
Abstract
Background
Age-specific trends of serum testosterone and sex hormone-binding globulin across the full lifespan have not been reported.
Methods
We deduced age-specific trends in serum testosterone and sex hormone-binding globulin in males and females between ages 10 and 90 from a large sample of consecutive results from a single large pathology laboratory. Coded results of 110,712 consecutive blood samples requesting serum testosterone over seven years (2007–2013) comprising blood testosterone, sex hormone-binding globulin and calculated free testosterone together with gender and age were analysed create smoothed age-specific centiles (2.5%, 5%, 25%, 50%, 75%, 95%, 97.5%) for males and females.
Results
These identified the pubertal increases in serum testosterone in males peaking at 20 years of age and remaining stable thereafter until the eighth decade. In females, circulating testosterone peaked in late adolescence and declined gradually over the next two decades but remained stable across menopause and beyond. After early childhood, serum sex hormone-binding globulin declines to a nadir in males at the age of 20 years and remains stable till the sixth decade with a gradual, progressive rise thereafter. In females, the sex hormone-binding globulin nadir is reached earlier with levels rising gradually and progressively with age thereafter and accelerating after the age of 70 years. Females also exhibit a second sex hormone-binding globulin peak during reproductive ages reflected only in upper centiles due to effects of pregnancy and oral contraceptive use in a significant minority of females.
Conclusions
This large sample of clinical data provides a comprehensive profile of androgen status across the lifespan from early adolescence to late old age.
Introduction
Testosterone is the pivotal hormone in determining male sexual differentiation, development, maturation and reproductive function from conception to death. 1 Recent studies prove that androgen receptor-mediated androgen action, predominantly exerted by circulating testosterone, is also essential for optimal female reproductive function 2 while hyperandrogenism is a key component of polycystic ovary syndrome, the most frequent endocrinopathy of young females.3,4 Yet, despite the significance of circulating testosterone throughout the lifespan, there is no report of the age-specific profile of circulating testosterone in males and females from birth to advanced old age.
Specific measurement of testosterone became possible with the invention of steroid immunoassay in 19695 with the first testosterone immunoassay described soon after. 6 Subsequently, increasing demand for testosterone measurement in clinical practice and research led to incorporation of testosterone immunoassay into multiplex platforms which increased throughput at lower cost. Increasingly large population studies have aimed to define the age-specific patterns of circulating testosterone in studies involving up to several thousand participants.7–10 However, all published studies feature restricted age ranges and different testosterone assays. In recent decades, routine clinical practice incorporates a high utilization of testosterone immunoassays to evaluate androgen status in neonates (disorders of sexual differentiation), during puberty (pubertal status), adulthood (sexual and reproductive function) and ageing. In all these clinical contexts circulating testosterone measurement is usually aimed to identify or, much more often, exclude relevant reproductive system disorders. Although reproductive system disorders are relatively uncommon among the general population, they are so readily treatable that medico-legal concern over missed diagnosis effectively drives tacit population screening using testosterone assays. On this background and employing statistical methods to extract underlying data distributions from big datasets, we have used a large sample of consecutive hormone assays from a large pathology laboratory to deduce the age-specific profile of circulating testosterone across the adult male and female lifespan.
Materials and methods
Study design and population
The study was a retrospective analysis of previously collected, coded archival data. The data comprised an identifier, age and gender together with the results of assays performed over seven years (2007–2013) on consecutive blood samples collected from patients referred to a large urban commercial pathology laboratory. The Melbourne-based laboratory provides private sector pathology services to community-based general practitioners and specialists throughout the city of Melbourne and central Victoria. The state of Victoria, representing about 25% of the Australian population, is representative of the national population in demographic characteristics (see http://www.stat.abs.gov.au/itt/r.jsp?databyregion#/).
The study was initiated only after at least a year had passed since all test results had been provided by the pathology laboratory to the referring doctor. No other personal, demographic, anthropometric or medical information of the patients were available for analysis. No new individual health information could be generated by this present re-analysis of non-identifiable coded information. As a result, neither ethics approval nor individual patient consent was required for this archival data analysis.
