
Abstract
Background
The aim of this study was to evaluate the use of procalcitonin in the assessment of bacteraemia in patients in the emergency department, both alone and in conjunction with existing inflammatory markers of bacterial infection.
Methods
We enrolled 3305 cases (range 20–90 years) for which we retrospectively compared procalcitonin concentration, blood culture results, body temperature, absolute neutrophil count, and C-reactive protein concentration. The positive predictive value and the negative predictive value of procalcitonin were established at different cut-off concentrations. Receiver operating characteristic curves were plotted, and the areas under the ROC curves calculated, to allow assessment of the diagnostic accuracy of (a) a combination of three existing inflammatory markers of bacterial infection (body temperature, C-reactive protein, absolute neutrophil count), and (b) this combination with procalcitonin.
Results
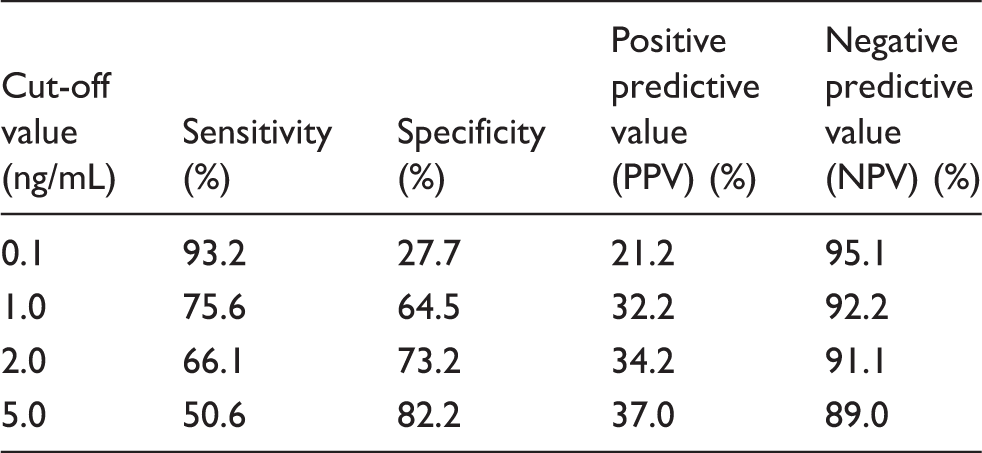
Positive predictive values of procalcitonin using 0.1, 1, 2, and 5 ng/mL as the cut-off values were 21.2, 32.2, 34.2, and 37.0%, respectively. Negative predictive values of procalcitonin using 0.1, 1, 2, and 5 ng/mL as the cut-off values were 95.1, 92.2, 91.1, and 89.0%, respectively. Areas under the curve of three inflammatory markers (absolute neutrophil count, C-reactive protein, and body temperature) combined was 0.879; areas under the curve of these markers combined with procalcitonin was 0.932 (p = 0.018).
Conclusions
When procalcitonin is used as a serum marker for ruling out bacteraemia, a cut-off of 0.1 ng/mL may be used. Procalcitonin improves the diagnostic accuracy of existing markers of bacteraemia.
Introduction
Bacteraemia is defined as the presence of bacteria in the blood. The mortality rate associated with bacteraemia is high in patients with systemic clinical symptoms, such as fever, chills, and tremors, even when these patients are actively treated. 1 Thus, it is very important to treat these cases immediately. The diagnosis of bacteraemia should therefore be made promptly and correctly in the emergency department. A blood culture is the gold standard for diagnosing bacteraemia, but the relatively long time required to obtain the results of this test means that diagnosis and treatment are delayed.2–4 Therefore, in emergency situations, a presumed diagnosis of bacteraemia may be made by taking a blood specimen and determining the white blood cell count (WBC, including the absolute neutrophil count (ANC) and the fraction of immature WBCs) and the concentrations of C-reactive protein (CRP) and procalcitonin (PCT).5–7
PCT has only recently been identified as a potential diagnostic marker of bacteraemia. Several studies have analysed its performance in the emergency department, and a meta-analysis in 2007 reported that it is moderately useful in this setting. 8 Other studies have also reported that PCT is a useful marker for ruling out bacteraemia.9–11 The 2007 meta-analysis 8 included 2008 cases of suspected bacteraemia. In order to confirm if PCT is a useful marker evaluating this condition, a larger sample size was used in the present study. In addition, we sought to determine if the addition of PCT could improve the diagnostic assessment of bacteraemia if used in combination with other markers of inflammation.
