
Abstract
The use of doping agents is evident within competitive sport in senior and junior age groups, where they are taken by non-elite as well as elite participants. They are also taken in non-sporting contexts by individuals seeking to ‘improve’ their physique through an increase in muscle and/or decrease in fat mass. While attaining accurate data on the prevalence of their use has limitations, studies suggest the illicit use of doping agents by athletes and non-athletes may be 1–5% in the population and greater than 50% in some groups; with the prevalence being higher in males. There is conclusive evidence that some doping agents are anabolic and ergogenic. There is also evidence that the use of doping agents such as anabolic androgenic steroids, growth hormone and other anabolic agents, erythropoietin and stimulants conveys considerable health risks that include, but are not limited to: cardiovascular disease, diabetes, cancer, mental health issues, virilisation in females and the suppression of naturally produced androgens in males. This review will outline the anabolic, ergogenic and health impacts of selected doping agents and methods that may be used in both the sporting and physique development contexts. It also provides a brief tabulated overview of the history of doping and how doping agents may impact upon the analyses of clinical samples.
Introduction
Sport and physical activity are widely encouraged by governments and health authorities for their perceived benefits to health and quality of life. Conversely, illicit drug use is deemed to have a negative impact on health and adversely affect society. However, since some drugs are known to augment physical performance and adaptations to exercise training, these two contrasting areas can intersect.
In sport the use of illicit drugs comes under the category of ‘doping’ with the relevant sports governing bodies pursuing strategies to prevent the use of banned substances. Doping is used in sport and exercise contexts for a number of reasons, including the desire to win and to improve aesthetic appearance. Sports are governed by rules and codes, including those relating to the prohibition of doping. Perhaps the most well known of these is the ‘World Anti-Doping Code’,
1
which is implemented by the World Anti-Doping Agency (WADA) and WADA publishes a list of prohibited substances and prohibited methods.
2
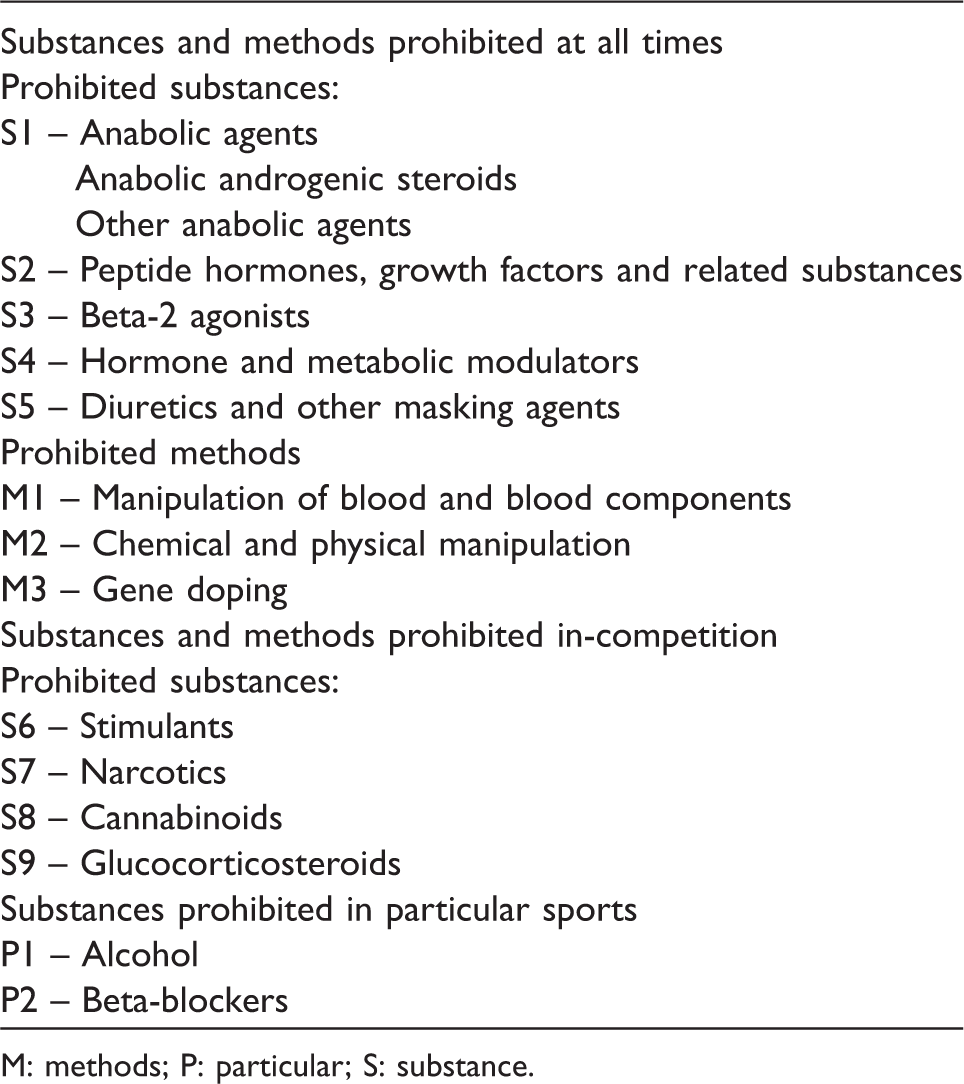
Doping substances and methods are included on the WADA prohibited list if they meet two of the following three criteria:
3
Evidence that it has the potential to enhance sport performance; Use of the substance or method represents a health risk; Use of the substance or method violates the spirit of the sport. A summary of the world antidoping agency antidoping code and doping categories. M: methods; P: particular; S: substance.
The WADA list clusters its doping categories into: ‘Substances and Methods Prohibited at All Times (in- and out-of competition)’; ‘Substances and Methods Prohibited In-Competition’ and ‘Substances Prohibited in Particular Sports’ (Table 1). As a broad generalisation for this distinction the ‘Substances and Methods Prohibited at All Times (in- and out-of competition)’ have potential benefits in terms of enhancing adaptation to training and either directly to or as a consequence of these augmented adaptations to improve performance in competition. Whereas ‘Substances and Methods Prohibited In-Competition’ are likely to enhance the immediate short-term performance of the body by augmenting its ability to meet the demands of the exercise and thereby perform better. Furthermore, some substances are prohibited under the WADA code in ‘Particular Sports’ if they convey benefits or hazards in specific sports but not others, such as alcohol in motor sports. WADA publishes a list of sport organisations and countries who comply with the WADA antidoping code and are subject to WADA testing.
4
However, it should be noted that many professional sports such as the National Football League (American Football/Gridiron),
5
some boxing federations and many body-building type sports do not comply fully with the WADA code and its antidoping regulations.
In the wider context, the use of such drugs extends beyond regulated elite sport, into lower competitions and younger age groups, as well as occurring outside of the sporting context, where they may be used to enhance the development of a person's physique for reasons of aesthetics and physical presence. 6 Consequently, the health issues associated with the use of such drugs permeate society beyond the sporting elite. Additionally, not all ergogenics are banned from sport, examples being caffeine, creatine and bicarbonate, all of which have strong research evidence for their efficacy.7–11 This review will briefly present some of the key events in the history of doping, consider current doping prevalence and then review the performance and health issues of the WADA doping categories.
Methods for literature review
The published scientific literature was searched using key words in databases, primarily Pubmed. Additionally, literature and documents were searched from key sites, such as the WADA. To ensure currency of data and information, those articles published within the last 10 years were preferentially referred to over older publications. When the identified literature referred to a key publication that had not been identified in our searches this article was located directly, likewise where the original search had been refined to reviews, key original data articles cited in the reviews were downloaded. Where applicable, confirmed examples were sought from the popular press.
For note, the nomenclature and level of detail applied to peptide hormones in the published literature varied based on the context of the information provided. Within this review when discussing the use of various hormones, such as erythropoietin (EPO), growth hormone (hGH), luteinising hormone (LH) and chorionic gonadotrophin (CG), the prefix ‘h’ indicates the ‘human’ form of the hormone and ‘r’ indicates the recombinant synthetic version, with ‘rh’ indicating a recombinant version of the human form. Hence the terminology may vary in places depending on the specific form of the hormone being discussed and the information provided in the source material.