Assays
The laboratory's standard operating procedure was for all samples requesting serum testosterone to have serum SHBG and albumin measured concurrently. Serum samples were stored frozen until assay usually within one to two days of collection. Serum testosterone and SHBG were measured on the Roche E170 modular analytics immunoanalyser, a high volume throughput multiplex platform supporting electrochemiluminescence-based immunoassays. 11 The limit of detection of the serum testosterone immunoassay was 0.4 nmol/L and for serum SHBG 1 nmol/L. Serum albumin was measured by the Roche Bromcresol Green method on a Roche c701 analyser. Assay methodology did not change during the study period and was routinely within acceptable limits by a national external quality assurance scheme. Free testosterone was calculated using an empirical equation (FTZ) which was validated in two large studies involving over 6000 specimens against the laboratory measurement by equilibrium dialysis, the standard reference method.12–14
Data analysis
Data were analysed to derive smoothed centiles using the General Additive Model for Location, Scale and Shape (GAMLSS, http://www.gamlss.org/), an approach originally developed by Cole for paediatric growth charts,15,16 incorporating the non-parametric method of quantile regression developed in econometrics, 17 and implemented in modified form using R software by Rigby and Stasinopoulos.18,19 Briefly, the model fits four parameters (µ, σ, ν, τ) which, together with the explanatory variable of age, define the location (µ, median), scale (σ, spread) and uses a Box-Cox exponential power transformation to reduce asymmetry (ν, skewness) and kurtosis (τ, power exponential parameter) of the distribution. Smooth centile curves are obtained by modelling each of the four parameters of the distribution as a smooth non-parametric function of age using penalized splines for weighting and automatic smoothing parameter selection. 