Materials and methods
Materials
The present study analysed 3305 blood samples from patients with suspected bacteraemia (1855 samples from male and 1450 samples from female) who presented at the emergency department in Seoul Asan Hospital from 1 January 2008 through 31 December 2010. ANC, CRP and PCT concentrations and blood culture positivity of each blood sample, and the body temperature of each patient at presentation, were determined by reviewing the medical records. The patients were between 20 and 90 years of age. Data from separate visits were included if the interval between visits was ≥1 month.
Methods
Blood culture tests were performed within 12 h of presentation at the hospital. Blood cultures that were determined to have been contaminated were excluded from the positive results. A blood culture was considered contaminated if bacterial growth was only detected in one set of several blood cultures or if skin-residing or contaminating bacteria (Bacillus spp., Coagulase negative Staphylococcus, Corynebacterium spp., Propionibacterium spp., Saccharomyces cerevisiae) grew in the cultures. When bacteria grew in the blood culture and contamination could be excluded, the patient was determined to have bacteraemia. The body temperature was taken upon presentation at the hospital for each case. The PCT and CRP concentrations, and the ANC, were measured immediately or within 12 h of presentation.
Body temperature
Body temperature was assessed orally as the patient arrived at the emergency department. Temperature was used to categorize patients as febrile (≥38℃) or not (<38℃).
PCT
PCT concentrations were measured using the VIDAS B.R.A.H.M.S PCT assay (bioMérieux, Marcy L’Etoile, France). The detection limit for PCT was 0.05 ng/mL. Based on previously published studies,2,11–14 four PCT cut-off concentrations were used: 0.1, 1, 2, and 5 ng/mL.
CRP
CRP concentrations were measured using a Roche reagent (Roche Diagnostics, Basel, Switzerland) and the Toshiba-200FR biochemical automated analyser (Toshiba Medical Systems Co., Tokyo, Japan). When there is a concomitant bacterial infection, a CRP concentration of ≥100 mg/L is considered diagnostically meaningful.12,14 Therefore, this was used as the cut-off value.
ANC
The ANC was measured using the Sysmex XE2100 Cell Counter (Sysmex, Kobe, Japan). Blood samples were classified into two groups based on an ANC cut-off value of 7500 cells/mm3, which is considered to be a marker of neutrophilia and is often caused by bacterial infection. 15
Blood culture tests
Blood culture tests were performed using BACTEC PLUS Aerobic/F and BACTEC LYTIC Anaerobic/F Bactec Plus (BD Microbiology, Cockeysville, MD). The presence of bacteria in the cultured blood was determined using the BACTEC 9240 System (BD Microbiology, Cockeysville, MD). After four days in culture, inoculum smearing and Gram staining were performed to look for signs of microorganism growth were detected. Culture-positive bottles were immediately analysed by Gram staining and subcultured using sterile syringes. Five millilitres of Gram-positive isolates were centrifuged into bacterial pellets and bacterial identification was performed using MicroScan Walk-away (Dade Behring, Inc., West Sacramento, CA) via direct inoculation. When micro-organism growth was not detected, sets were checked with acridine orange staining.
Statistical analysis
The sensitivity, specificity, positive predictive value (PPV), and negative predictive value (NPV) of PCT in relation to the blood culture data were analysed using SPSS (version 17.0) (SPSS Inc., Chicago, IL, USA). Body temperature ≥38℃, CRP ≥100 mg/L, ANC ≥7500 cells/mm3 can be considered indications of inflammation that could be due to a bacterial infection11,12,14; therefore, analyses of the sensitivity, specificity, PPV, and NPV were performed relative to these cut-offs. Receiver operating characteristic (ROC) curves were plotted for a combination of these three inflammatory markers, and for this combination with PCT, and diagnostic accuracy was assessed by calculating the respective areas under the ROC curves (AUCs).
