second round of MRA analysis, dummy variables for the menstrual cycle were replaced by the four sex hormones (oestradiol, progesterone, FSH, and LH), keeping other explanatory variables in place. Because of the large data-set, the standardized partial regression coefficient (which corresponds to the partial correlation coefficient: rp) was statistically significant at P = 0.01 when rp was as small as 0.08. Therefore, we focused on the absolute value of rp and judged it as significant only with |rp| ≥ 0.15.
Test results of 33 items showed apparent skewness in the distribution, and thus they were logarithmically transformed to make the distribution closer to the Gaussian pattern (Table 1). The Kruskal–Wallis test, 3N-ANOVA, and MRA were performed by use of general purpose statistical software, StatFlex Ver. 6 (Artech Co., Ltd, Osaka, Japan).
Results
Kruskal–Wallis test for between-menstrual phase differences
Results of Kruskal–Wallis test (KW) and three-level nested ANOVA for menstrual cycle-related changes.

Kruskal–Wallis (KW) test was performed to test for significance of menstrual cycle-related changes.
Three-level nested ANOVA was used to derive SD due to between-country, between-age, and between-menstrual cycle-related changes.
SD ratio (SDR) representing each source of variation was computed as its ratio to SD representing between-individual variations.
Analysis of differences by country, age, and menstrual cycle by 3N-ANOVA
The test results of 893 subjects were analysed using 3N-ANOVA by setting country, age, and menstrual phase as three SVs, and SDcntr, SDage, SDcycle, and SDindiv were then derived. SDRcntr, SDRage, and SDRcycle were computed by taking the ratios of the respective SD to the SDindiv. In this study, SDRcntr > 0.3 were noted in 24 items: K, urea, TP, Glob, IgG, CRP, SAA, C3, C4, retinol-binding protein (RBP), transthyretin (prealbumin) (TTR), triglycerides (TG), HDL-C, alkaline phosphatase (ALP), ApoA1, TRAP-5b, ferritin, CA15-3, PTH, folate, adiponectin, WBC, Bas, and PLT. SDRage > 0.3 were noted for 11 items: Ca, IP, TP, Alb, Glu, TC, LDL-C, ApoB, FSH, testosterone, and dehydroepiandrosterone sulphate (DHEA-S).
With SDRcycle > 0.3, partitioning by menstrual phase was applied to oestradiol (0.49), progesterone (0.87), FSH (0.45), and LH (0.35). All other test items showed SDRcycle < 0.3 (Table 2). However, for the physiological evaluation of menstrual cycle-related changes, we chose the following 30 test items with SDRcycle > 0.15 for further analysis: Na, K, Cl, Glob, IgG, IgM, CRP, SAA, C4, RBP, TC, TG, LDL-C, CK, ApoB, Bone-ALP, alfa-fetoprotein, CA15-3, insulin, PTH, FT3, adiponectin, WBC, Neu, Bas, oestradiol, progesterone, FSH, and LH (Table 2).
MRA
Partial correlation coefficients between each test item and sources of variations by multiple regression analysis.