19 Using the raw data, smoothed centiles (1, 2.5, 5 10, 25, 50, 75, 90, 95, 97.5 and 99) for the age-specific distribution of the serum testosterone, SHBG and FTZ were estimated for males and female separately. Data with undetectable T or SHBG were deleted from the analysis. Furthermore, to reduce any hypothetical impact of biological or analytical outliers, smoothed centiles of distributions were also estimated using data trimmed by 1%, 2% and 5% in the uppermost and lowermost distribution. Preliminary analysis and sensitivity estimates resulted in defining the 2% trim (i.e. 4% of samples overall deleted) as optimal and was used for further robust analysis. The smoothed central centiles, representing the quartiles (25%, 50% = median, 75%) were also fitted to polynomial equations using TableCurve 2D (Systat Software, San Jose, CA) to derive parametric function to describe the centile curves. Among over 4000 formulae automatically fitted and ranked according to goodness of fit, we selected the best parsimonious fit according to the hierarchical criteria (1) r 2 >0.99, (2) fewest coefficients required and (3) acceptable visual fit to the data.
Results
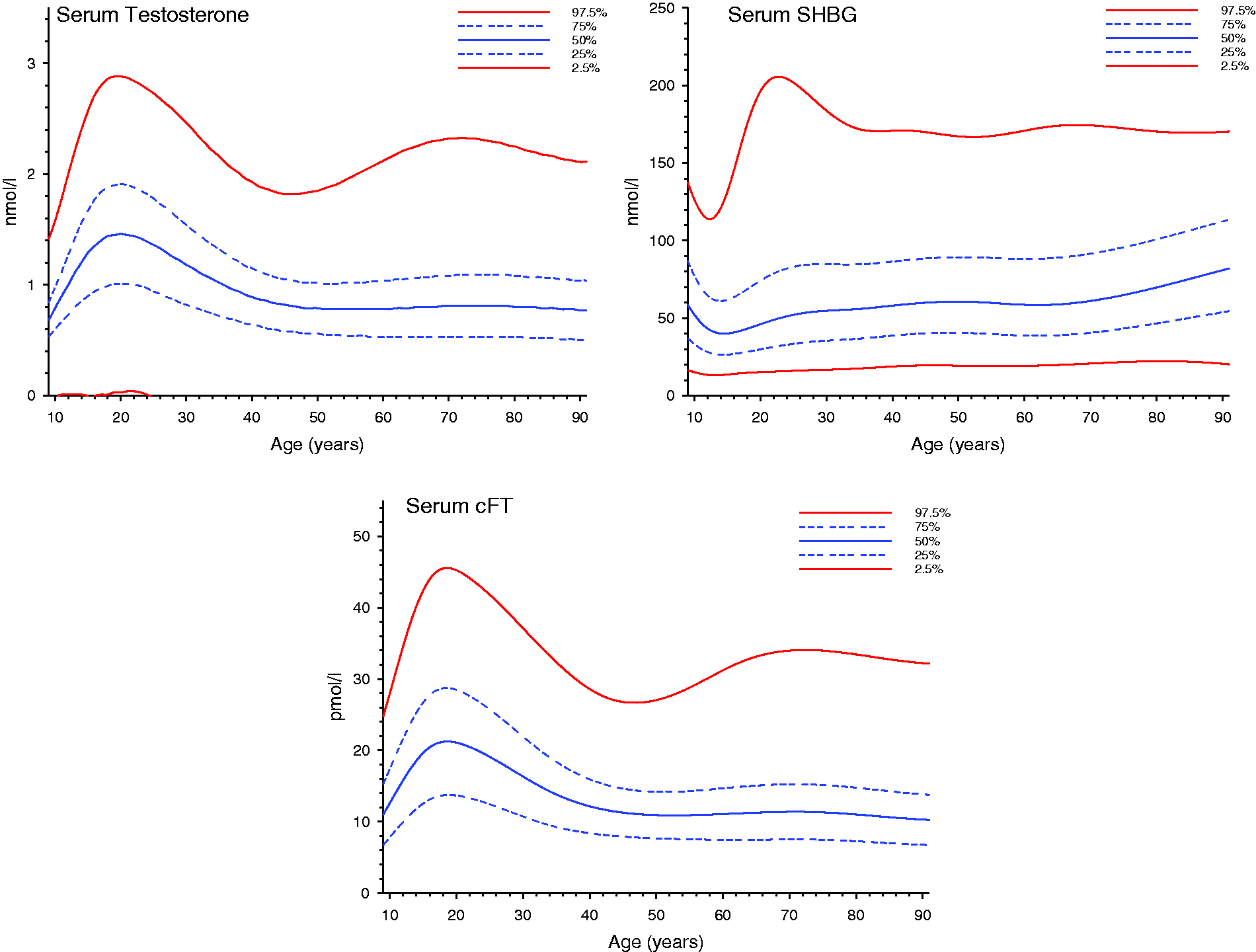
Data comprised results from 123,572 consecutive blood samples requesting serum testosterone measurement. Samples from females comprised 50.5% of samples (n = 62,441, mean age 36.3 (SD 13.2, range 0–97 years; male n = 61,131, 53.3 (17), 0–99 years). From the full dataset, 110,967 samples (90%) had detectable (>0.4 nmol/L) serum testosterone. Most undetectable serum testosterone samples came from females (9849, 78% of undetectable, 8% of all samples) with a near-Gaussian unimodal age distribution across the whole dataset (data not shown). The remaining minority of undetectable serum testosterone samples came from males (2756, 22% of undetectable, 2% of all samples) and were distributed in a bimodal fashion according to age, with the majority in a near-Gaussian distribution from males 60 years of age and older with a second, much smaller and skewed distribution below the age of 15 years. There were 18 samples (12 female, 6 male) with undetectable SHBG (< 1 nmol/L) that were deleted from further analysis. Similarly, sparse data from children < 10 years of age (19 female, 10 male) and over the age of 90 years (8 females, 202 male) were deleted. Final analyses were undertaken on all samples with detectable serum testosterone, SHBG and cFT (110,712 samples, 90% of all samples) depicting the smoothed centile distributions for males (Figure 1) and females (Figure 2).