Results
Sensitivity, specificity, positive predictive value, and negative predictive value of procalcitonin for predicting bacteraemia using different cut-off values.
Sensitivity, specificity, and positive and negative predictive values using different procalcitonin cut-off values for predicting bacteraemia relative to the presence of other markers of inflammation.
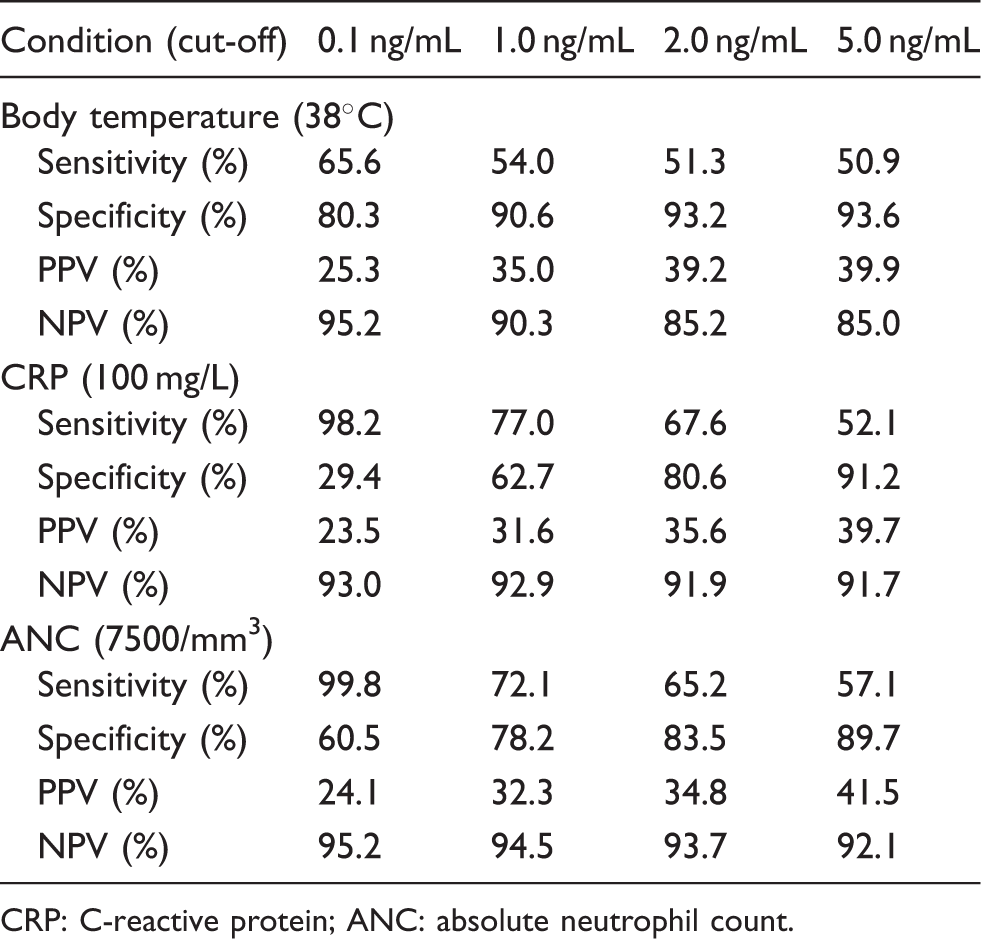
CRP: C-reactive protein; ANC: absolute neutrophil count.
Positive and negative predictive values of different procalcitonin cut-off values for predicting bacteraemia.