The physiological basis for doping in sport and exercise
Sport and exercise initiate both short-term acute responses and longer term adaptations. The short-term acute responses include elevations in heart rate and cardiac output, redistribution of blood flow, increased pulmonary ventilation and endocrinological responses. These responses enhance the body's ability to cope with the immediate demands of the current exercise bout, for example through the facilitation of oxygen delivery and its utilisation by the muscles. The longer term adaptations, such as structural and physiological changes to the skeletal musculature, cardiovascular system and haematology, enhance the body's ability to cope with the demands of subsequent exercise, for example through an increased capacity to deliver and utilise oxygen or an increase in contractile proteins of the muscle that thereby increase the amount of force that they can exert. Such adaptations would be seen as improvements in ‘fitness’ and enable the person to potentially achieve a higher level of performance in subsequent exercise bouts or events.
Doping is used to augment these responses and adaptations, thereby elevating what the person can achieve to a level above that attainable by training alone. Due to the specific demands of each sport, the prevalence of different drugs and doping procedures will differ accordingly, as they are used to target specific aspects of the fitness needed by the performer in that particular activity. Additionally, as previously indicated, some doping practises are used specifically to enhance the physique of an individual, often to gain muscle mass and/or lose body fat: and while for sports performers such outcomes may benefit their strength, power and endurance, for others it is the enhanced physique that is the primary objective.
A brief history of doping in sport
Historically, the second half of the 19th century saw the start of what has become the epidemic problem of doping in sport and exercise at all levels of competition. In the first half of the 20th century (up until the end of World War II), doping expanded with programmes aimed at the individual and administration controlled by the athlete themselves or by their coach or doctor. Doping at this time was generally confined to the elite level of sport. Post-World War II, doping expanded significantly with systemic team doping programmes emerging. In response to the increased incidence and adverse outcomes, doping controls were first introduced in the late 1960s; partly due to the outcry resulting from the first televised doping-related death.
Sport-related drug use has significantly influenced competition since the mid-20th century. The 1960s and 70s saw the wide use of amphetamines in sport; the 1980s has been described as the anabolic steroid and cortisone era; the 1990s as the hGH and EPO era; and more recently, the use of peptides has become widespread. Today we generically classify such performance-enhancing drugs according to terms such as ‘anabolics’ and ‘stimulants’ to describe the general desired effect of their administration.
With doping control, comes the introduction of drugs to ‘cheat’ the system. The reported instance of evasive measures became prevalent after the 1980s when the first assay to detect testosterone in urine was developed. Despite these control measures and awareness of the risks of sport-related drug use, doping in sport remains endemic; transgressing all levels of activity.
A brief summary of the history of doping in sport.

The prevalence of doping
Sport-related drug use
The prevalence of doping can be indicated through surveys or by the testing of participants, but both methods have inherent problems. For example, survey data have limitations relating to differences in the definitions of doping and the taking of ‘banned’ substances for social rather than performance-enhancing reasons, as well as a reliance upon honest self-reporting of an illicit activity. 13 Whereas data based on the clinical testing of blood or urine samples may underestimate the prevalence of doping if the timing of the sample collection does not coincide with the window of time when a substance or its metabolites are present within the sample.
While the highly publicised cases highlighted above create awareness through the media, quantifying the actual prevalence of sport-related drug use is more problematic and incurs the aforementioned limitations. However, as an initial indication, WADA reports the results of 269,878 samples analysed in 2013, of which 5962 (2.21%) indicated either an ‘adverse analytical finding’ or ‘atypical finding’.
14
Of these: 63.0% were due to anabolic agents; 10.1% stimulants; 7.5% diuretics and other masking agents; 6.3% glucocorticosteroids; 3.8% peptide hormones, growth factors and related substances; and 3.6% cannabinoids; with all other categories contributing <3% to the total adverse/atypical findings and their combined total being about 6% of all adverse or atypical results (Figure 1). The relatively recent introduction of testing blood samples has added to these results with a study that included the samples of 2737 international track and field athletes, mainly endurance athletes, from whom blood samples were collected indicating the prevalence of blood doping (any method that increases red cell mass and enhances oxygen transport) to be 14%, but with considerable variation in prevalence between nationalities.
15
Prevalence of sport-related drug use.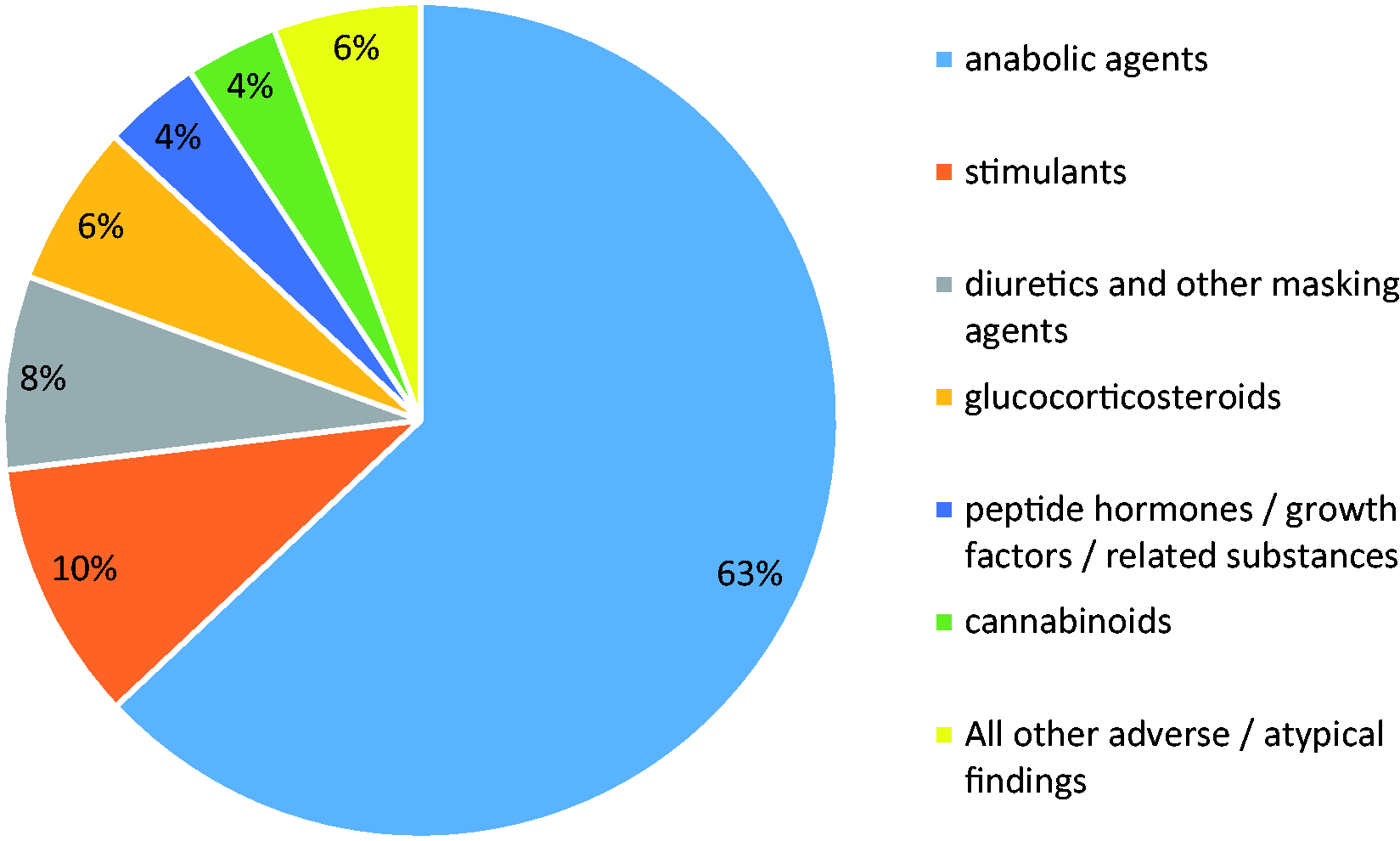
Doping violations have also been reported in Paralympic sport, albeit with a relatively low prevalence of <1% and when such violations are detected it is most commonly for anabolic agents, with sports such as powerlifting having the highest prevalence. 16 At lower levels of sport the reported prevalence includes: 43% anabolic androgenic steroids (AAS) and 12% hGH or insulin-like growth factor (IGF-1) in young male weightlifters. 17 Indeed it is suggested that 4–6% of adolescent male athletes and 1.5–3.0% of adolescent female athletes will have used AAS at some time. 18
Non-sport-related drug use
In addition to sport-specific doping, social drug use is also evident among athletes, and an Italian study indicated that 18% of all positive results were for cannabis and 7% for cocaine which while constituting a positive test, were likely to be cases of social drug use rather than for performance-enhancing purposes. 19 In May 2013, the WADA raised the in-competition threshold for marijuana (cannabis) 10-fold to 150 ng/mL to avoid such use being included as a doping offence. 20 Likewise, the results from a study that questioned members and junior members of German national teams from 43 different sports, indicated a 7% prevalence of illicit drug use, and a study of over 2000 German adolescents, in which 15.1% indicated that they had used a WADA banned substance, cannabis was the most prevalent (13.2%), 21 followed by stimulants (2.4%), cocaine/heroin (2.2%) and AAS (0.7%). 22
What is also evident from other studies is that the use of doping agents is not confined to those involved in competitive sport but are also used for aesthetic reasons and ‘body styling’ in young and adult males and females, notably for the aforementioned increase in muscle mass and/or fat reduction, with AAS being the most common drugs used.23–27 With scenarios such as the seizure of millions of doses of steroids and hGH by the US Drug Enforcement agency further indicating a widespread illicit use of doping agents. 23 Indeed, a Swedish study indicated that the use of AAS was more prevalent in society than in regulated sport and the use among Swedish high school pupils has been reported as 2.7% in males and 0.4% in females.28,29 This concurs with other studies in which prevalence rates for high-school-aged students range between 1 and 3% across several countries. 30 Similar prevalence rates have been reported for tertiary education students from six developed countries, with a higher usage by males compared to females. 31 Furthermore, studies indicate a 3–11% use in US high school students, 4–12% in US male adolescents and up to 2% in young US women, 32 and use by around 3% of young males in many ‘western’ countries,33,34 with their use being more prevalent among body builders and weightlifters (3–5%).33,34 AAS use has even been reported in younger age groups such as adolescent boys (1.7%) and girls (1.4%), as well as preadolescents where the prevalence was 1.2–3.0%. 35 At the other end of the age spectrum, the therapeutic prescription of AAS and related anabolic agents have the potential to benefit older adults through their antiageing properties, such as the prevention of sarcopaenia and, as a consequence, they are also taken illicitly by some adults without medical supervision for their perceived physical enhancement. 30