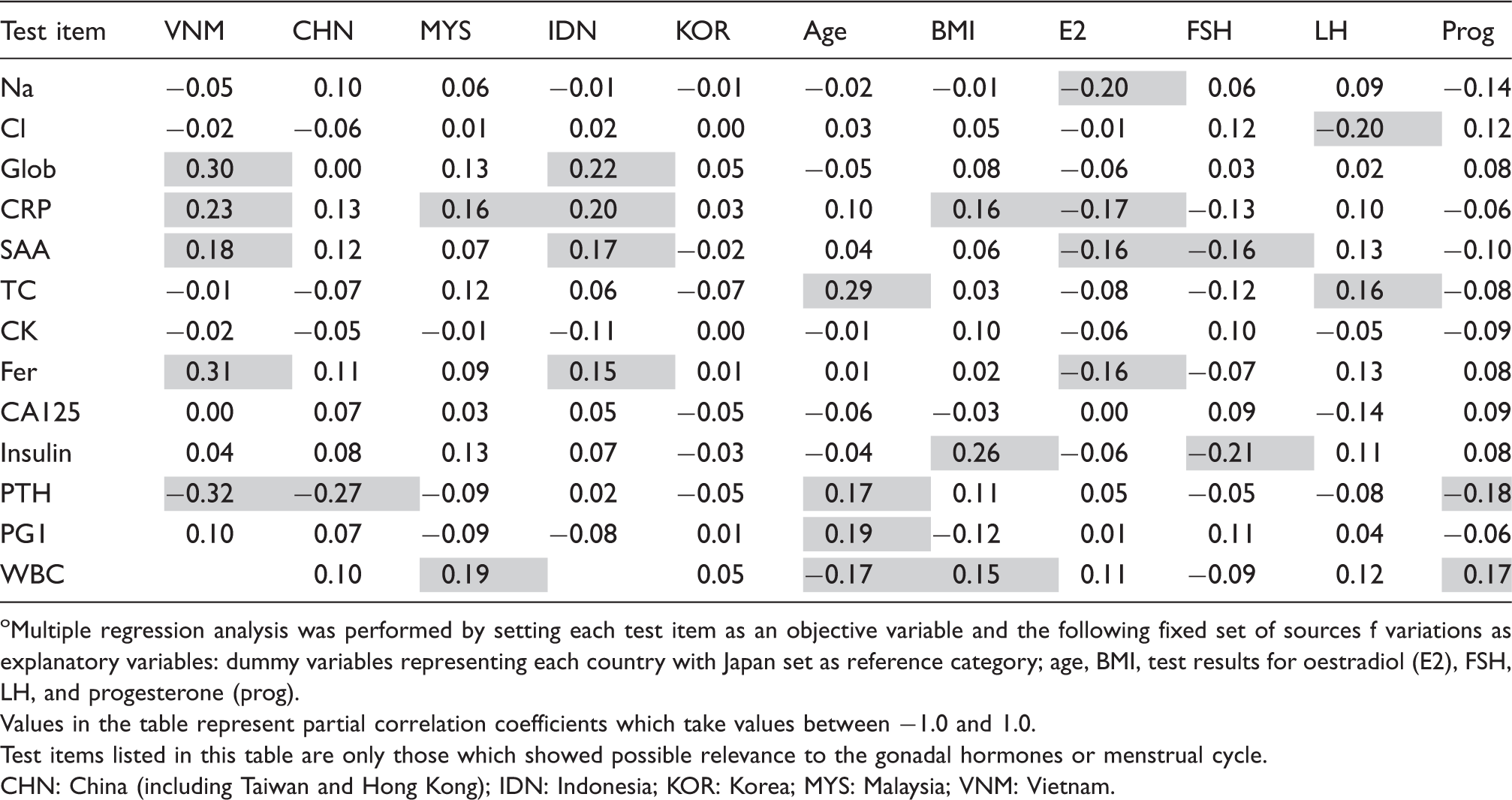
Multiple regression analysis was performed by setting each test item as an objective variable and the following fixed set of sources f variations as explanatory variables: dummy variables representing each country with Japan set as reference category; age, BMI, test results for oestradiol (E2), FSH, LH, and progesterone (prog).
Values in the table represent partial correlation coefficients which take values between −1.0 and 1.0.
Test items listed in this table are only those which showed possible relevance to the gonadal hormones or menstrual cycle.
CHN: China (including Taiwan and Hong Kong); IDN: Indonesia; KOR: Korea; MYS: Malaysia; VNM: Vietnam.
Partial correlation coefficients between each test item and sources of variations by multiple regression analysis.