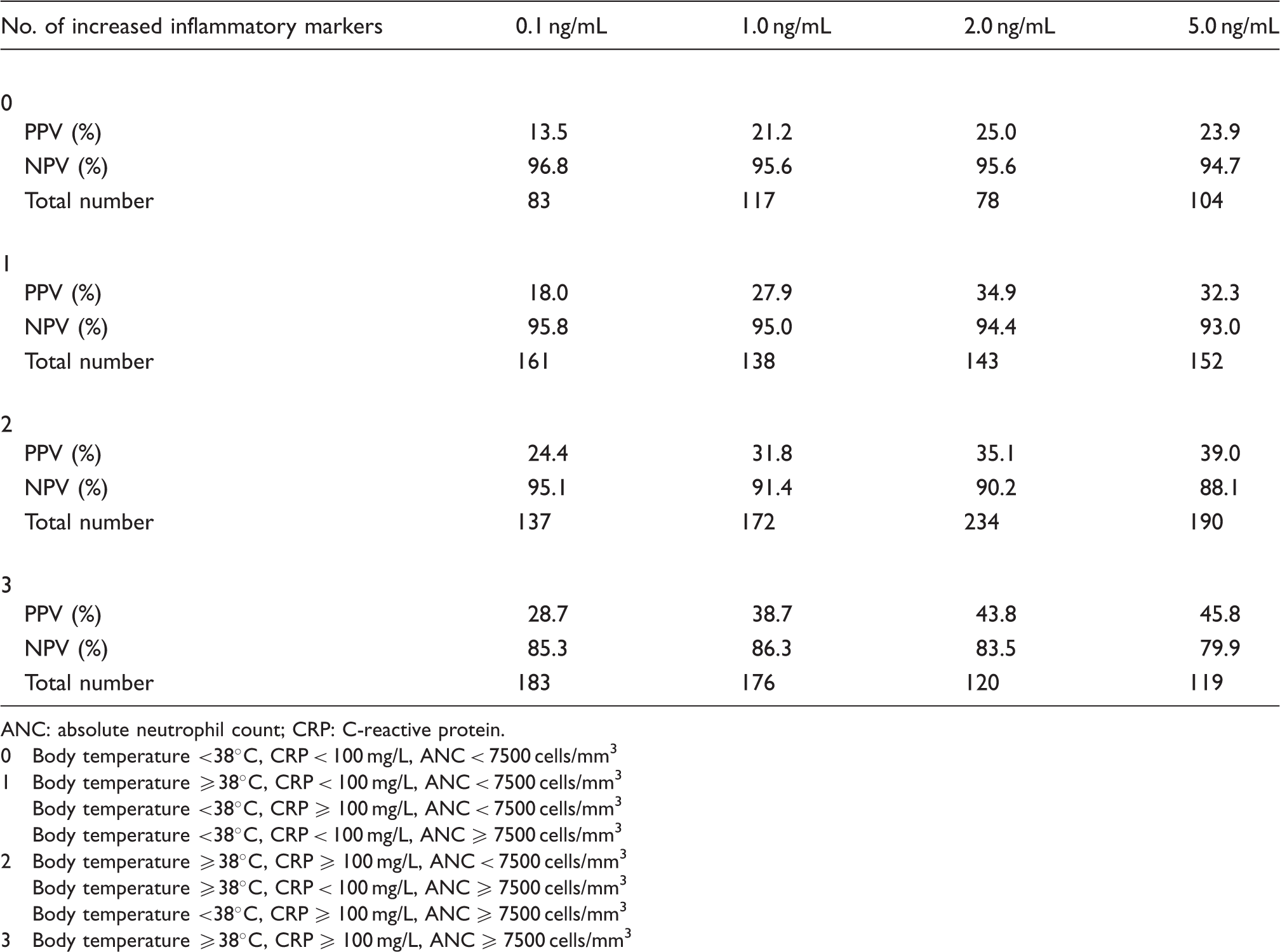
ANC: absolute neutrophil count; CRP: C-reactive protein. 0 Body temperature <38℃, CRP < 100 mg/L, ANC < 7500 cells/mm3 1 Body temperature ≥38℃, CRP < 100 mg/L, ANC < 7500 cells/mm3 Body temperature <38℃, CRP ≥ 100 mg/L, ANC < 7500 cells/mm3 Body temperature <38℃, CRP < 100 mg/L, ANC ≥ 7500 cells/mm3 2 Body temperature ≥38℃, CRP ≥ 100 mg/L, ANC < 7500 cells/mm3 Body temperature ≥38℃, CRP < 100 mg/L, ANC ≥ 7500 cells/mm3 Body temperature <38℃, CRP ≥ 100 mg/L, ANC ≥ 7500 cells/mm3 3 Body temperature ≥38℃, CRP ≥ 100 mg/L, ANC ≥ 7500 cells/mm3
Figure 1 shows ROC curves for the combination of three inflammatory markers and for this combination with PCT. The AUC for the combination of three inflammatory markers was 0.879. When PCT was added, the AUC was 0.932 (p = 0.018).
