
Abstract
The case of a 50-year-old man who died mysteriously after being admitted to hospital is reported. He had raised the possibility of being poisoned prior to his death. A Coroner’s post-mortem did not reveal the cause of death but this was subsequently established by post-mortem trace element analysis of liver, urine, blood and hair all of which revealed very high arsenic concentrations.
Keywords
Introduction
In the past, arsenic has been a popular choice of poison used for suicide and homicide; however, more recently its availability in UK and USA has been restricted. Only two cases of intentional arsenic poisoning have been reported in the western literature since 1992.1,2 We present a recent case of unexplained sudden death. The case was reported to the Procurator Fiscal (Scottish equivalent to the Coroner), and a diagnostic forensic process was instigated that supported the conclusion that the man died as a direct result of maleficent arsenic poisoning.
Case report
A 50-year-old man of Pakistani origin who had been living in Saudi Arabia with relatives for three months, presented with a six-week history of diarrhoea and vomiting. He also reported general malaise, abdominal tenderness, mild fever, numbness in his arms and legs and blurring of vision. He had lost approximately 15 kg in weight. When his symptoms began, he had volunteered to his partner, a nephew and a friend that he thought he may have been poisoned as he had felt unwell following a meal.
He returned to the UK via Pakistan where he again visited relatives. In Pakistan, he presented to a local hospital with diarrhoea and vomiting. He was diagnosed with Helicobacter pylori infection and was commenced on H. pylori eradication therapy. After returning to the UK and around seven weeks after the onset of his illness, he presented to his GP with diarrhoea, vomiting and a tender abdomen. The patient was referred to hospital.
There was no significant medical history, but the patient had been shot in the leg, allegedly by a relative during a trip to Pakistan around a year before his death.
On general examination, he looked well. His temperature, pulse, blood pressure, respiratory rate and oxygen saturations were normal. He had moderate tenderness over the right hypochondrium.
Laboratory findings on admission showed pancytopenia and deranged liver function tests (reference ranges in parentheses): haemoglobin 117 g/L (130–180 g/L), white blood cells 1.0 × 109/L (4–11 × 109/L); platelets 95 × 109/L (150–400 × 109/L); mean cell volume 80 fL (78–99 fL); neutrophils 0.4 × 109/L (2–7.5 × 109/L); lymphocytes 0.4 × 109/L (1.5–4 × 109/L); vitamin B12 1053 ng/L (200–900 ng/L); folate 4.3 µg/L (3.1–20 µg/L); ferritin 422 µg/L (10–275 µg/L); urea 10.3 mmol/L (2.5–7.8 mmol/L); creatinine 122 µmol/L (40–130 µmol/L); total bilirubin 46 µmol/L (<20 µmol/L); alkaline phosphatase 70 U/L (30–130 U/L); aspartate aminotransferase 78 U/L (<40 U/L); alanine aminotransferase 103 U/L (<50 U/L); calcium 2.15 mmol/L (2.2–2.5 mmol/L); phosphate 1.83 mmol/L (0.8–1.5 mmol/L); C-reactive protein 16 mg/L (<10 mg/L); lactate 1.5 mmol/L (0.5–2.2 mmol/L); and amylase 98 U/L (<10 U/L).
Tests for HIV-antigen/antibody, hepatitis Bs-antigen, hepatitis C antibody, malaria blood film and antigen, anti-nuclear antibodies, mitochondrial antibody and smooth muscle antibody were all negative. A blood film showed moderate anisocytosis with some polychromasia. There was marked leucopenia and thrombocytopenia. The chest X-ray was normal. Abdominal ultrasound reported a trace of free fluid within the pelvic cavity. An electrocardiography was scheduled for the following morning; however, that morning the patient was found deceased hanging over the side of his bed. The patient was already cold and resuscitation was not attempted. The case was referred to the Procurator Fiscal (Scotland), and a post-mortem examination was instructed.