Smoothed centile plots of circulating testosterone (left panel), SHBG (middle panel) and cFT (right panel) in males plotted for each year of age at centiles 2.5%, 25%, 50% (median), 75% and 97.5%. The median plot is a solid [blue] line, 25% and 75% in broken [blue] lines, and 2.5% and 97.5% in solid [red] lines. Note the scale of testosterone measurements is higher than in females. Smoothed centile plots of circulating testosterone (left panel), SHBG (middle panel) and cFT (right panel) in females plotted for each year of age at centiles 2.5%, 25%, 50% (median), 75% and 97.5%. The median plot is a solid [blue] line, 25% and 75% in broken [blue] lines, and 2.5% and 97.5% in solid [red] lines. Note the scale of testosterone measurements is lower than in males.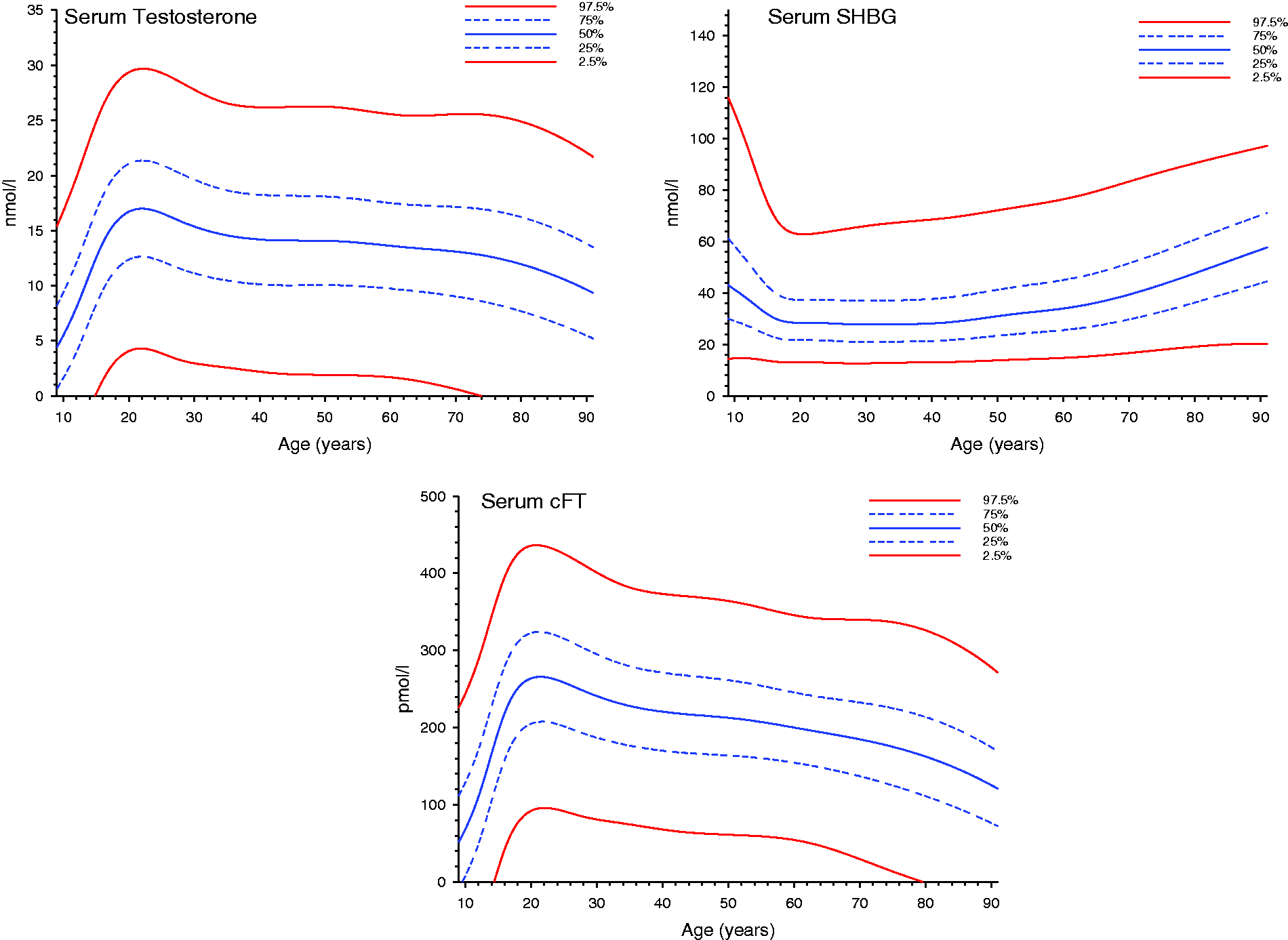
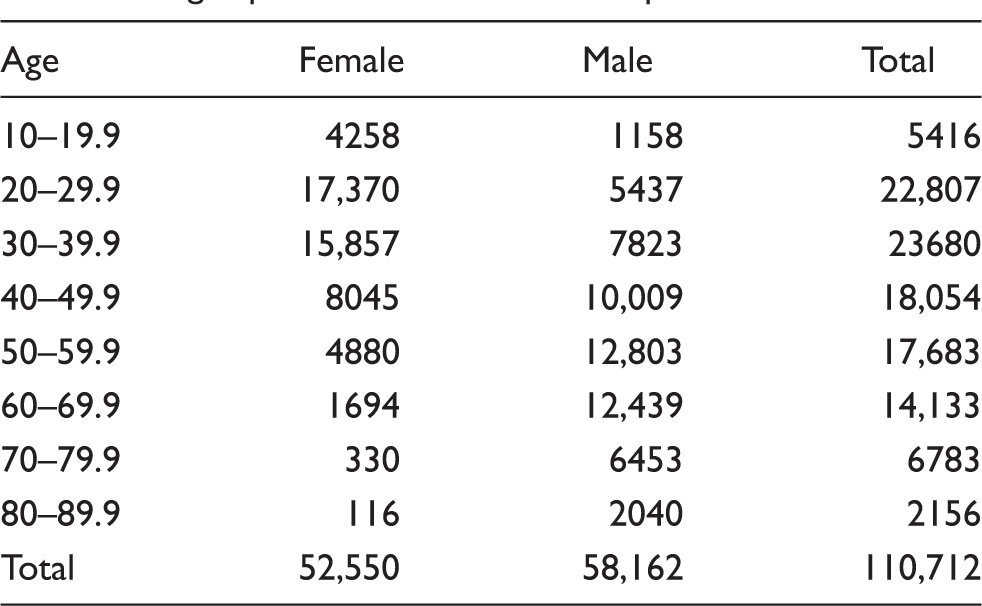
Age-specific distribution of samples.
The smoothed central centiles (75%, 50% = median, 25%) were fitted to polynomial equations as shown in supplementary Figures 1 (male) and 2 (female) with the coefficients shown in supplementary Table 1.
Discussion
This study presents the first comprehensive profile of serum testosterone, SHBG and cFT in males and females across the adult age spectrum from early adolescence to late old age (10–90 years). It uses a consistent assay methodology in a single laboratory based on results from over 100,000 consecutive blood samples. For analysis of this large dataset, we utilized the versatile GAMLSS modelling framework to provide smoothed age-specific centiles. Based on the normalizing Box-Cox transformation18,19 and the non-parametric method of quantile regression, 17 our application is analogous to that used to construct age-specific paediatric growth curves, which led to the development of this methodology.15,16