Receiver operating characteristic (ROC) curves are shown for the combination of PCT and other increased inflammatory markers. Top (red) line indicates area under ROC curved (AUC) of PCT + 3 inflammatory markers (0.932, 95% CI: 0.907–0.966) and middle (green) line of three inflammatory markers (0.879, 95% CI: 0.835–0.924).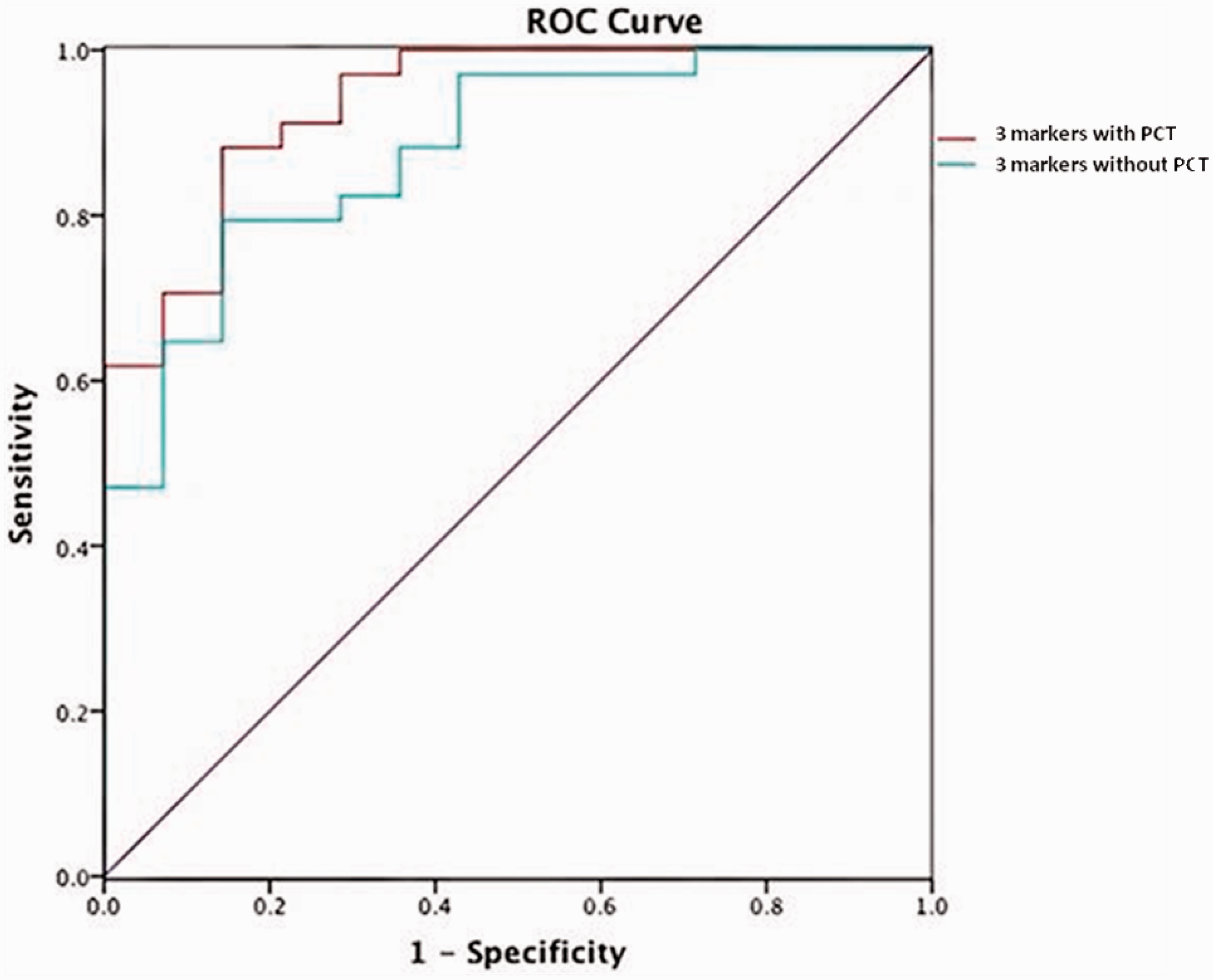
Discussion
This is a large-scale retrospective study of 3305 blood samples with suspected bacteraemia in our emergency department. When PCT cut-offs of 0.1–5 mg/dL were used to indicate bacteraemia, the PPVs were 21.2–37.0% and NPVs were 89.0–95.1%. Similarly, Chirouze et al. have reported that when PCT cut-off concentrations of 0.07–6.20 ng/mL were used to indicate bacteraemia, the PPVs were 14.3–31.3% and NPVs were 89.0–100%. 10 In addition, Kim et al. have reported that when PCT cut-off concentrations of 0.05–5.98 ng/mL were used, the PPVs were 14.0–48.0% and NPVs were 94.0–99.0%. 16 These two studies and two additional reports indicate that the PPV at which the PCT concentrations indicate bacteraemia is generally about 50%, although this will differ depending on the cut-off concentration, the patient group, and the hospital.9,11,16,17 In a recent meta-analysis of studies on bacteraemia markers, Jones et al. reported only moderate diagnostic performance for PCT as a single test for diagnosing bacteraemia in emergency department patients, demonstrating a sensitivity of 76% and a specificity of 73% at a cut-off concentration of 0.4–0.5 ng/mL. 8 PCT performed similarly in our present study, although the specificity of 0.5 ng/mL was lower.
Since the utility of PCT alone to predict bacteraemia was reported to be only moderate, 8 several other studies have also examined whether it can serve as an auxiliary marker. A study on 211 patients with a body temperature of ≥38℃ who presented at the department of internal medicine of a college hospital revealed that compared with PCT alone, PCT when used together with body temperature and CRP significantly increases the sensitivity at which bacteraemia could be diagnosed, although the PPVs did not differ significantly. 