At post-mortem, there were few pathological findings. External examination revealed petechial haemorrhages in and around the eyes, in the mouth and over the trunk and right upper arm and an area of darker brown discolouration of the skin over the back. Internally, there were bilateral pleural effusions, the trachea contained a large amount of frothy fluid and there was non-specific pulmonary congestion and oedema. The liver was congested reflecting the deranged liver function tests, and there was focal reddening of the lining of the ascending colon, the remainder of the gastrointestinal tract being normal. Microscopy revealed very occasional contraction bands in the myocardium and some scattered mixed inflammatory cells in the liver sinusoids, but no unequivocal hepatocyte necrosis. Several oval scars were present on the front of each thigh. The entire body was X-rayed prior to post-mortem, and pieces of lead shot were subsequently retrieved from the right thigh and scrotum. No Geiger counter was used.
Concentrations of arsenic species in a post-mortem urine sample.
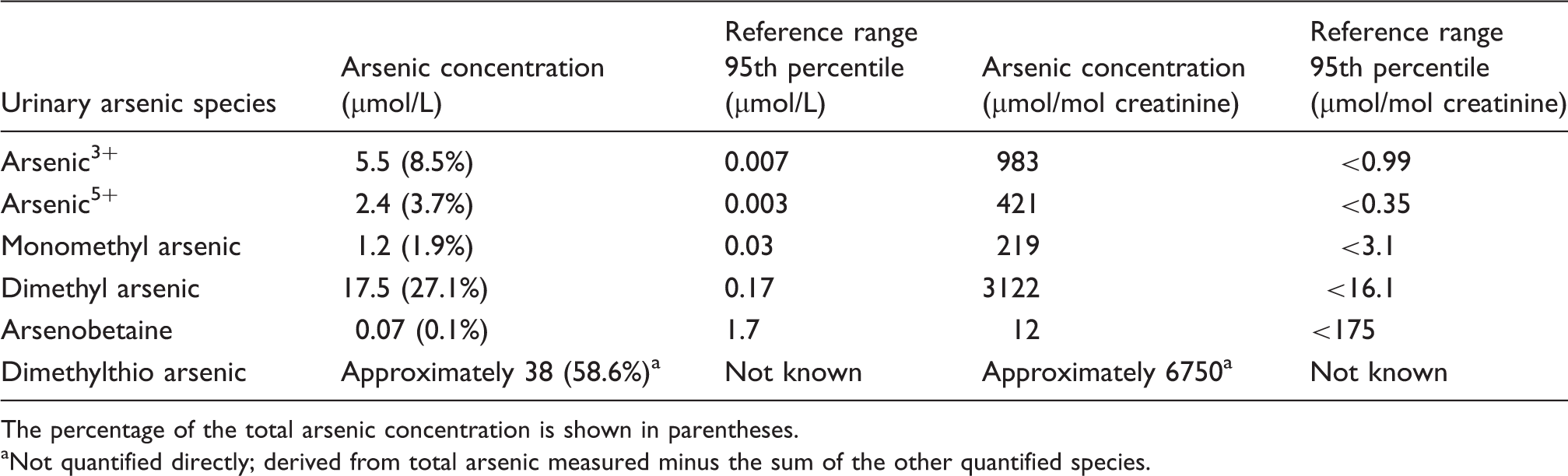
The percentage of the total arsenic concentration is shown in parentheses.
Not quantified directly; derived from total arsenic measured minus the sum of the other quantified species.
Speciation of arsenic in urine was performed by micro flow liquid chromatography coupled to ICP-MS
3
(see Figure 1). The peak fraction which was unidentified was collected by high-performance liquid chromatography and analysed by micro liquid chromatography-ICP-MS and electro-spray ionisation-tandem mass spectrometry. The mass spectrum of this peak showed a fragmentation pattern that was similar to the mass spectrum obtained from dimethylthioarsenic ((CH3)2As(S)O). The mass spectrum results are also consistent with a previous study of dimethylthioarsenic identification.