An important consideration for the validity of this analysis is that the dataset is derived from serum testosterone assays ordered from routine clinical practice rather than a deliberately population representative sample. Given the goal to describe age-specific trends in the general population, several steps have been taken to minimize bias in estimating centiles arising from that data source, a bias most likely to be evident at the extremes. Samples from patients with genuine reproductive system pathology, however, only represent a small proportion of all samples so that they have minimal impact on the large-sample estimates of central centiles we have derived. This is because blood testosterone measurement is available without cost to the patient or doctor ordering the test under the Australian national health scheme. Easy access at negligible cost has fostered the application of testosterone assays, mainly by non-specialists, to rule out reproductive pathology in males and females of all ages. Although the prior diagnostic probability for uncommon reproductive disorders is low, concern about medico-legal risk from missing a diagnosis of treatable reproductive tract disorders constitutes a strong incentive towards a defensive screening of patients for possibly unrecognized pathology by non-specialists with limited experience of uncommon reproductive disorders. This medico-legal imperative together with negligible cost and access disincentives has promoted a de facto standard of care of population screening using serum testosterone assays. As most tests prove to have normal findings which dispel the risk of missed diagnosis, these findings are then discarded; however, this analysis shows that such aggregate data may provide coherent and useful insight into the health status of the general population including reasonable estimates of population age-specific trends for people without reproductive system pathology, despite its origins based on requested pathology tests.