The illicit access to these drugs by both those involved in competitive sport and those seeking physical enhancement for aesthetic reasons appears to be through a combination of: physicians, pharmacies (both with and without the required prescription), fellow gym users, external suppliers and the internet. 24 Indeed some studies indicate that more than 50% of AAS users in some groups acquire their drugs through physicians. 24
It is also interesting to note that a number of studies have reported an association between the use of sport performance/physique-enhancing doping agents and other risk behaviours, such as increased alcohol intake and use of recreational drugs such as cannabis and cocaine. 36 Additionally, other studies have found an increased likelihood of adolescents using AAS to smoke, shared needles, possess a weapon and exhibit suicidal behaviour, all of which result in further health risks. 37
Review of doping categories: Their effects on physique, performance and health
S1 – Anabolic agents
This category includes: AAS and other anabolic agents such as selective androgen receptor modulators (SARMs).
AAS
Anabolic and ergogenic properties
AASs are synthetic derivatives of the hormone testosterone, which is also included in this category and is the most prevalent AAS. Other commonly used AAS include: nandrolone decanoate, methandienone, stanozolol, androsterone and androstane. 38 AASs are primarily used to increase muscle mass and as a consequence are associated with activities that require strength and high levels of peak power, such as weightlifting, throwing events and sprinting. They are also used by those seeking to increase muscle mass per se, which includes those seeking to attain a greater musculature and physical presence, as well as competitive body builders. Additionally, their use is known to extend to endurance athletes and cyclists who use AAS in smaller doses to increase red blood cell mass and haematocrit, which may augment oxygen delivery and utilisation, as well as aiding recovery. 39 Furthermore, the reported psychotrophic effects of AAS include the elevation of mood, determination and aggression, all of which may aid in training and competition, but may result in psychological health problems as well as inappropriate and undesirable behaviour in social as well as sporting contexts. 40
The anabolic properties of AAS promote increases in muscle mass and aid recovery, while the androgenic properties promote masculinisation, which has particular health implications when taken by females due to their virilising effects. The production of endogenous testosterone is 20–30 times higher in males than females, which results in males having around a 10-fold greater blood testosterone concentration. 40 Hence it could be suggested that in terms of gains in muscle mass and strength, females have the capacity to gain a greater relative increase from AAS use than males: a feature that was evidently exploited in the GDR doping programme.
AAS may be taken orally, via intramuscular injections or through topical gels and creams. The use of AAS as a doping agent involves doses that are considerably greater than those prescribed medically for therapeutic purposes, which has implications for research studies in which the use of therapeutic doses are unlikely to produce the performance benefits of the supraphysiological doses taken by athletes. 30 Hence many early studies failed to detect performance benefits, whereas more recent studies using supraphysiological doses provide evidence for their effects in enhancing muscle mass and strength.
As previously indicated, AASs are used by individuals seeking to become more muscular for aesthetic rather than sport performance goals and here their potential effectiveness is unequivocal. 41 However, while increases in muscle strength and aerobic capacity are evident, what is less certain is the extent to which these translate into improvements in performance, but the lack of unequivocal evidence may be due to the ethical and research design issues associated with undertaking double-blind clinical trials of a banned substance on competitive sportsmen and women. 40 Indeed, the prevalence of AAS use in these groups, despite their use being banned and the reported health risks, would suggest a belief in their effectiveness among elite sportsmen and women.
Health risks
As indicated above, doping practices use doses of AAS that are considerably greater than those prescribed therapeutically; consequently, many of the elevated health issues associated with doping are due to these supraphysiological intakes. AASs use has been associated with adverse effects upon the cardiovascular system, liver, kidney, endocrinological and reproductive systems. The cardiovascular health issues include elevated concentrations of low-density lipoprotein cholesterol and lower concentrations of high-density lipoprotein cholesterol (HDL-C); increased triglyceride concentrations,30,33,42–44 elevated systolic and diastolic blood pressure,42,43 which is reported in some studies but not others 45 ; endothelial dysfunction 46 ; increased concentration of clotting factors, thrombosis, 47 hyperinsulinaemia and reduced glucose tolerance30,43,47; left ventricular hypertrophy,42,43 cardiomyopathies,30,33 fibrosis and myocytolysis, 48 and polycythaemia. 49 Right as well as left ventricular function may be impaired, including slower diastolic velocities, 50 and there are reported cases of acute myocardial infarction and non-fatal and fatal ventricular arrhythmias.30,42,48,49,51 These aforementioned changes, which represent an increased risk of atherosclerosis and other cardiac pathologies may be evident for some time after AAS use has been discontinued and damage to vital organs may be permanent.23,42,45
AAS use is also associated with alterations to liver function, cholestatic jaundice, peliosis hepatis, hepatocellular hyperplasia and hepatocellular adenomas, with these changes being linked to the use of orally taken 17 α-alkylated AAS.30,44 Additionally there are reported increased risks of liver tumours with the death from hepatic carcinomas of some athletes being linked to AAS use.44,52 Similarly renal dysfunction and Wilms tumours have been reported in athletes using AAS.44,53
The adverse effects on the male reproductive system relate to the effects of exogenous AAS suppressing the hypothalamic–pituitary–testicular axis (HPT) and reducing the concentrations of the gonadotrophic hormones, LH and follicle-stimulating hormone, which ultimately reduces the concentrations of circulating endogenous testosterone. 43 There is also a reduction in sex hormone-binding globulin. 30 These endocrine changes are associated with reductions in testicular size, sperm count, sperm motility and changes to sperm morphology.30,44,54 However, in many cases these changes appear to be reversible upon cessation of AAS use. 33 In males there are also reports of prostatic hypertrophy, 55 and AAS use is also associated with gynaecomastia, due to the peripheral conversion of androgens to estradiol and estrone. 44 Indeed antiestrogenic drugs are taken by some AAS users to ameliorate this effect. 55
In females AAS use can result in menstrual abnormalities and virilisation, such as: deepening of the voice, breast shrinkage, male-pattern baldness, increased libido, acne, body hair and an increase in the size of the clitoris, with some of these changes not being reversible.30,44
Other effects in both males and females include the androgenic stimulation of the sebaceous glands, resulting in acne, which can be severe, affecting the face, back, shoulders and chest.44,56 Additionally, there have been reports of spontaneous subdural haematomas in weightlifters using AAS, which may have caused vascular changes that made the individuals vulnerable to these events when performing the valsalva manoeuvres while lifting. 57 Other physical consequences of AAS use may include an increased risk of tendon injuries, as some researchers suggest that the muscles may increase in strength disproportionately to the tendons, which then become vulnerable. 44 Case studies have also reported that AAS use in adolescents may cause premature epiphyseal closure of the growth plates in the long bones thereby preventing full stature being attained.30,44
Furthermore, AAS use has been associated with adverse mental health, including aggressive behaviour, commonly referred to as ‘roid rage’,44,58 and prior use of AAS has been associated with a two to fourfold increased risk of suicide in former athletes. 59 Other studies have suggested a link between the use of AAS and other health behaviours, such as high alcohol intake and the use of illicit recreational drugs. 60
Clinical implications
Potential effect on test results in clinical diagnostic laboratories.

