
Abstract
Background
B lymphocyte stimulation is described in human immunodeficiency virus (HIV) infection and results in ongoing immunoglobulin production with abnormal serum protein electrophoresis patterns. We hypothesized that serum protein electrophoresis patterns would be abnormal in untreated HIV subjects and correlate with markers of disease severity.
Methods
Serum protein electrophoresis was performed on 70 HIV-positive, clinically well treatment-naïve subjects and 42 HIV-negative controls and correlated with markers of disease severity, namely CD4+ counts, viral loads, IgG and albumin.
Results
The mean age for both groups was 33 years, and female-to-male ratios were 4:1. All were of Black ethnicity. Mean CD4 counts ± SD for HIV group and controls were 419.5 ± 218.6 and 960.4 ± 378.5 cells/mm3, respectively. Of the HIV-infected group, 44% showed polyclonal hypergammaglobulinaemia versus 10% of controls (P < 0.01). The HIV group had 27% with an abnormal pattern requiring immunofixation which revealed nine (12.5% of total) had oligoclonal bands, seven (10.3% of total) had polyclonal hypergammaglobulinaemia and three (4% of total) had monoclonal bands. CD4+ counts were lower in those with polyclonal hypergammaglobulinaemia or abnormal serum protein electrophoresis. Interestingly, viral load results showed no statistically significant differences.
Conclusion
We found a remarkably high level (53%) of polyclonal hypergammaglobulinaemia in our untreated population compared with uninfected controls (10%). Only 4% of the HIV-positive group had a monoclonal band. Polyclonal hypergammaglobulinaemia correlated significantly with lower CD4+ counts. These results highlight the generalized B cell stimulation in untreated HIV infection. Future longitudinal studies will be important to determine the prognostic value of these findings.
Keywords
Background
Human immunodeficiency virus (HIV) infection is characterized by persistent immune activation which is a major contributing factor to increased mortality, even in antiretroviral treatment (ART)-treated individuals. 1 HIV and other co-infections, together with leakage of microbial products from the damaged gut mucosa into the systemic circulation, all contribute to the ongoing stimulation of both the innate and adaptive immune systems.2,3
In HIV infection, CD4+ T cells decrease, leading to impaired B-T cell interactions and B lymphocyte dysfunction which results in the ongoing production of immunoglobulins. Activated CD4+ T cells interact with B lymphocytes to induce immunoglobulin switching from IgM to IgG. Therefore, HIV infection is characterized by polyclonal hypergammaglobulinaemia, and concentrations of IgG in particular have been shown to be increased in untreated individuals. 4 Multiple B cell abnormalities have been described which ultimately predispose patients to the development of lymphomas.5,6
Early studies showed a high prevalence of monoclonal, oligoclonal and polyclonal gammopathies in HIV;7–9 however, recent work has indicated a lower prevalence.10–12 This is likely due to the efficacy of ART in improving the B cell dysfunction. B cells also benefit indirectly by improved B-T cell interactions due to improved CD4 counts.5,13,14 A direct effect of virus replication or viral proteins on B cell function has also been described.15,16
We hypothesized that serum protein electrophoresis (SPE) patterns would be abnormal in an untreated HIV cohort and would correlate with markers of disease severity. To our knowledge, this is the first study to examine the SPE patterns in ART-naïve, newly diagnosed HIV-infected subjects.
Methods
Subjects
This was a retrospective cross-sectional study. SPE was performed on 72 HIV-positive subjects; clinically well and not on ART and 42 HIV-negative controls recruited from the Voluntary Testing and Prevention clinic, Emavundleni in Crossroads, Cape Town, Western Cape, South Africa. This is a clinic attached to the Institute for Infectious Diseases, Desmond Tutu HIV centre, University of Cape Town (UCT). At the end of 2012, an estimated 6.1 million people in the Republic of South Africa were living with HIV with a prevalence of 17.9% among adults aged 15–49 years – the highest number of people in any country. Of these, 18.2% reside in the Western Cape. The samples used for this study were collected for a previous study and immediately processed and stored at −70℃. When this study was performed, they had been stored for less than a year.