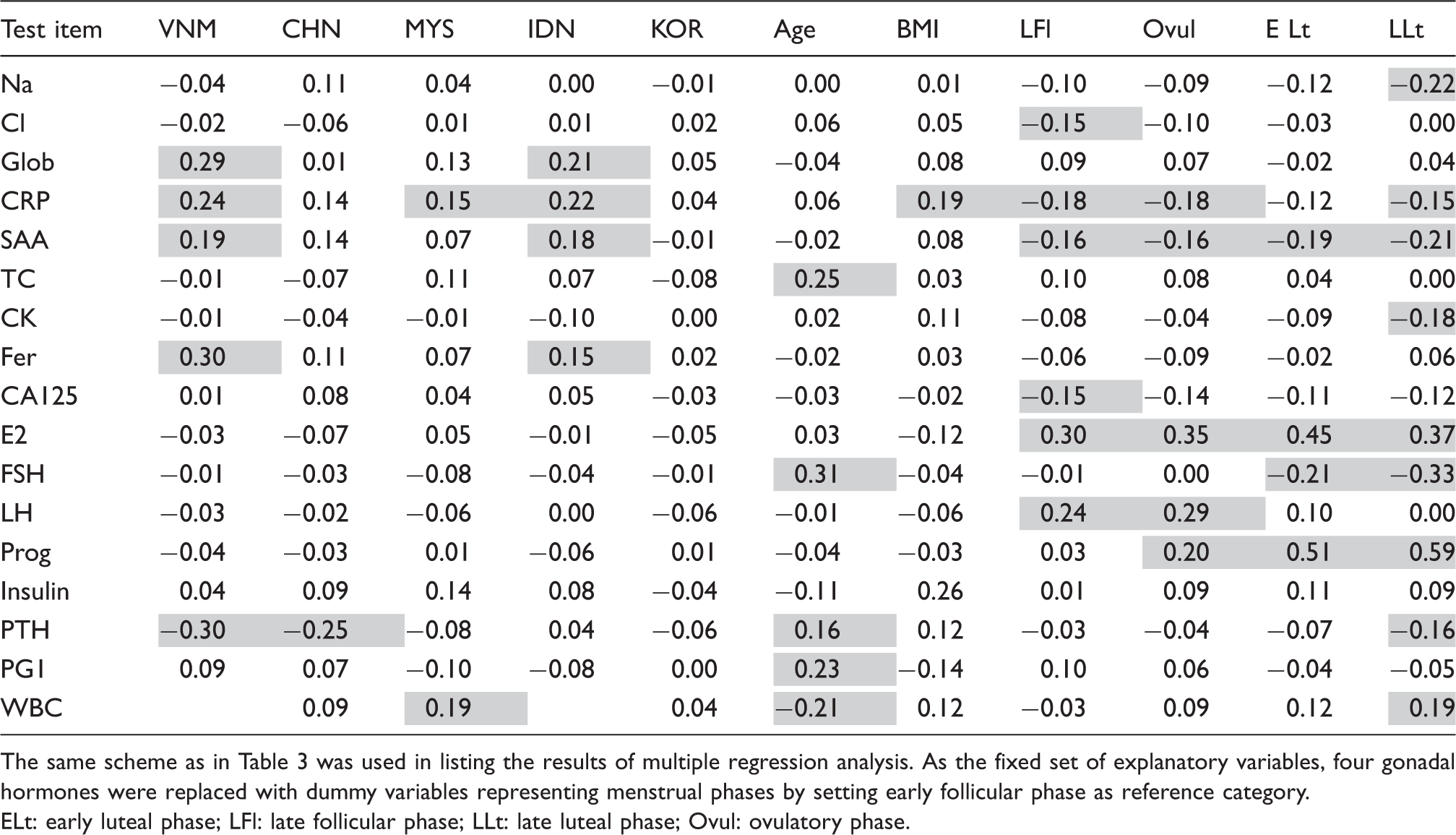
The same scheme as in Table 3 was used in listing the results of multiple regression analysis. As the fixed set of explanatory variables, four gonadal hormones were replaced with dummy variables representing menstrual phases by setting early follicular phase as reference category.