The validity of this approach is reinforced by the low proportion of the general population affected by reproductive system pathology. Whereas ∼5% of males have male infertility due to defects in spermatogenesis, circulating testosterone is usually unaffected. 20 Furthermore, only 0.5% of the male population have pathologically based androgen deficiency 1 and among the general male population <1% have ever been (including currently) treated with testosterone. 21 For females, polycystic ovarian syndrome is relatively common affecting 5–10% of females of reproductive age with serum testosterone measured for clinical diagnosis.4,22 Only a small minority of menopausal females are treated off-label with testosterone to improve oestrogen-resistant menopausal symptoms; 23 however, the already low prevalence of such testosterone treatment declined further following the failure of placebo-controlled clinical trials of testosterone to achieve marketing together with the impact of WHI in reducing all postmenopausal hormone replacement. 24 Considering these issues, to ensure a more robust analysis free from undue influence of clinical and/or analytical outliers, we used a 2% trimmed dataset (i.e. removing the upper 2% and lower 2% of data, so that a total of an unbiased 4% of samples were removed) to eliminate extreme outliers. The trim fraction used was calibrated to match or exceed plausible estimates of the proportions of people with reproductive system pathology that might impact on circulating testosterone. Hence, it is plausible that the sampling framework used would provide at least central centiles as reasonably representative of the general male and female population without undue influence from people with reproductive system disorders. All attempts to derive representative population-based reference ranges are flawed. For example, cross-sectional studies, even if drawn from population-based sources, typically have incomplete participation which creates participation bias. Furthermore, longitudinal studies (which originate as cross-sectional) suffer additionally from drop-outs from the inception cohort as well as healthy survivor bias. In this novel alternative approach to extract population representative data from a large dataset, it is also likely to have inherent bias especially at upper and lower end of the distribution. Our approach minimizes these influences so that at least the central centiles are likely to be valid population estimates. However, as it is impossible to eradicate residual bias especially at the extremes of the distribution, the present estimates should be considered as depicting age-specific trends and not population-representative reference ranges. In addition, the large sample provides convenient empirical equations to model the age-dependence of serum T, cFT and SHBG in males and females across all ages, which may have utility in modelling androgen status in males and females, in derivation of power and sample size estimate for clinical trials as well as for covariate adjustment for smaller sample size studies.
The present analysis was focused on a sample rather than an individual level of analysis so some individuals were sampled more than once for this study. In routine clinical reproductive medicine practice, measurements of serum testosterone are usually required for diagnosis and only measured repeatedly in a small minority. The conventional recommendation for males to have two measurements of serum testosterone for primary clinical evaluation, 25 explains the higher proportion of males having two rather than a single sample in the analytical sample for this study. Furthermore, a re-analysis based on a per-person rather than a per-sample analysis, with its reduced power, produced essentially identical patterns of age-specific centiles.
The deduced age profiles replicate previously established trends demonstrated in smaller and/or more age-restricted studies as well as some novel findings. Among the novel findings is the peak of circulating testosterone around the age of 20 years in females as well as in males with decline over the next two decades. This early adult peak may explain some discrepancies between previous studies of circulating testosterone in male ageing according to how much of the younger age groups are included; for example, the higher mean testosterone among males under the age of 40 years 26 than among those above 40 years old. 27 The minimal decline in serum testosterone between the ages of 35 and 65 years is also striking and consistent with some 27 but not other previous studies28–30 which report various degrees of decline in serum testosterone with advancing male age. Only after the age of 80 years is there a more pronounced, definite decline in circulating testosterone, consistent with many other studies (reviewed in Kaufman and Vermeulen 31 ), consistent with the impact of cumulative effects of the co-morbidities of male ageing rather than age itself. 27 Analogous findings were recently reported from a compilation of data from 13 different studies showing a negligible decline but increased variability in serum T with age until the late 80s. 32 The increased variability in serum T in that study may reflect an analytical limitation that all but two studies used direct (non-extraction) T immunoassays so that a linear interpolation was used to estimate MS-equivalent serum T levels for immunoassays. However, serum T concentrations measured by direct immunoassay deviate from MS measurements in non-linear fashion26,33,34 especially at the lower serum T concentration levels characteristic of males over the age of 65 years. Hence, the increased variability at older ages rather than the consistent decline we report may be due to inaccurate re-calibration of serum T concentrations from data of direct T immunoassays.
In females, circulating testosterone peaks at age 20 years followed by a marked decline over the next two decades, remaining stable thereafter. This is consistent with the reported decline in serum testosterone between the ages of 20 and 40 coinciding with the age-related decline in adrenal androgen (DHEA) secretion, rather than during the menopausal transition 35 as formerly believed. 36
In these data, serum SHBG in males declines to a nadir at about the age of 20 years to remain stable until undergoing a gradual, progressive rise from the sixth decade onwards. In females, the SHBG nadir is reached earlier, in late adolescence, with median levels rising progressively with age thereafter with an acceleration after the age of 70 years. In addition, females exhibit a serum SHBG peak, confined to the higher centiles, during the early half of reproductive life due to the minority at any one time who are pregnant or using oral contraceptives, both of which markedly increase serum SHBG. The confinement to the upper centiles confirms the stability of the other deduced more central centiles. As expected, cFT estimates reflect the findings of circulating testosterone in males and females. The interpretation of this derived measure, even using a formula which corresponds to the reference equilibrium dialysis method,13,14 is dubious as many assumptions of the free hormone hypothesis remain largely untested or are either implausible, unfulfilled or refuted.