18 In the current study, various PCT cut-off values were used to assess its ability to predict bacteraemia on their own. The use of additional markers (body temperature, CRP, and ANC) increased the sensitivity, specificity, and PPVs compared with PCT alone; ANC ≥ 7500 cells/mm3 with PCT showed best sensitivity. Moreover, PCT improved the diagnostic discrimination of a combination of three existing markers of bacterial infection. The combination of PCT with body temperature, CRP, and ANC could differentiate between confirmed bacteraemia by blood culture and non-infectious fever with an AUC of 0.932.
Several studies have reported that PCT is a useful biochemical marker for ruling out bacteraemia.10,11,13,19 Riedel et al. reported that bacteraemia could be ruled out using a PCT cut-off value of <0.1 ng/mL with an NPV value of 96.3%. 9 This was also observed by Kim et al. (NPV 96.2%) 16 and Albrich and Mueller (NPV = 98.2%). 10 Consistent with these studies, the NPV in the present study was 95.1% at a PCT cut-off value of 0.1 ng/mL; the number of samples with PCT <0.1 ng/mL was 564 out of 3305.
In summary, when dealing with patients with suspected bacteraemia who present at the emergency department, it is important to determine promptly whether or not to administer antibiotics empirically; hence the need for clinical signs and serum markers that can permit accurate and rapid prediction of bacteraemia. The current study shows that when PCT is used as a serum marker for ruling out bacteraemia in adult patients, a cut-off value of 0.1 ng/mL can be used; if PCT is <0.1 ng/mL, then antibiotics may be withheld. When screening for bacteraemia, the addition of PCT to a combination of body temperature, CRP, and ANC improves diagnostic discrimination.
Footnotes
Acknowledgements
We would like to thank department of laboratory medicine for assistance and guidance in this research.
Declaration of conflicting interests
None declared.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Ethical approval
The ethics committee of Asan Medical Center in South Korea approved this study (REC number: 2012-0302).
Guarantor
W-KM.
Contributorship
S-YK, TDJ, WL, and SC researched literature and conceived the study. W-KM was involved in protocol development, gaining ethical approval, patient recruitment, and data analysis. S-YK wrote the first draft of the manuscript. All authors reviewed and edited the manuscript and approved the final version of the manuscript.