Inclusion criteria
Patients >21 years of age with HIV infection and CD4+ counts >200 cells/mL were recruited. All were treatment-naïve.
Controls were recruited from those >21 years tested without HIV infection.
Exclusion criteria
Patients with tuberculosis (TB) or other co-infections and those receiving ART, anti-TB treatment or other antibiotic treatment were excluded. Pregnant women were also excluded.
Ethical consideration
The study was carried out in accordance with the Declaration of Helsinki and ICH GCP guidelines. The study protocol was submitted for ethical approval by the University of Stellenbosch Ethics Committee, which had already approved previous studies of the same origin (HREC NO 07/09/197). All patients signed an informed consent form explaining what tests would be performed and that confidentiality would be maintained at all times. Specimens were identified by means of allocated study numbers.
Procedures
Total protein used for quantifying the various electrophoretic fractions by densitometry was determined on the ADVIA™ 1800 clinical chemistry analyzer using the biuret method according to the manufacturers recommended protocol (Siemens, Erlangen, Germany). SPE was performed on the Sebia® hydrasys®2 which is a semi-automated electrophoresis instrument. These results were then correlated with markers of disease severity in HIV, namely CD4+ counts, viral loads, IgG and albumin. IgG was determined on the ADVIA™ 1800 clinical chemistry analyzer (Siemens Erlangen, Germany). Albumin and gamma fractions were determined densitometrically from the SPE using agarose gel electrophoresis. The SPE results were evaluated by three blinded independent chemical pathologists. Flow Cytometry for CD4+ T-cell counts was performed on whole blood using the BD MultiTEST™ CD3-FITC/CD8-PE/CD45-PerCP/CD4-APC reagent together with BD TruCOUNT tubes (BD Biosciences, San Jose, CA). HIV-1 RNA quantifications were performed on plasma with use of the Nuclisens Easy Q HIV-1 v.1.2 (BioMerieux Inc., Boxtel, Netherlands) kit, an assay with a lower detection limit of 40–50 copies/mL.
The SPE results were classified as follows.
Normal – normal SPE protein band distribution Polyclonal hypergammaglobulinaemia – increased SPE gamma fraction but no definite bands identified Abnormal – increased SPE gamma fraction with suspicion of a monoclonal or oligoclonal bands on polyclonal background; for which immunofixation was performed
Statistical analysis
The data were analysed, using STATISTICA version 10 (StatSoft Inc.) and Microsoft® Excel®. The calculations were performed in STATISTICA, and Microsoft® Excel® was used to graphically display the results of the calculations. Descriptive statistics were used to analyse each parameter in terms of distribution, mean, maximum and minimum values and standard deviation. Continuous variables were compared against each other using regression and correlation analysis. For data with a normal distribution, Pearson’s correlation coefficient was performed. For data with non-normal distribution, the Spearman rank correlation coefficient was used.
Results
The mean age for both groups was 33 years (range 21–60 years), and most subjects were aged between 20 and 50 years. The female-to-male ratios were similar for both groups (4:1). All were of Black ethnicity.
Levels of total protein, albumin, IgG, CD4 counts and viral loads in the two groups.