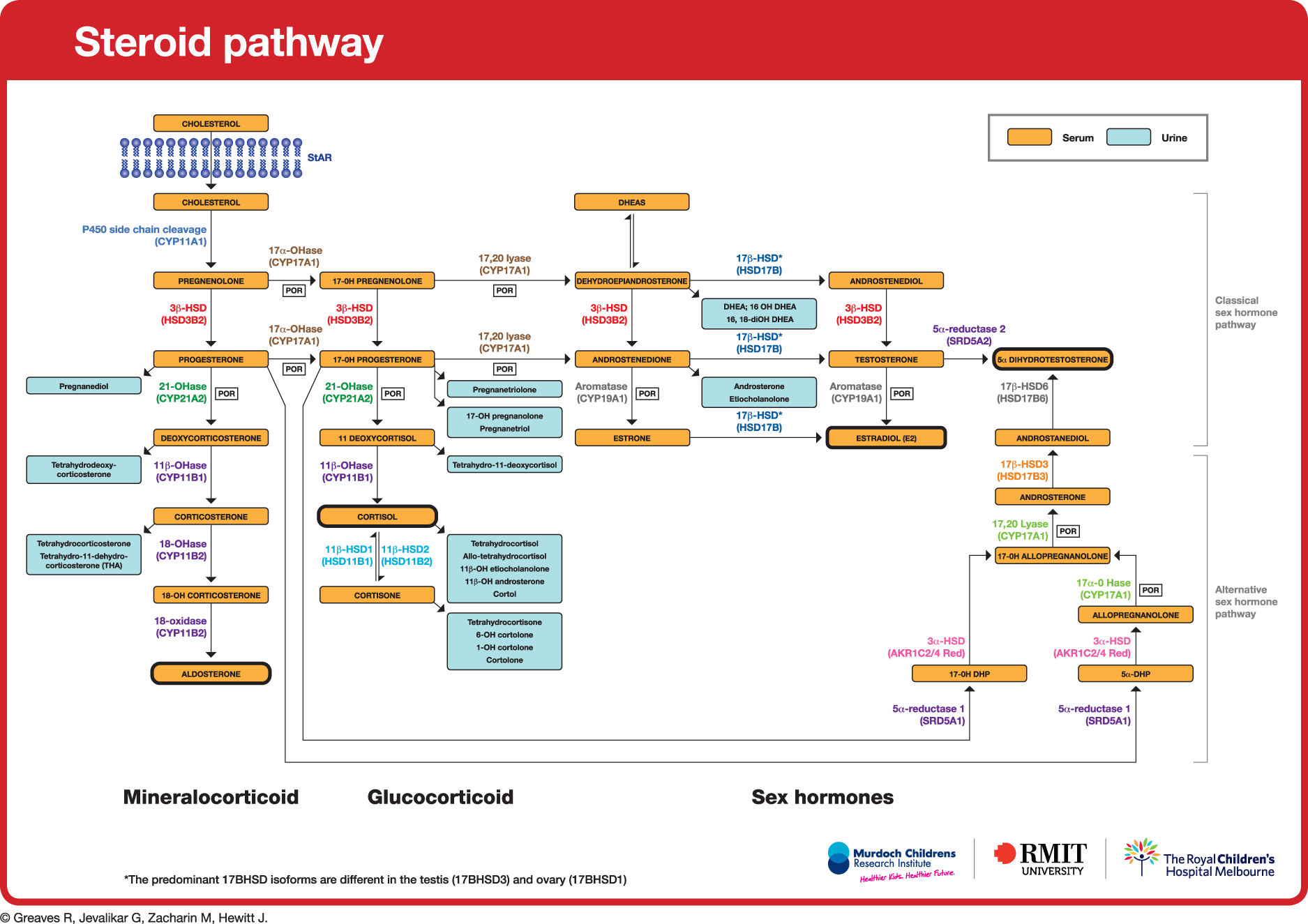
Endogenous steroid pathway providing a succinct overview of the relationship of steroid hormones to each other and the likely matrix for measurement (blood or urine) in the clinical diagnostic laboratory. 61
Case examples highlighting the dilemma occasionally faced by clinical diagnostic laboratories.

Other anabolic agents
Other anabolic agents include dehydroepiandrosterone (DHEA), which is secreted by the adrenal glands and is a precursor to testosterone. While it is reported to be taken by individuals seeking to enhance their muscle mass, research studies on its effectiveness in male athletes are equivocal. It is also taken for its suggested antiageing and antiobesity properties, but again its effectiveness remains unclear. 30 In females it appears to increase the circulating concentrations of testosterone and thereby increase the health issues associated with virilisation, including acne and hirsuitism, as well as reducing HDL-C, insulin sensitivity and glucose tolerance, 30 which have implications for increased risk of Type 2 diabetes. Through its influence on the concentration of circulating testosterone, the health risks associated with DHEA are accordingly those stated above for AAS. 55
SARMs are drugs that may be taken to enhance the action of the testosterone receptor,43-45 and thereby attain a greater anabolic effect. Clinical trial reports related to non-steroidal selective androgen receptors suggest that they are likely to induce the desired anabolic effects of circulating anabolic hormones, while minimising the often unwanted androgenic effects that present with AAS, such as the virilisation of females and feminisation of males. 65 To date the health issues associated with their use remain unclear. However, it is suggested that if they are taken without AAS, the individual may gain some hypertrophic benefits to the muscles, without incurring the aforementioned health risks associated with AAS use. This would be a result of the SARMs acting on the receptors within muscle and bone, but not affecting other organs such as the prostate or virilising other tissues. 23 Clenbuterol is another anabolic agent but is discussed under the category of beta 2 agonists.
S2 – Peptide hormones, growth factors and related substances
This category includes:
Erythropoiesis-stimulating agents, such EPO; CG and LH and their releasing factors in males; Corticotrophins and their releasing factors; Various growth factors, including but not limited to hGH and its releasing factors and IGF-1.
EPO
EPO is a glycoprotein hormone that is produced endogenously by the kidney and to a lesser extent (<10%) by the liver. 66 Its function is to promote the production of erythrocytes (erythropoiesis). Under normal aerobic exercise conditions, transient hypoxia is detected by cells within the kidney and liver, with a resultant increase in EPO production. This stimulates the proliferation and differentiation of erythroid precursor cells in the bone marrow and results in the postexercise generation of additional erythrocytes. 23 In turn, this enhances the capacity to deliver oxygen to the exercising muscles in subsequent exercise sessions. With recombinant EPO (rhEPO) being developed and becoming available in recent decades, this training effect can be augmented pharmacologically, resulting in even greater red blood cell production and haemoglobin mass.
The detection of rhEPO use has been problematic, with both endogenous and rhEPO having the same amino acid sequence. However in some versions of rhEPO there are small differences in the side chains with rhEPO exhibiting fewer sialic acid residues due to glycosylation, although the recent increase and widespread production of rhEPO has resulted in other variations which further complicate the detection process. 67 Recent developments in antidoping strategies now include an athlete's ‘Biological Passport’. This requires a record to be kept of the results of several blood samples and new samples to be compared against the athlete's historical record. Experts evaluate the records to determine whether any changes to the athlete's blood profile suggest doping. Those with suspicious profiles can then be targeted for additional testing by the antidoping agencies.67–69 Other doping methods that have the potential to enhance oxygen delivery to the muscles are covered in ‘M1 – Manipulation of blood and blood components’ section.