ELt: early luteal phase; LFl: late follicular phase; LLt: late luteal phase; Ovul: ovulatory phase.
Discussion
In this study, we evaluated menstrual cycle-related changes in laboratory test results in healthy females with regular cycles. The magnitude of the changes was computed as SDR after adjusting for the influence of each subject’s age and country of origin by use of 3N-ANOVA. In our previous study, we reported that regional differences were observed in inflammatory markers such as TP, IgG, CRP, SAA, C3, C4, and also nutritional markers such as TG, HDL-C, ApoA1, folate, adiponectin, tumour markers such as ferritin and CA15-3, and bone markers such as PTH and TRAP-5b.4,5 In addition to these parameters, differences among regions were noted in measurements of nine items: K, urea, Glob, ALP, TTR, RBP, WBC, Bas, and PLT in premenopausal female. From the ANOVA results, between-age differences were detected in Ca, IP, TP, Alb, Glu, TC, LDL-C, ApoB, FSH, DHEA-S, and testosterone in premenopausal female.
Between-menstrual phase differences were significant in 15 test items by the Kruskal–Wallis test. The four sex hormones are known to fluctuate during the menstrual cycle, with SDRcycle > 0.3, and the menstrual phase-specific RIs were derived for them. On the other hand, another 11 analytes (Na, Cl, CRP, SAA, TC, CK, ferritin, CA125, insulin, PTH, and WBC) showed significant association with the menstrual phase and/or one or more of the sex hormones. The actual profiles of menstrual cycle related change are shown in Figure 1.
Menstrual cycle-related changes for selected analytes. Healthy female volunteers with regular menstrual cycles were subgrouped by the period between the first day of the last period and the blood sampling date into early follicular (EFl), late follicular (LFl), ovulatory (Ovul), early luteal (ELt), and late luteal phases (LLt). The box in the scattergram for each subgroup represents the central 50% range of values and the vertical line in the centre of the box indicates the median.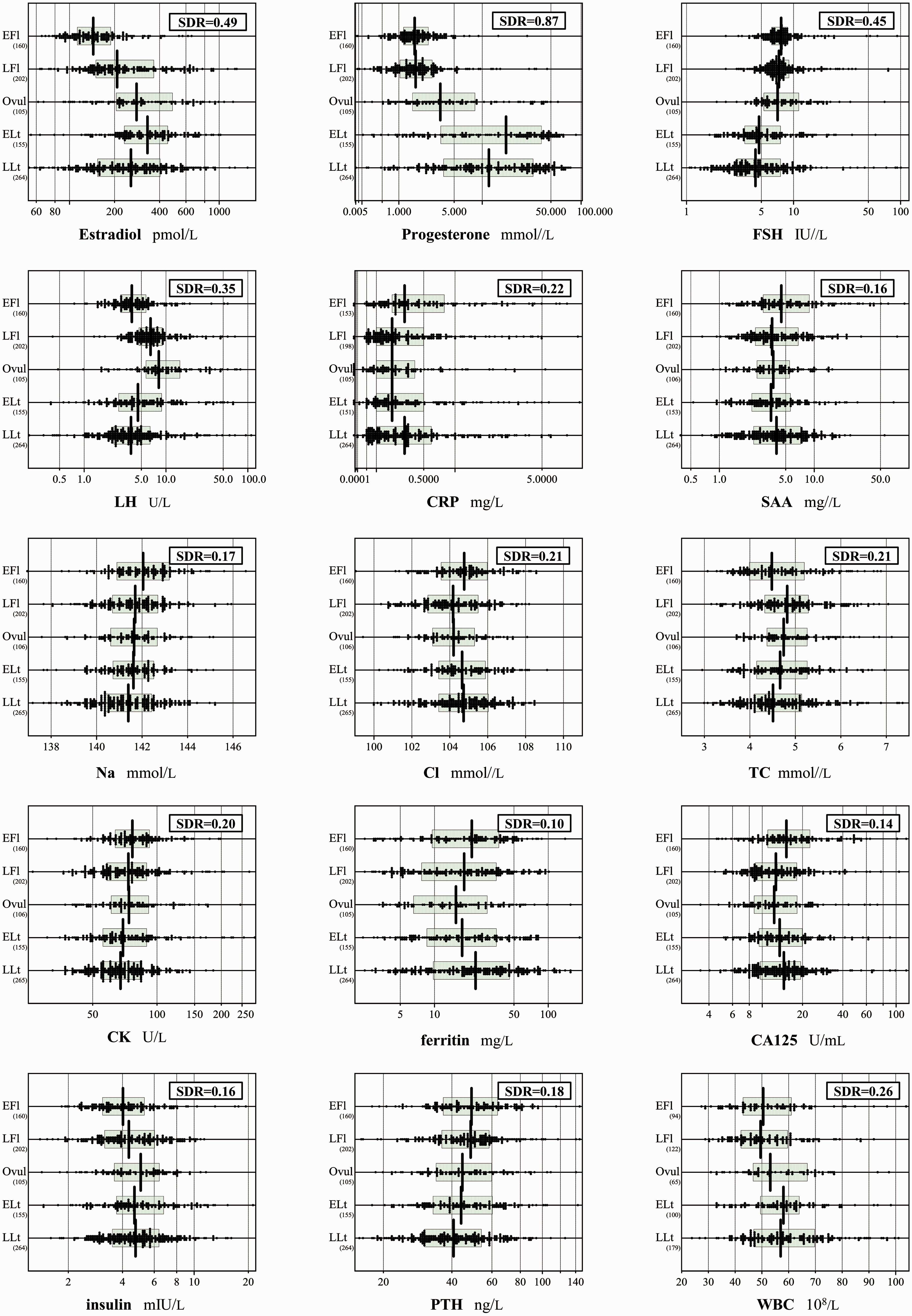
Oestrogen is well known to affect lipoprotein metabolism. For example, oestrogen promotes the clearance of chylomicron remnants, stimulates hepatic lipid production, increases very low-density lipoprotein synthesis and the production of HDL, and enhances the expression of the LDL receptor.11–16 However, reports on relationships between lipoproteins and sex hormones across the menstrual cycle have been inconsistent. 1 We demonstrated that TC was higher in the late follicular phase than in the early follicular phase, and TC was positively correlated with LH. Similar fluctuations of TC during the menstrual cycle have been seen in several former reports. 1