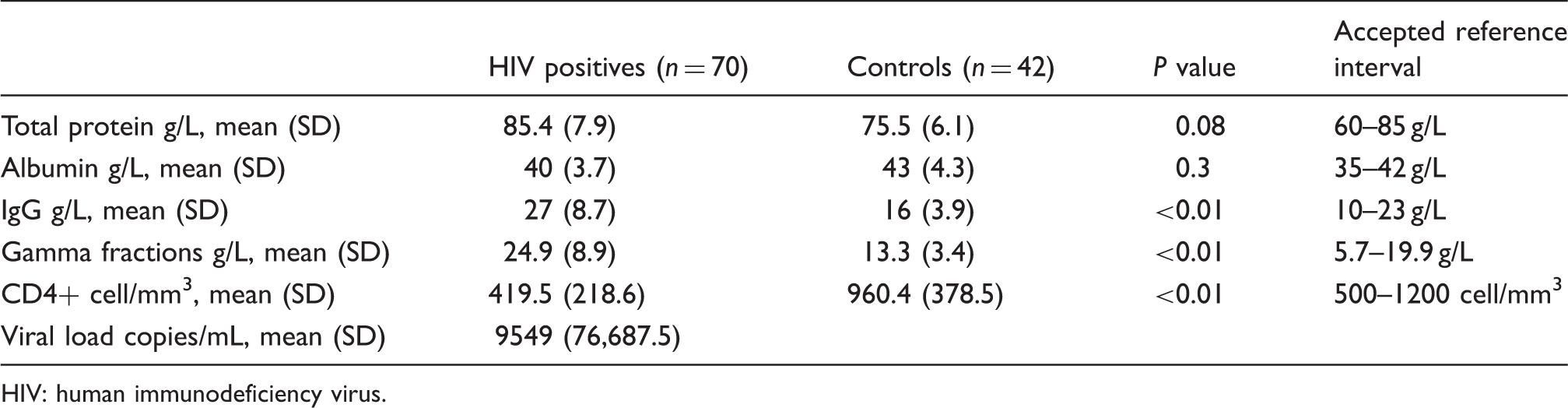
HIV: human immunodeficiency virus.
Electrophoretic patterns in the various groups.
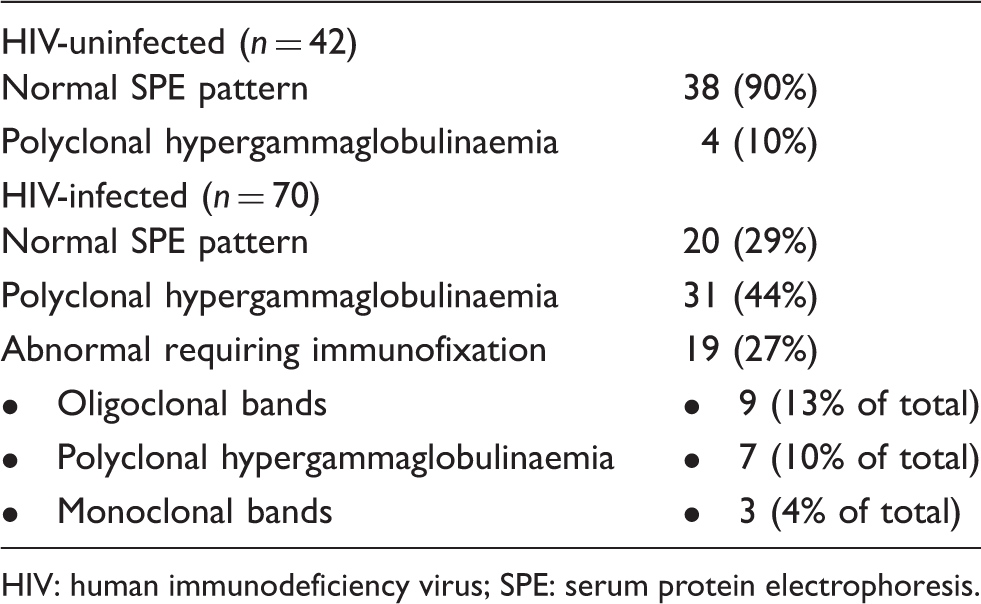
HIV: human immunodeficiency virus; SPE: serum protein electrophoresis.
Measures of HIV disease severity in the various electrophoretic patterns.