Ergogenic properties
Clinical studies with trained athletes have shown rhEPO to increase haemoglobin mass from 12.7 ± 1.2 to 15.2 ± 1.5 g/kg. 70 This increases the capacity to utilise oxygen (VO2 max) by around 5–10% and reduce the time to run 3000 m by approximately 6%.70,71 Perhaps the most infamous use of rhEPO has been in the Tour de France, with several prominent cyclists later confessing to using rhEPO 72 and subsequent revelations about rhEPO use by seven times Tour de France winner Lance Armstrong are well publicised. 73 The endemic use of EPO in cycling events is supported by the experiences of elite cyclist Tyler Hamilton 74 and while some individual riders had been withdrawn or suspended from the race in previous years its systematic use by teams was revealed in 1998 tour when one team was ejected from the race for using EPO and six other teams quit the event. 75 Other sports in which rhEPO use have been implicated include endurance running and endurance events in the Winter Olympics. 23
Health issues
The use of rhEPO results in an increase in red blood cell mass that is greater than an increase in the plasma volume, hence the blood becomes more viscous, 76 and studies have demonstrated haematocrit increasing from 42.7 ± 1.6 to 50.8 ± 2.0%. 71 Notably an haematocrit > 50% has been used in some sports, such as cycling, as a threshold, above which the individual is not permitted to participate, the inference being that they may have doped. 67 From a health perspective the increased blood viscosity is believed to increase the risk of thrombosis, which may be further elevated if the person becomes dehydrated. 52 Indeed some authorities have implicated rhEPO abuse with the death of competitive cyclists and other endurance athletes, 55 although the association does not appear to have been proven unequivocally. 77 Other reported health risks include: hypertension and headaches, 22 and some authorities suggest that rhEPO use may be associated with the development of some cancers. 52
hCG and hLH in males
In males, endogenous hCG and hLH act on the Leydig cells of the testes to stimulate testosterone production. 78 Because of this action, hCG and hLH and their recombinant versions (rhCG and rhLH) have the potential to be used as doping agents by males to promote the body's own production of testosterone and epitestosterone. The use of hCG/rhCG and hLH/rhLH in this way may thereby circumvent the risks of detection associated with using exogenous testosterone since both testosterone (T) and epi-testosterone (ET) are increased. This helps to maintain the normally occurring ratio of T/ET at around 1–2 and avoids the problem of a T/ET ratio exceeding 6, which can occur when exogenous testosterone is used 79 and such test results initiate further investigations.23,80 However, while a high T/ET ratio is used as an indicator of a possible doping offence by antidoping authorities, it is acknowledged that some individuals have naturally occurring low concentrations of epi-testosterone which result in an elevated ratio. 81 Alternative tests involve assessing the T/LH ratio on the basis that the use of AAS suppresses LH production and thereby elevates the T/LH ratio.81,82 rhCG may also be taken by males to restore endogenous T production by the testes, which may be suppressed through the use of exogenous AAS. 83 In males hCG/rhCG and hLH/rhLH concentrations above certain levels suggest a possible doping violation; however, it is also known that hCG can become elevated in cases of testicular cancer.39,83 Indeed there have been occasions when a doping test has resulted in tumours being identified in athletes who were unaware of their condition (Table 4). 84
In females, endogenous hCG and hLH stimulate progesterone and estradiol production by the ovaries. Endogenous hCG increases in pregnancy and the hLH surge in the menstrual cycle triggers ovulation. Consequently, these hormones have different levels and functions for males and females. In females hCG/rhCG is not believed to substantially alter T levels. 23 Therefore, for this and the previously indicated confounding reasons, which include an intrusion of privacy, neither hCG/rhCG nor hLH/rhLH is believed to be effective as doping agents in females nor are they systematically tested for. 85
Corticotrophins
These are hormones secreted from the anterior pituitary gland that act on the adrenal cortex to influence the secretion of various hormones. The key hormone is adrenocorticotrophic hormone and its primary function is to promote the release of corticosteroids such as cortisol (see ‘S9 – Glucocorticosteroids’ section). The performance effects of corticotrophins are equivocal. 86
hGH and IGF-1
hGH is a polypeptide hormone that affects many metabolic activities within the body, notably the growth and division of cells. Endogenously it is secreted in a pulsatile pattern from the anterior pituitary while exogenous sources include synthetic recombinant growth hormone (rhGH), which is difficult to distinguish from endogenous sources. Endogenous production of hGH has been shown to increase in response to high-intensity aerobic exercise. 87 Some of the indirect effects of hGH are mediated by IGF-1, which is produced in the liver and up-regulated by hGH. Among its numerous effects, IGF-1 promotes amino acid uptake and protein synthesis in muscles, which makes it an anabolic agent increasing muscle mass and strength. 23 However in contrast to hGH, it can cause hypoglycaemia and does not appear to be lipolytic. 88 Unlike the pulsatile release of hGH concentrations, IGF-1 serum concentrations are less variable across a day. 23
Anabolic and ergogenic properties
Medically, exogenous hGH (including rhGH) promotes muscle growth in people with growth hormone deficiency. This has led to its use as an anabolic doping agent by bodybuilders, weightlifters and people involved in sports requiring high levels of strength and power. 89 It is also taken for its lipolytic effects that facilitate the loss of body fat, which also makes it attractive to body builders. However, the extent to which the increases in muscle mass translate into improved sports performance is unclear.23,88,90–92 Some authorities question whether there is strong evidence for its effectiveness if taken as a sole doping agent by those who are not GHD, although they do suggest that it could have a synergistic effect if taken in combination with AAS. 93 As with studies on AAS, clinical studies with hGH may use lower doses than those taken by sports performers and hence may not provide a true reflection of its ergogenic potential. 91 The use of rhGH to benefit aerobic/endurance exercise lies in its potential to enhance lipolysis and thereby spare muscle glycogen, which is a limiting factor in prolonged (>2 h) exercise. 94 However, despite the equivocal nature of the clinical evidence, hGH is being used by athletes across a range of sports events from the 100 m sprint to the Tour de France; and the conviction of Sylvester Stallone for possession of hGH when entering Australia would suggest that its use extends beyond the sporting arena. 95
Health issues
The use of hGH in supraphysiological doses, which in athletes may be 10 times higher than the therapeutic dose, 95 is known to cause fluid retention due to its effects on increased sodium retention by the kidneys, with peripheral oedema resulting in swollen hands and feet as well as headaches and hypertension. It may also cause carpal tunnel syndrome and long-term use can produce aspects of acromegaly 54 (the abnormal growth of the bones) which occurs in those with inherently elevated concentrations of hGH. Additionally, since acromegaly is associated with muscle weakness it has been argued that it could theoretically have an adverse effect on performance, 52 although its widespread use by power athletes and bodybuilders would suggest otherwise. 23
hGH abuse has also been reported to increase the risk of cardiomyopathy, possible arrhythmias, insulin resistance that can lead to diabetes mellitus, bone abnormalities, adverse lipid profiles, acute renal failure and osteoarthritis.23,52,55,96 As a doping agent it can be obtained as synthetically produced rhGH, but has also been available from cadaveric sources, which incur the risk of contracting Creutzfeldt–Jakob disease.93,95
Some studies report the adverse effects of IGF-1 to be hypoglycaemia, myalgia and fluid retention, 97 while others indicate that the long-term effects of its abuse are largely unknown. 98 hGH and IGF-1 abuse have also been associated with colon, breast and prostate cancers.52,77
S3 – Beta 2 agonists
Adrenaline and noradrenaline are catecholamine hormones that are released from the adrenal medulla and also function as neurotransmitters. Their secretion increases at times of stress and facilitates a physiological response to a situation. In a sporting context this relates to increases in cardiac output, vasodilation, ventilation and circulating glucose, with the response being proportional to the intensity of the exercise. These catecholamines bring about their effects through binding to ß-adrenoceptors (ß-AR), both ß1-AR and ß2-AR. 99 These ergogenic properties have been exploited by the use of doping agents in the classes of ‘beta 2 agonists’ and ‘stimulants’ (see ‘S6 – Stimulants’ section).
Beta 2 agonist drugs that have the potential to be doping agents in sport focus on the ß2-AR in the brain and peripheral tissues. Stimulation of these receptors results in diverse effects such as bronchodilation, anabolic actions and the enhancement of anti-inflammatory corticosteroids. 99 Beta 2 agonist drugs may be inhaled or taken orally and are commonly used as medications to treat and prevent asthma. WADA prohibits the use of beta 2 agonists, including bronchodilators unless the participant has a ‘therapeutic exemption’, which must be applied for. 100 This exception covers a limited list of drugs such as formoterol, salbutamol, salmeterol and terbutaline when taken via inhalation. Studies suggest that these drugs do not appear to have an ergogenic benefit when inhaled, but salbutamol may improve strength and endurance if taken orally. 101 One beta 2 agonist that has been used as a doping agent in sport is clenbuterol. Clenbuterol is a non-steroidal anabolic agent that increases muscle mass, which would explain its use by weightlifters and other strength athletes. It is also used in the livestock industry and some recent reports suggest that eating the meat of animals given clenbuterol could result in a positive test. 102
Ergogenic effects
In terms of performance benefit for the elite non-asthmatic athlete, ß2-agonists do not improve aerobic capacity (VO2 max), performance in endurance events, or peak cycling power. 103 Similar results were found by Elers and colleagues who also found no effect on oxygen kinetics. 104 However, Pluim et al.'s analyses of studies that had used systemic ß2-agonists produced equivocal results, with some studies indicating that they could benefit endurance performance and cycling sprint power, and others concluding that oral ß2-agonists, combined with resistance training could improve strength.103,105 Hence the therapeutic inhaled doses of ß2-agonists do not appear to be ergogenic, but systemic and supraphysiological doses may enhance the effects of strength training and benefit endurance performance.