The synthesis of CRP, an acute-phase protein, is induced by TNF-α, IL-1β, and IL-6, and is synthesized in the liver by macrophages. 17 CRP is used as a serum marker for vascular inflammation and is a useful predictive marker for cardiovascular risk.18–21 Serum oestrogen concentration is known to affect serum CRP concentrations, and oral administration of an exogenous oestrogen preparation to postmenopausal female increases the CRP concentration. 22 SAA is also known to be a sensitive inflammatory marker, 23 and it is thought that SAA can also be used as a predictive marker for cardiovascular risk. 24 The oral administration of oestrogen is also known to increase the SAA concentration, as with the CRP concentration. 25 Serum CRP is known to fluctuate during the menstrual cycle and is accompanied by the fluctuation of endogenous oestrogen. Since SAA is likewise affected by oestrogen administration, it is also predicted to fluctuate during the menstrual cycle. In this study, we found that both SAA and CRP were inversely associated with serum oestradiol and fluctuated depending on the concentration of serum oestradiol during the menstrual cycle. Fluctuations of serum CRP concentration during the menstrual cycle have been studied previously; however, the fluctuations have not been observed in several studies.26–28 In contrast, a recent study that chronologically evaluated the relation between concentrations of high-sensitive CRP assays and endogenous sex hormones in premenopausal female over the entire menstrual cycle showed that CRP fluctuated significantly (P < 0.001). 29 Our results showed that the CRP concentration in the early follicular phase was significantly higher (P < 0.01) than that in the late follicular phase and was also significantly higher (P < 0.05) than that in the ovulatory and late luteal phases. These results are consistent with the report by Gaskins et al. 3 and support the hypothesis that endogenous oestrogen may exert an anti-inflammatory effect. 30 In addition, the concentration of SAA, similar to that of CRP, was higher in the early follicular phase than in the ovulatory and luteal phases. TNFα is a cytokine that promotes the synthesis of both CRP and SAA in the liver. TNFα is known to inhibit cholesterol efflux to HDL, 31 suggesting the possibility that the action of oestrogen on cytokines including TNFα may regulate the fluctuations of CRP and HDL during the menstrual cycle. Previous studies reported that an increase in serum oestrogen causes a decrease in CRP, whereas an increase in progesterone causes an increase in CRP.3,30 Because the study designs of these previous studies differ from ours, the results cannot be compared directly. Progesterone enhances neutrophil chemotaxis, increases production of some inflammatory mediators by monocytes, 32 causes activation of NK cells, and decreases the production of NO synthase and the activation of T cells. 33 These results suggest that the increase in progesterone is related to anti-inflammatory effects in normal female with a normal menstrual cycle. However, the results in this study showed that CRP and SAA were not significantly associated with progesterone.
Progesterone plays an important role in regulating bone metabolism. Progestins have been demonstrated to increase gene expression of PTH and the progesterone receptor in the parathyroid gland. 34 In this study, however, PTH was significantly higher in the early follicular phase compared to the concentration in the late luteal phase, and PTH was negatively correlated with progesterone. Our results coincide with other previous reports.35–38