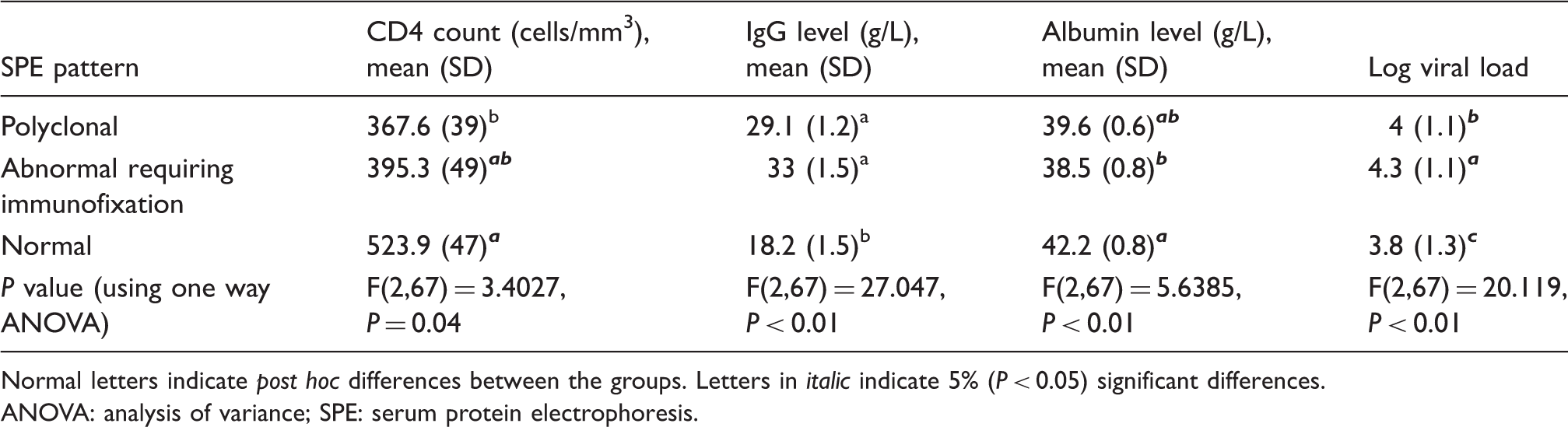
Normal letters indicate post hoc differences between the groups. Letters in italic indicate 5% (P < 0.05) significant differences.
ANOVA: analysis of variance; SPE: serum protein electrophoresis.
Discussion
We have shown a remarkably high level of abnormal SPE patterns in our untreated HIV-infected population (71%) compared with uninfected high-risk controls (10%). Of this 71%, 44% had a polyclonal hypergammaglobulinaemia and 27% had an abnormal pattern requiring immunofixation to exclude a monoclonal band. Only 4% overall of the HIV-positive group (3 or 15% of the abnormal patterns) was eventually found to have a monoclonal band. The other abnormal patterns were found to be either oligoclonal bands on a polyclonal background or polyclonal hypergammaglobulinaemia. In support of our findings of high levels of abnormal SPEs in untreated patients, an early study by Sinclair et al. examining HIV-infected and at-risk HIV-negative subjects found an increased incidence of abnormal SPE (61% versus 37%). However, that study noted that patients with oligoclonal bands and those with monoclonal gammopathy of undetermined significance had a higher risk of developing plasma cell tumours; 17 whereas in the current study, we investigated the value of polyclonal hypergammaglobulinaemia as a marker of generalized B cell stimulation in untreated HIV infection.