Health risks
Clenbuterol and salbutamol are the most commonly reported doping agents in this class, with clenbuterol in particular being taken for its anabolic properties. Since beta 2-AR agonist drugs bind to the ß2-AR in the heart they thereby elicit health risks such as cardiac arrhythmias, palpitations and myocardial ischemia. 106 They are also reported to cause muscle tremor and may increase circulating glucose concentrations due to their action on the liver. Additionally, clenbuterol has also been associated with reducing bone mineral content. 91
S4 – Hormone and metabolic modulators
The prohibited list divides this category into five groups
2
:
Aromatase inhibitors; Selective oestrogen receptor modulators (SERMs); Other antiestrogenic substances; Agents modifying myostatin function(s); Metabolic modulators.
Aromatase inhibitors, SERMs and other antiestrogenic substances
These drugs are used clinically in the treatment of breast cancer or other tumours that are hormone dependent. They are also used in the treatment of osteoporosis. In males oestradiol is produced by the aromatisation of testosterone and this oestradiol plays a key role in the negative feedback regulation of testosterone production via the HPT axis. Oestrogen blocker drugs include antiestrogen drugs that block oestrogen receptor action and aromatase inhibitors that block the synthesis of oestradiol. Hence when males take these drugs the negative feedback process is interfered with, resulting in increased secretion of gonadotrophins from the pituitary and a subsequent increase in circulating testosterone. 40 They may therefore convey an ergogenic benefit to males from the elevated concentrations of testosterone. Additionally, they may be taken by males trying to prevent the development of gynaecomastia, which occurs with AAS abuse that results in elevated oestrogens. 23 Due to the physiological and endocrinological differences between male and female, oestrogen blocker drugs are unlikely to increase testosterone concentrations in females to concentrations that would measurably increase muscle mass or strength. When used inappropriately the health risks include cardiac arrhythmias, dizziness, osteoporosis and joint pain. Some can also result in breathlessness.
Agents modifying myostatin function(s)
Myostatin (growth differentiation factor 8) is a naturally occurring hormone that regulates muscle growth. Its function is to limit growth and hence muscle mass. Naturally occurring genetic mutations occur in which the myostatin is non-functional and this results in an abnormally large muscle mass, with homozygous conditions being more extreme than the heterozygous condition. This is exploited in the livestock industry with the Belgian Blue and Piedmontese cattle breeds in which abnormalities in the myostatin genes result in cattle with greater muscle mass and hence increased meat production. Further examples occur in greyhounds and there are a few recorded examples in humans. Clinically, myostatin inhibitors endeavour to inhibit the normal action of myostatin and thereby have the potential to treat muscle wasting conditions such as sarcopaenia, muscular dystrophy and cancer cachexias. 23 As doping agents this inhibitory effect may enable muscle hypertrophy to exceed that attainable under non-doping conditions.
Metabolic modulators
Metabolic modulators include insulins and peroxisome proliferator activated receptor δ (PPARδ) agonists. Insulin is a key regulator of glucose concentrations within the blood and is secreted by the β cells of the pancreas primarily in response to high blood glucose concentrations. Clinically, it is used by insulin-dependent diabetics whose endogenous production of insulin is insufficient or non-existent. The use of exogenous insulin by non-diabetics can lower blood glucose to hypoglycaemic concentrations, resulting in the risk of dizziness and coma in more extreme cases. As a doping agent, insulin may increase the rate of glucose uptake into the muscles and thereby aid recovery by facilitating muscle glycogen replenishment. In addition to their hypoglycaemic properties, insulins have an anabolic action, which makes them potential doping agents for increasing muscle mass.23,107 However, while there are some reports of insulin abuse it does not appear to be as widespread as other anabolic agents.
PPARδ agonists specifically mentioned in the WADA prohibited list are 5-aminoimidazole-4-carboxamide-1-β-D-ribofuranoside (AICAR; PPAR-δ-AMPK (AMP-activated protein kinase) agonist) and GW1516 (PPARδ-agonist). 2 Their inclusion on the prohibited list relates to their effect in augmenting the adaptations to endurance training, such as the enhancement of mitochondrial biogenesis, angiogenesis and insulin sensitivity, 108 with the overall outcome being muscle fibres with a greater aerobic capacity and greater fatigue resistance. Mechanistically PPARδ are believed to be involved with AMPK and Peroxisome proliferator-activated receptor-γ coactivator (PGC)-1α responses, which have well-established roles in the promotion of biogenesis postexercise.
Health risks
As mentioned previously, one of the consequences of AAS abuse is their conversion to oestrogens, with a resultant risk of gynaecomastia. To combat this, oestrogen antagonists such as SERMS may be used, as are aromatase inhibitors that inhibit the synthesis of oestrogen. The health risks associated with the specific use of these drugs as doping agents by ‘healthy’ individuals are currently unclear, since they are taken in combination with other doping agents. However, it is suggested that oestrogen blocking agents and aromatase inhibitors do not have direct androgenic effects, and therefore do not convey the health risks associated with the use of androgens such as AAS. 40 The health risks associated with the use of myostatin inhibitors are likewise unclear at this stage, but their potential for development as therapeutic agents means that their use may become more widespread in the future.
S5 – Masking agents
Masking agents are not considered performance enhancing, but they are taken to conceal the use of other doping agents and abuses. They include diuretics, epi-testosterone, probenecid, 5α-reductase inhibitors and plasma expanders. The mechanism of action varies, with the intention being to reduce the concentration of the doping agent or its metabolites in the sample through increasing the volume of urine or reducing the rate of excretion of the doping agent/metabolites into the urine; or alternatively by interfering with the parameters used by antidoping labs to identify doping offences. 109
Diuretics
Therapeutically, diuretics are used to increase urine production and sodium excretion. They are prescribed for a variety of conditions, such as hypertension, heart failure, liver, kidney and lung diseases. 110 Diuretics promote urine production. As doping agents they are used in a number of sporting contexts for a variety of reasons, with the 2008 WADA laboratory statistics indicating that nearly 8% of positive samples involved diuretics. 111 The diuretic-induced increase in urine production has two effects that may be exploited by the doping athlete. First, it can produce a rapid and temporary weight reduction when endeavouring to make a weight category in sports such as boxing. It may also be used to counteract fluid retention, which can occur when using other drugs, notably in body building where the fluid excess would conceal the definition of the musculature. Second, the increased urine volume will lower the concentration of doping agents and/or their metabolites in a urine sample, with the intent of reducing the concentration to below detectable concentrations. Third, some diuretics can alter urinary pH and inhibit the excretion of some drugs into the urine, thereby lowering their concentration in urine samples. 110
Health risks
The use of diuretics either to reduce weight or mask the use of other doping agents through the production of copious amounts of dilute urine entails the risk of dehydration and excessive loss of minerals such as potassium and calcium.
Probenecid
Therapeutically, probenecid is used to treat chronic gout and may also be prescribed alongside antibiotics for the treatment of some bacterial infections. Probenecid acts on the renal tubules of the kidneys to increase the excretion of uric acid and reduce the excretion of some acidic compounds. In a doping context, this would include a reduced excretion of testosterone, epi-testosterone and AAS, which are excreted mainly as their glucuronic acid compounds. In such contexts, the purpose of using probenecid is to lower the concentrations of exogenous doping agents and their metabolites to below the detectable concentrations. 109 It may also interfere with the concentrations of endogenous T and E in urine samples.
Plasma expanders
Clinically, plasma expanders, in the form of colloid solutions containing dextrans, are used in situations of blood or fluid loss. As doping agents they may be used to mask the use of EPO and blood infusions. The rationale for their use is that EPO and blood infusions will increase the haematocrit and Hb concentrations, which are advantageous in endurance sports. Sports authorities set thresholds for haematocrit and the concentration of haemoglobin, above which a possible EPO and/or blood transfusion doping offence is indicated. Plasma expanders will temporarily dilute the blood, lowering the haematocrit and Hb concentration, thereby bringing them below the concentrations that are used as indicators of doping.
