
Abstract
Background
Deriving and validating local adjusted calcium equations is important for ensuring appropriate calcium status classification. We investigated the impact on our local adjusted calcium equation of a change in calcium method by the manufacturer from cresolphthalein complexone to NM-BAPTA.
Methods
Calcium and albumin results from general practice requests were extracted from the Laboratory Information Management system for a three-month period. Results for which there was evidence of disturbance in calcium homeostasis were excluded leaving 13,482 sets of results for analysis. The adjusted calcium equation was derived following least squares regression analysis of total calcium on albumin and normalized to the mean calcium concentration of the data-set. The revised equation (NM-BAPTA calcium method) was compared with the previous equation (cresolphthalein complexone calcium method).
Results
The switch in calcium assay resulted in a small change in the adjusted calcium equation but was not considered to be clinically significant. The calcium reference interval differed from that proposed by Pathology Harmony in the UK.
Conclusions
Local adjusted calcium equations should be re-assessed following changes in the calcium method. A locally derived reference interval may differ from the consensus harmonized reference interval.
Introduction
Serum calcium concentration is commonly adjusted for albumin (Alb) to assess more accurately the calcium status. Locally derived adjusted calcium (ACa) equations normalized to a mean calcium of 2.40 mmol/L are advocated in the UK by Pathology Harmony for harmonized ACa reference intervals of 2.20–2.60 mmol/L. 1 Important differences in calcium status classification between locally derived and generic ACa equations have been observed in previous studies. 2 In addition, changes in analytical methodology have previously been noted to change regression coefficients in the ACa equation. 3 A review of our locally derived ACa equation was prompted by a change in the local calcium assay; Roche cresolphthalein complexone (Roche Diagnostics UK Ltd, West Sussex, UK) to NM-BAPTA (Roche Diagnostics UK Ltd). The albumin method remained unchanged (bromcresol green; Roche Diagnostics UK Ltd).
Methods
Data were collected from the Laboratory Information Management system (Telepath, iSoft Ltd [CSC], UK) and separated by requesting location. To minimize the inclusion of patients with disturbances in calcium homeostasis, data were included only on requests from general practice patients between May and July 2013. Replicate results on the same patient were removed with only the initial result being included in the dataset. Results were excluded if urea, creatinine or alkaline phosphatase were above the upper limit of normal, total calcium > 3.00 mmol/L and albumin < 20 g/L or > 50 g/L, leaving 13,482 sets of results. Least squares regression analysis (Microsoft Excel 2003; Microsoft Limited, Reading, UK) of total calcium on albumin was used to generate the ACa equation according to procedures described previously.4,5 The revised ACa equation was compared with the current ACa equation, ACacurrent = Total Ca + 0.0133 (44.1 − [Alb]), to assess the impact of the calcium method change. The current equation was derived using the same procedure described herein.
Results
Total calcium and albumin results were normally distributed with means (95% CI of mean) of 2.32 (2.322–2.325) mmol/L and 43.2 (43.2–43.3) g/L, respectively. Linear regression of total calcium and albumin is shown in Figure 1 (y = 0.0152x + 1.67; R2 = 0.22). The adjustment equation was normalized to the local mean calcium concentration of 2.32 mmol/L and generated a revised ACa equation, ACarevised = Total Ca + 0.0152 (43.2 − [Alb]). Mean absolute and percentage differences in ACa between the current and revised adjustment equations were − 0.002 mmol/L and − 0.7%, respectively. This was not deemed clinically significant, which we defined as an absolute difference in ACa < 0.1 mmol/L or a percentage difference < 5% as proposed previously.
5
The 95% population reference intervals for ACa were 2.15–2.49 mmol/L (revised equation) and 2.16–2.51 mmol/L (current equation). The regression equation between the ACa results generated by the current and revised equations was y = 0.996 x−0.002; R2 = 0.995. Both the current and revised 95% population reference intervals are lower than the Pathology Harmony reference interval. Other studies have previously reported differences in locally derived regression equations and reference intervals between laboratories.
4
If local ACa reference intervals were applied rather than Pathology Harmony reference intervals, calcium status classification would have changed from low to normal in 433 cases (3.2% of total cases) and normal to high in 294 cases (2.2% of total cases). If all patients with disturbances in calcium status were further investigated, 139 fewer investigations would have been performed over the three-month study period if local rather than Pathology Harmony reference intervals were used. The clinical appropriateness of further investigations in cases of discrepant results was not investigated.