In this study, we observed that serum concentrations of CK, insulin, WBC, Na, and Cl also fluctuated in relation to the menstrual cycle. Serum CK activity was significantly lower in the late luteal phase of the cycle, but CK activity had no correlated sex hormone values. Serum insulin was higher in the early luteal phase of the menstrual cycle; its concentrations were negatively correlated with FSH. WBC was significantly higher in the late luteal phase. IL-6 transduction by oestrogens and progesterone may affect these parameters.
There are few reports on the fluctuation of serum electrolytes during the menstrual cycle. The present study clearly shows that serum Na is lower in the luteal phase compared to the early follicular phase, and serum Na is negatively correlated with oestradiol. These findings match well with the phenomenon of surge in Na concentration after menopause when oestradiol drops sharply. 39 On the other hand, serum Cl was significantly lower during late follicular phase compared to the early follicular phase. Cl was negatively correlated with LH.
Conclusion
From 893 well-defined healthy females with regular menstrual cycles, we analysed menstrual phase-related changes for 85 major laboratory tests, including CBC, chemical analytes, tumour markers, and various hormones. In the four sex hormones, well-known menstrual cycle-related changes were conspicuously observed. Based on ANOVA (SDR for menstrual cycle-related changes) and multiple regression analysis (partial correlation coefficients), we revealed statistically significant menstrual cycle-related changes in the following test items: Na, Cl, CRP, SAA, CA125, and PTH are higher during the early follicular phase when oestradiol is in its nadir, while WBC is higher during the luteal phases, with no direct association with the concentration of sex hormones. However, the magnitude of these changes is rather small and not very relevant in daily interpretation of laboratory test results.
Footnotes
Acknowledgements
We are in great debt to all the colleagues in the laboratories who collaborated in the 2009 Asian study and allowed us to use the data-set for our secondary analyses to elucidate menstrual cycle-related variations of laboratory test results performed in this study.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
This study was approved by the Ethical Committee of Yamaguchi University Graduate School of Medical Sciences (193-1).
Guarantor
TK.
Contributorship
KI led the Asian multicentre study and SM collaborated in the study in recruiting healthy volunteers. KI provided the full data-set for analyses done in this study. SM, KI, and TK designed this observational study for exploring the menstrual cycle-related changes. SM analysed the data-set. SM and TK wrote the manuscript. KI edited the manuscript. All authors approved the final version.