M1 – Manipulation of blood and blood components
Autologous and allogenic blood doping
As previously stated, increasing RBC elevates the capacity of the body to deliver oxygen to the exercising muscles and increases aerobic performance.112,113 Key to this improvement is the increase in the total Hb mass rather than [Hb] or Hct, although these tend to increase alongside the increase in Hb mass.114,115 Consequently, drugs such as rhEPO are banned (see ‘S2 – Peptide hormones, growth factors and related substances’ section). Prior to the availability of rhEPO in the 1980s, endurance athletes and cyclists are known to have achieved an increase in RBC via the transfusion of matched blood from another person (homologous or allogenic blood doping) or through the reinfusion of their own blood, which had been removed around four weeks previously and then reinfused 1–7 days before the event (autologous blood doping). Since the development of tests to detect rhEPO and allogenic blood doping in the early 2000s, 113 autologous blood transfusion has made a resurgence among those wishing to avoid detection. 116 Tests to detect autologous doping assess inconsistencies in the blood profile of athletes in accordance with the Athlete's Biological Passport, in which a record of their blood profile from previous tests has been recorded. Longitudinal comparisons of the athlete's blood involve assessing a combination of hematologic markers. 117 These tests work on the basis of detecting altered erythropoiesis and include measures of total mass of haemoglobin and the ratio between the amount of Hb in the mature erythrocyte population and the reticulocytes (RBCHb:RetHb ratio).116,118,119 Other suggested markers relate to the body's response to the withdrawal of blood (anaemic phase) in which [Hb] is reduced, while EPO, % reticulocytes and soluble transferrin receptor (sTfR) increase for a number of days until the blood loss is replenished. 120 Another approach for the detection of autologous blood doping is to test for markers that indicate that blood has been in storage. These include decreases in 2,3-bisphosphoglycerate, altered cell membrane structure, 112 changes to gene expression related to T lymphocytes that occurs due to a transfusion-induced immune response and the presence in the urine of metabolites of plasticisers such as di-ethylexylphthalate that have leaked from the bags in which the blood was stored.121,122
Ergogenic properties
A review of early studies conclude that blood doping using 1–3 units of blood increased Hct by up to 13%, improved aerobic capacity (VO2 max) by 0–10% and endurance by 3–37%. 123 These figures were supported by later studies. In the 1984 Los Angeles Olympics, some members of US cycling team utilised blood transfusions and achieved exceptional performances including nine medals; the US having not won a cycling medal in the previous 72 years of the games. 124 The more recent revelations around the Tour de France further support the efficacy of this practice in enhancing aerobic performance in cycling. 74 These doping practises extend into other sporting arenas, such as distance running and endurance skiing events. 121
Health risks
Health issues relate to the risks of infection and in cases of allogenic blood doping, the risk of transferred infection and mismatching of blood.
Artificial enhancement of oxygen uptake, transport and delivery
Other potential agents that enhance oxygen delivery to the muscles include synthetic O2 carriers such as haemoglobin-based oxygen carriers and perfluorocarbons.72,122 However, unlike endogenous Hb, which releases more of its oxygen to the tissues in hypoxic conditions, the aforementioned exogenous artificial agents do not, which may limit their effectiveness. They also have adverse side effects and may result in tissue damage, which would not make them conducive as doping agents. 72 Likewise, while endogenous 2,3-diphosphoglycerate (2,3-DPG), which promotes oxygen release to the tissues is clearly beneficial to the endurance athlete, artificial 2,3-DPG mimetics do not as yet appear to be effective in a sporting context due to easy detection and a short half-life. 72 However, others suggest that efaproxiral, which alters the haemoglobin–oxygen saturation curve, may be of benefit. 122
M2 – Chemical and physical manipulation
This refers to tampering with a sample taken as part of the antidoping testing procedures, in order to alter its integrity and validity. It also includes the adulteration of samples by the addition of proteases and other chemicals that alters parameters of the steroid profile, a characteristic that appears to be relatively consistent within individuals, but is altered by the use of doping agents. For the interested reader, aspects of this were investigated and are described in detail by Kuzhiumparambil and Fu. 125 ‘Intravenous infusions and/or injections of more than 50 mL per 6 hour period except for those legitimately received in the course of hospital admissions or clinical investigations’ are also prohibited. 2
M3 – Gene doping
The capacity to attain an elite level of performance in sport has a genetic component, and it is said that to become an elite athlete you need to choose your parents very carefully. The current human gene map for performance and health-related fitness phenotypes identifies over 200 genes that appear to be associated with athletic performance 126 : some phenotypes favouring endurance, while others favour strength, anaerobic power and sprinting.
Gene therapy is a concept that has the potential to treat genetically based diseases such as cystic fibrosis, 127 Duchenne muscular dystrophy and many others. It works primarily on the principle of adding a functional gene and/or genetic material into the cells of the recipient and thereby enabling the expression of a gene. This may increase the number of copies of the gene within these cells or provide a functioning form of the gene to cells when the recipient's own genotype includes a less effective or non-functioning mutated version of that gene. The means by which this new genetic material gets into the cells is usually via a virus (viral vector) with the virus being introduced into the body via injection or nasal spray. Once in the target cells the introduced genetic material will be activated to produce the mRNA and protein that the cell/body currently lacks. To date there are relatively few examples of effective gene therapy, but as a concept it has great potential.
In a sporting context, the principles of gene therapy have been foreseen as having the potential for abuse as a doping procedure. For example, in theory it could be abused to enhance an athlete's production of proteins such as EPO, 128 hGH and IGF-1, 129 vascular endothelial growth factor and myostatin antagonists that will promote muscle hypertrophy. 130 So, while there are no recorded cases of gene doping or even its efficacy in enhancing performance, the procedure has been added to the WADA banned list. Furthermore, the process of gene doping, which has the potential to temporarily enhance or suppress the production of key proteins could be further developed into genetic enhancement, whereby the introduced genetic material becomes fully integrated into that of the recipient and is consequently replicated with the host's own genetic material and is thereby be perpetuated with each cell division. If such procedures become a reality they may again convey great benefits in a therapeutic setting but would also be open to abuse in sport. For example, as the details of the human genome are further elucidated, the influence of specific genetic polymorphisms upon the individual's aerobic capacity and endurance or ability to produce high anaerobic power and sprint become evident, 126 manipulating the genetic makeup of the individual has the potential to augment their performance.
In the context of health risks, the science of gene therapy is in its infancy with relatively few successful clinical trials, but even these have exposed risks with the procedures, and some of these have fatal consequences, even in carefully regulated clinical trials.
S6 – Stimulants
Stimulants are a diverse group of banned drugs that are ‘banned in competition’. They have the confounding aspect of including drugs that while having possible ergogenic properties may also be found in over-the-counter medicines and/or be taken as ‘recreational drugs’. The former would include ephedrine and pseudoephedrine, while the later would include cocaine and ecstasy. Studies indicate that stimulants account for around 6–18% of the positive samples detected in the sporting context, which makes them the third most prevalent category, behind AAS and cannabinoids. 131 The stimulant caffeine, which is included in a number of sports drinks and gels and generally consumed broadly around the world, was removed from the WADA banned substance list in 2004 but is briefly considered in this review.
The potential ergogenic properties of stimulants primarily relate to their effects on the central nervous system and their capacity to: reduce the perception of fatigue; increase alertness, promote self-efficacy and confidence; and in some cases stimulate cardiac output and blood flow to the exercising muscles. Typically, they work via their pharmacological effects on increasing the release of neurotransmitters, blocking the reuptake of neurotransmitters and the activation of receptors. Some mimic the responses of the sympathetic neuroendocrine system, notably adrenaline and noradrenaline, while others affect the dopamine and serotonin systems. 132 WADA lists over 60 specific drugs within this category and includes a general statement aimed at covering similar drugs with similar properties.
Evidence for the ergogenic efficacy of many stimulants on sports performance is often equivocal and the use of such drugs can entail serious health risks including hyperthermia, stroke, respiratory and cardiac arrest. 99 A difficulty with clinical research on the ergogenicity of stimulants is that the laboratory/experimental setting can rarely, if ever, fully mimic the competition environment. As a consequence an enhanced performance in experimental trials, when arousal may not be maximal, may not translate into the competition environment when the athlete's arousal is likely to be higher. Within this review, a few examples will be mentioned briefly to illustrate the characteristics of different stimulants. For a more extensive coverage of the pharmacological aspects, see the review by Docherty. 132
Amphetamines
Amphetamines may be used in sport to reduce the perception of fatigue and promote concentration, alertness and self-confidence. They enhance the brain activity of noradrenaline and dopamine. 133 They also increase blood pressure and peripheral vasoconstriction.