A previous study in our hospital found that 3.2% of subjects had monoclonal bands and 3.8% had oligoclonal bands. 12 However, these were subjects being followed up at the clinics, and most were already on ART. In support of our study findings of a low incidence of monoclonal bands, Lefrere et al. screened 243 HIV-infected subjects not on treatment and found that six (2.5%) had monoclonal bands. Most of these bands were IgG subtype (kappa more than lambda). 18 In addition, Crapper et al. 7 published a study showing that 4.6 % of HIV subjects had monoclonal bands and 4% had oligoclonal bands on SPE. However, these early studies were performed on a different population to ours, namely homosexual men. A 2-year follow-up of these subjects found that the monoclonal bands had no prognostic significance and were not predictive of outcome. 19
More recent studies have also found a low incidence of monoclonal bands. In 2007, Konstantinopoulos et al. 20 studied HIV-positive subjects on ART and found that 8.1% had oligoclonal bands and 4.4% low-concentration monoclonal bands and 1.9% had polyclonal increases on SPE. However, these subjects were on ART as opposed to ours which were treatment-naïve and clinically well. The significance of these bands is uncertain. Dezube et al. 21 described that these subjects may be more likely to progress to multiple myeloma. Salarieh et al. 22 found that these subjects have an increased incidence of plasma cell tumors which may be more aggressive and have an atypical presentation. However, Pontet et al. 9 performed a long-term follow-up and found that these abnormal electrophoretic patterns had no significant prognostic value. Ng et al. 23 and Lefrere et al. 24 also found that these patterns were of no prognostic value and postulated that they may just be a normal response to HIV antigens. Most of these studies show that the most common monoclonal band is IgG kappa, which agrees with our findings.
In our study, a polyclonal hypergammaglobulinaemia correlated significantly with a lower CD4 count and therefore may be a valuable prognostic marker. Albumin was also decreased in the abnormal electrophoresis group, but less so in the polyclonal hypergammaglobulinaemia group. An important finding was the lack of association of viral load with any of the SPE groups (P = 0.49). This would suggest that viral load is not the underlying cause for the stimulation of B cells in this HIV-infected group, and further supports the concept of generalized immune activation as an important driving force in disease progression.
It was interesting to note the high level of polyclonal hypergammaglobulinaemia patterns (10%) detected in the uninfected control group in our study. This may reflect the higher antigen burden in our setting.
An important limitation of our study is that we relied on a clinical history alone to exclude TB and other infectious diseases and did not do specialized tests. Although TB affects the cellular arm of immunity predominantly, it may be associated with polyclonal hypergammaglobulinaemia on SPE. Another potential limitation is that the interpretation of SPE may be subjective; therefore, we ensured that the SPEs were interpreted blindly by three independent chemical pathologists and found good interobserver correlations. A further limitation may be that albumin was determined densitometrically and not colourometricaly which may have also affected the results. An important strength of our study was that these subjects were clinically asymptomatic with relatively well-maintained CD4 counts and therefore not yet on ART. This enabled important B cell abnormalities to be documented at this stage of the disease.
Conclusion
Our results highlight the generalized B cell stimulation that occurs in untreated HIV infection and show the important correlation of polyclonal patterns with lower CD4 counts. Future longitudinal studies will be important to determine the prognostic value of SPE in the development of acquired immunodeficiency syndrome or B cell lymphomas.
Footnotes
Acknowledgements
We wish to thank the patients and staff of the Emavundleni Prevention Centre of the Desmond Tutu HIV Centre in Crossroads Cape Town for their participation in this study and particularly Dr Surita Roux for her involvement and co-ordination. In addition, we would like to thank Professor Martin Kidd for his aid in the statistical analysis of the results and Dr M Hoffmann and Dr C Meyer for their help in interpreting the serum protein electrophoreses.
Declaration of conflicting interests
None declared.
Funding
This research was supported by the National Health Laboratory Services Research Trust, South Africa; the Poliomyelitis Research Foundation (PRF), South Africa; the Department of Science and Technology of South Africa (through the SHARP initiative) and the Harry Crossley Foundation.
Ethical approval
The study was approved by the ethical committees of the University of Stellenbosch (HREC N07/09/197) and the University of Cape Town (REC 417/2006).
Guarantor
AEZ.
Contributorship
HI and AEZ conceived and designed the study. HI was involved in gaining ethical approval and patient recruitment. SM, AEZ and RTE researched the literature, and AEZ wrote the first draft of the manuscript. All authors reviewed and edited the paper and approved the final version.