Linear regression relationship of total calcium on albumin derived from a cohort of primary care patients (n = 13,482) with simultaneous calcium and albumin measurements between May and July 2013.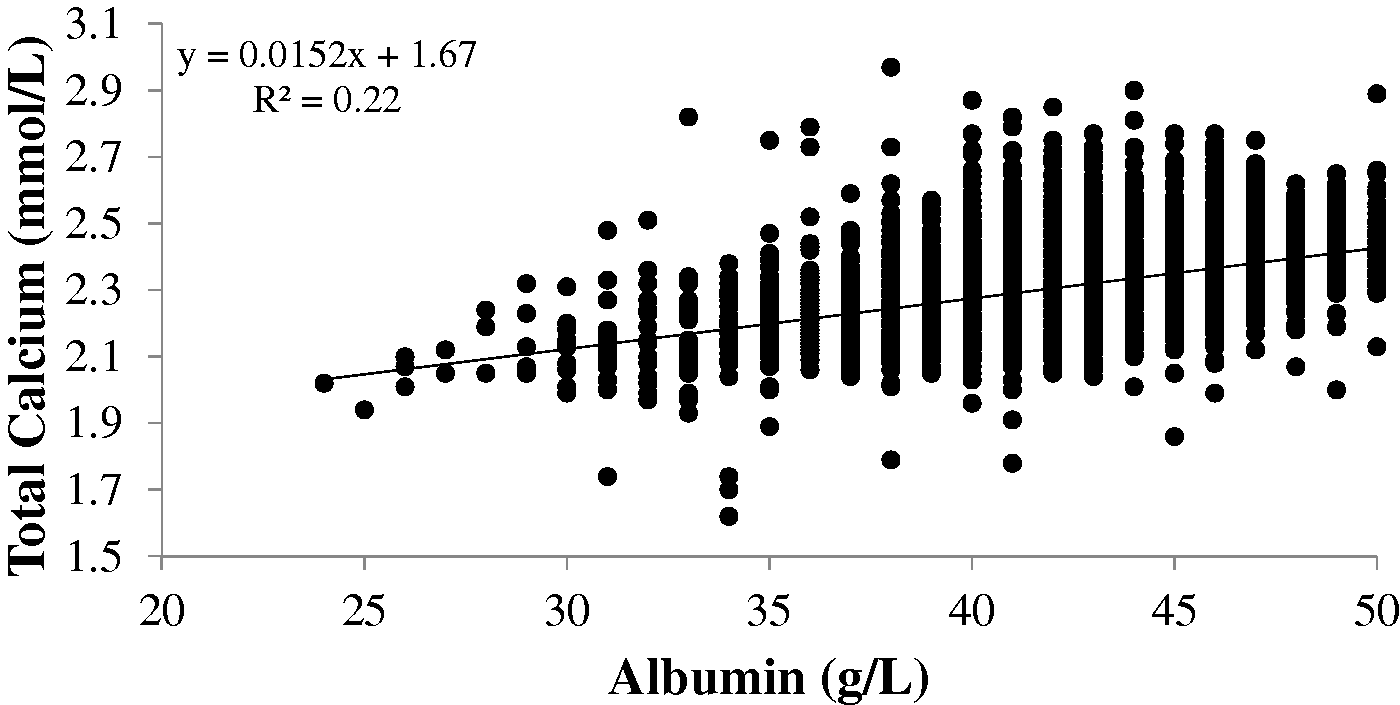
Conclusions
A change in the calcium assay (cresolphthalein complexone to NM-BAPTA) had a minimal effect on the local ACa equation. However, regular review and internal validation of the locally derived equation remain important, particularly following a change in analytical method. Normalizing adjustment equations to a mean ACa of 2.40 mmol/L (the mid-point of the Pathology Harmony reference interval) should allow for use of the harmonized reference interval for ACa advocated in the UK by Pathology Harmony (2.20–2.60 mmol/L). 1 However, the total calcium reference interval proposed by Pathology Harmony was based on consensus rather than a robust derivation from a reference population. We opted to normalize the adjustment equation to the mean total calcium of our dataset as has been proposed by others.4,5 The dataset reference interval for ACa so produced differed from that proposed by Pathology Harmony. This may reflect the case-mix of our dataset, the consensus derivation of the Pathology Harmony reference interval or the lack of ‘gold standard’ methods for calcium and albumin. If the dataset had been normalized to a Pathology Harmony mean of 2.40 mmol/L, the ACa equation generated would have been ACarevised = Total Ca + 0.0152 (48.2 − [Alb]) and would have given a 95% population reference interval of 2.23–2.57 mmol/L. The application of different reference intervals will inevitably result in different classifications for some patients with respect to their calcium status. The clinical significance of this was not addressed in the present study.
In summary, this report highlights the fact that a change in the calcium assay will affect the ACa equation, although this may not necessarily be of clinical significance. The ACa equation should, however, be re-assessed in the event of any change in the calcium assay. It also demonstrates that a consensus, harmonized reference interval may differ from a locally derived one.
Footnotes
Declaration of conflicting interests
None declared.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Ethical approval
Not applicable.
Guarantor
SD.
Contributorship
AM and AD conceived the study. SD, CH, AD and AM performed data capture and analysis. SD wrote the first draft of the manuscript. All authors reviewed and edited the manuscript and approved the final version of the manuscript.