Health risks
Their use has been associated with ventricular dysrhythmias, increased blood pressure and peripheral vasoconstriction. 76 As a consequence they increase the risk of tachycardia and cardiovascular failure, as well as reducing the body's capacity to lose the heat generated during strenuous exercise, which may result in hyperthermia. 133 Some fatalities in endurance cycling events have been attributed to this, including the televised death of Tommy Simpson in the 1967 Tour de France. Other health risks include anxiety, hallucinations and insomnia.32,133 Their regular use can result in tolerance and dependence that may cause depression following withdrawal. 133
Sympathomimetics (ephedra alkaloids including ephedrine and pseudoephedrine)
This group includes the drugs ephedrine and pseudoephedrine, which are agonists at both α- and β-adrenergic receptors, increasing heart rate and blood pressure.134,135 Ephedrine and pseudoephedrine are sympathomimetics commonly included in decongestant drugs. WADA monitors these substances on the basis of a urine concentration threshold due to their presence in many over-the-counter medicines, including those for nasal congestion. 2 The concentration for ephedrine is set at >10 mg/L and pseudoephedrine is set at >150 mg/L. Ephedrine acts on the CNS promoting the release of noradrenaline, 133 with resultant increases in heart rate and blood pressure. Other ephedra alkaloids have similar properties and may be found in traditional Chinese medicines, examples being the herb ma huang or guarana. 136 They may be abused by athletes because of a perceived benefit to strength, aerobic performance and even fat loss; however, studies on performance are equivocal, although there is some evidence that they may convey performance benefits if taken with caffeine. 135
Health issues
Reviews of sympathomimetic drugs indicate that their use has been linked to a number of adverse cardiovascular events and fatalities, including stroke, arrhythmias and myocardial infarction, as well as hypertension.133,134
Cocaine
Cocaine is reported to reduce the perception of fatigue and promote confidence and euphoria, which may aid performance. It exerts its effects via the CNS, increasing the release of catecholamines, dopamine and inhibiting the reuptake of noradrenaline.
Health risks
The health risks of cocaine are reported in the wider context of its use as a recreational drug and include: elevated heart rate and blood pressure, myocardial ischemia, myocardial infarction, arrhythmias and cardiac arrest even in the absence of atherosclerosis.133,134 It is considered highly cardiotoxic when taken with alcohol. 133 It can also adversely affect the vascular, pulmonary, gastrointestinal, musculoskeletal and genitourinary systems, as well as causing cerebrovascular events.133,137 Additionally, its vasoconstrictive action may adversely affect thermoregulation. 76
Caffeine
Caffeine is a stimulant that is not currently banned by WADA, despite its proven ergogenicity. In the past it was included on the banned list at urine concentrations above (12 μg/mL), on the basis that concentrations below this level may be attained from the consumption of coffee, coca cola and similar sources, whereas above this concentration indicated a deliberate consumption, probably via tablets, with the intent of performance enhancement. It was removed from the ‘banned list’ in 2004 but is still subject to monitoring, although it should be noted that the ergogenic benefits for a range of sports appear to be attained at modest doses (3 mg/kg): which are easily achieved via intake of everyday dietary sources such as coffee, cola drinks and energy drinks. The performance benefits include reductions in the perception of fatigue and direct effects on muscle contractility, although previously claimed mechanisms such as the promotion of fat as a fuel sources during endurance events are no longer considered important. 138
S7 – Narcotics
The category of narcotics includes substances such as morphine and related compounds. Morphine is known for its analgesic effects in increasing tolerance to pain, which may thereby improve performance. Another notable drug in this category is heroin, the health risks of which are reviewed elsewhere in the context of its wider use in society.
S8 – Cannabinoids
Natural and synthetic cannabinoids are banned ‘in competition’ and there have been a number of high-profile cases in which athletes have produced positive samples following competition and been disqualified as a consequence. Due to their ‘relaxing’ properties, such drugs are likely to impair performance (ergolytic) rather than being ergogenic 139 but a substance does not have to have proven ergogenic properties to be included on the WADA banned list, and the cannabinoids would tend to fall into this realm. Indeed, the reported reasons for taking them include relaxation and the promotion of sleep prior to competition. However, due to their effects on alertness, concentration and reaction time, they may present a safety problem for others as well as the user in some sporting contexts, 140 which is why they are banned. For the wider context, readers are directed to other reviews on the mental health consequences of taking cannabinoids.141,142
S9 – Glucocorticosteroids
Physiological glucocorticosteroids include cortisol and cortisone, which have an anti-inflammatory role. They are used to treat musculoskeletal and tendon injuries: a common example being hydrocortisone. In sport they are ‘banned in competition’ 2 due to their effects on pain relief and perhaps fatigue, which may aid performance. They but may also exacerbate injury to the damaged tissues as the person is able to continuing loading the tissue in the absence of pain that would normally cause cessation of the activity. 143 In the past they may also have been taken under the belief that their effects on increasing gluconeogenesis and the mobilisation of amino acids and fatty acids would aid performance, although the evidence for this is equivocal. 144
Health issues
Glucocorticosteroid injections are sometimes used within the treatment programme for Achilles, quadriceps and hamstring tendons. However, while their use may accelerate the athlete's return to training and competition, there is some debate as to whether their use is also associated with an increased risk of subsequent rupture of the tendon due to degenerative processes and incomplete repair in the tendon.96,143,145 This has raised concerns about the chronic use of non-steroidal anti-inflammatory drugs, which while producing short-term relief may retard complete healing and recovery of the tissue. In addition, the chronic use of glucocorticosteroids may increase the risk of diabetes mellitus, osteoporosis, necrosis of the femoral head and growth retardation in children.76,96,146
P1 – Alcohol
Within the WADA prohibited substances list alcohol (ethanol) is prohibited in competition in specific sports above a blood concentration of 0.10 g/L (i.e. 0.01%). 2 It is banned for reasons of safety to the participants and others, in sports including: aeronautics, archery, motorsport, karate and power-boating. The acute effects of alcohol consumption are generally ergolytic but may be used by the participants in sports requiring ‘boldness’, such as downhill skiing and mountain biking to overcome inhibitions and thereby improve performance or perception of performance. 147 Its health issues will not be discussed here as they are extensively debated elsewhere and in the wider context of society.
P2 – Beta-blockers
Beta-blockers also come under a category of being prohibited in specific sports during competition. Since their effects are antagonistic at the β-adrenergic receptors they have the effect of slowing the heart rate and reducing blood flow to the muscles, which would be ergolytic rather than ergogenic. 99 However, their performance benefits relate to a calming effect in slowing the heart rate and reducing tremor, which has been demonstrated to improve pistol shooting and may benefit similar target sports. 148 Hence they are not permitted in archery, motorsport, billiards, darts, golf, shooting and skiing/snowboarding. The health risks of their abuse include bradycardia, orthostatic hypotension and arrhythmias, as well as reducing the capacity to thermoregulate. 55
Concluding remarks
In summary, this review has provided an overview of the WADA doping categories, why substances or methods within these categories are used, the performance benefits, health risks and implications for clinical samples. While laboratories accredited by WADA carry out testing for these doping agents, in reality novel mechanisms of doping are being utilised by sports people at all levels to achieve that unfair advantage.
In the context of health risks, the use of various doping agents, including the most prevalent, such as AAS, stimulants and EPO, increases the risk of cardiovascular disease, thrombosis, stroke and cancers in males and females. Additionally, the use of AAS adversely affects the hormonal axes resulting in the suppression of endogenous hormone production in males, while exerting a virilising affect in females. Furthermore, the regular use of some anabolic agents and stimulants can have serious mental health/behavioural consequences. Hence the physical and mental health risks associated with the use of such agents are likely to exceed the health benefits associated with participation in physical activity. The prevalence of doping agents extends beyond the realms of elite sport, into lower levels of competition and into non-competitive exercise training for the development of an enhanced physique. So while the reliability of prevalence data and health impacts have limitations, the indications are that doping and related drug abuse represent a significant health issue, and those involved in the clinical testing of samples should be aware of the potential for some patients sample results to be affected by doping practises.
Footnotes
Acknowledgements
This article was prepared at the invitation of the Clinical Sciences Reviews Committee of the Association for Clinical Biochemistry and Laboratory Medicine.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
Not required.
Guarantor
SRB.
Contributorship
All authors listed contributed to this work. SRB researched the sporting literature and was the primary author, RFG provided the expertise in the clinical biochemistry aspects, CB contributed to the clinical aspects and current drug testing issues, while LMB provided the expertise in the sports antidoping aspects.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.