A limitation of this study is its reliance on direct testosterone immunoassays which are inaccurate when compared with mass spectrometry-based measurements, especially with low circulating testosterone levels such as in females and children as well as hypogonadal and very old males. 34 A further limitation is that this analysis used calculated rather than direct measurement of free testosterone by equilibrium dialysis. The laborious reference method, however, was not feasible for the routine pathology laboratory that provided this data retrospectively. Nevertheless, our empirical formula is well validated against the reference method in two studies involving over 6000 samples13,14 and is more accurate than the widely used equilibrium-binding equation formulae.37–39 It cannot be excluded that the single SHBG assay used in this study may also differ quantitatively from other SHBG immunoassays or rare SHBG genetic polymorphisms; 40 nevertheless, the age-dependent patterns are not likely to be materially altered by such systematic differences, if they exist.
A potential bias arising from the limited sensitivity of the testosterone immunoassay is the occurrence of undetectable serum testosterone values. This predominantly affected females whereby 78% of undetectable samples (8% of all samples) were from females. However, as this had a unimodal distribution across ages, it is plausible that this represents a random rather than a systematic error. The net effect of undetectable serum testosterone concentrations would be to overestimate the testosterone centiles; however, if this is a random error it would not distort the age-specific patterns which are the focus of this analysis. Furthermore, the magnitude of this upward bias appears to be small, presumably because the undetectable serum testosterone concentrations are so low. For example, using the upper 99th and 97.5th centiles from our data for specific age ranges (data not shown), the upper 99% centiles for females aged 23–30 years in the present study (3.01 nmol/L) were very close to the 99% confidence intervals of elite female athletes of similar age (3.08 nmol/L) estimated by mass spectrometry-based methods. 41 Similarly, the upper 97.5% centiles for females aged 20–30 and 40–50 years in the present study (2.69 nmol/L and 1.85 nmol/L) were comparable with those from a large population-based study of 985 German females (2.12 and 2.00 nmol/L). In addition, menstrual cycle variation with a small ovulatory peak in serum testosterone is quantitatively minimal42,43 and, as samples were collected without regard to menstrual stage, this would represent a source of random rather than systematic error.
In males, undetectable testosterone levels occurred in only 2% of all samples arising from two widely different age groups but these are unlikely to affect the centile estimates as they would have been eliminated by the data trimming. The majority of these samples were from older males who may have undergone therapeutic castration for prostate cancer or suffered from systemic disorders which cause a severe reduction in circulating testosterone. The remaining minority were from pre-pubertal boys although even among boys between 1 and 15 years of age, 60% had measurable serum testosterone. Again the small proportion of samples involved and the trimming make it likely that the central age-specific centiles are unlikely to have been distorted. A further potential limitation of this study is that it is impossible to separate age effects from potentially confounding period or cohort effects, which are inevitably collinear with age. 44 In this context it is notable that a temporal downward trend in age-specific serum testosterone has been reported in US 45 and Danish 46 populations. In these studies the temporal effects may reflect period and/or cohort effects of, for example, residual confounding despite attempts to eliminate temporal changes in assay methodology and/or increasing population prevalence of obesity, which lower serum testosterone. 47
We conclude that these routinely disregarded apparently normal hormonal data arising from routine clinical practice and pathology may be employed to deduce comprehensive temporal trends across the full adult age spectrum in males and females in the general community. Despite their origins in routine clinical testing, our methodology makes it realistic to infer general population trends undistorted by the presence of uncommon reproductive system disorders. Nevertheless, as it is impossible to exclude that the specific centile values may still be influenced by residual bias arising from the nature of the dataset, the age-specific patterns revealed may best be considered to reflect age-specific population trends without constituting population representative reference ranges.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
Not applicable.
Guarantor
DJH.
Contributorship
DJH designed, directed data analysis, drafted manuscript. KS contributed to design, provided the coded data for analysis and reviewed manuscript. LPL performed the data analysis and reviewed manuscript.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.