4
Arsenic speciation chromatogram of post-mortem urine sample. DMA: dimethylarsinous acid.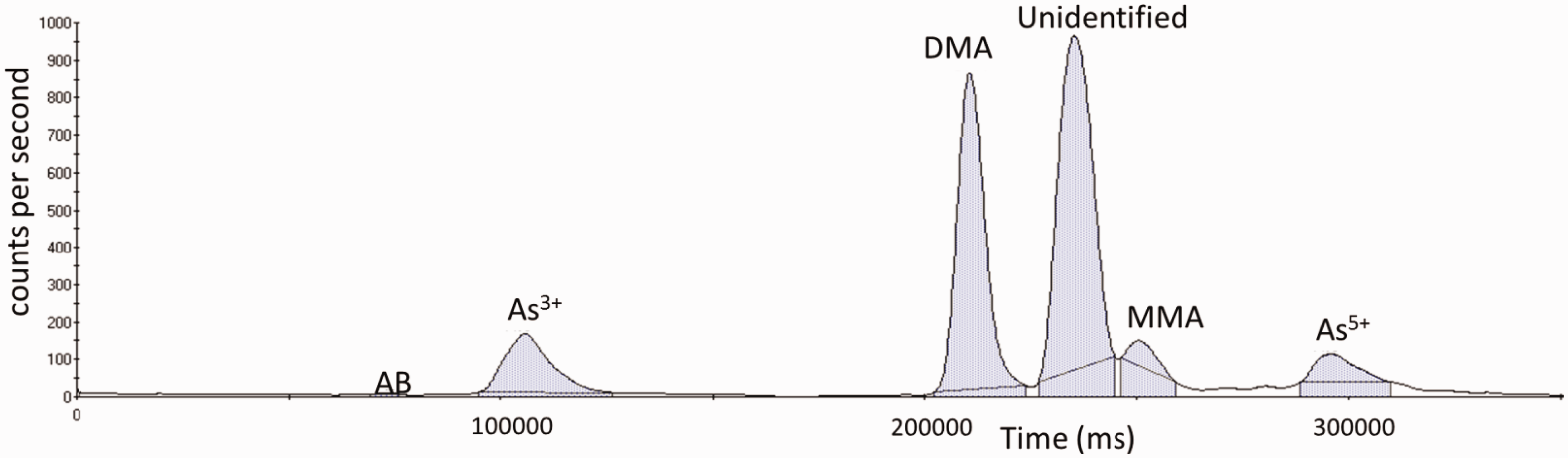
Discussion
This patient’s blood arsenic result of 7 µmol/L was substantially higher than our upper reference limit of 0.135 µmol/L but considerably lower than other fatal cases of arsenic poisoning, for example 96 µmol/L 5 in one case, an average of 49 µmol/L (range: 4 to 267 µmol/L) reported in a series of 19 victims 6 and 144 µmol/L (range: 8 to 1802 µmol/L) in a subsequent series of 18 victims. 7 However, the time from poisoning to blood collection was not quoted in these studies and since the half-life of arsenic in vivo is around 48 h, 8 blood concentrations fall quickly. Consequently, blood taken on the day of poisoning shows much higher concentrations than samples taken several days later as was the case in the present report in which three days passed between leaving Pakistan and his death.
Urine arsenic concentrations fall quickly after a single arsenic exposure9,10 and so interpretation is difficult. The victim had a post-mortem urine arsenic concentrations of 65.4 µmol/L compared to 49.9 µmol/L found in another fatal case although in the current case, the time from exposure was indeterminate and in the latter was not recorded. In two other severe but ultimately non-fatal cases, concentrations of 70.8 and 77.4 µmol/L were found on the day of exposure. 11 A concentration of 2777 µmol/L was found in one non-fatal case in which the sample was collected the day after poisoning 12 and in a failed suicide attempt the urine concentration was found to be 734 µmol/L only 3–4 h after exposure. 13 Even with relatively low arsenic exposure, urine concentrations may be high in urine that has been collected soon after ingestion; for example, six healthy volunteers had urine arsenic concentrations of up to 37 µmol/L 10 h after a relatively small bolus dose of 6 mg arsenic trioxide. 14
The main factors affecting arsenic concentrations in blood and urine are the time from poisoning to sample collection and the amount of arsenic consumed. Unfortunately, very few publications document the former and the latter is rarely known. Since the half-life of arsenic in these samples is very short, concentrations will decrease rapidly over a brief time period. For this reason, it is only possible to make limited inferences from blood and urine concentrations.
The incorporation of trace elements in hair, fingernails (not collected in this case) and liver is more likely to be in proportion to the systemic burden and so comparison of arsenic concentrations in these tissues with reported fatal poisonings is likely to be a more reliable means of assessing degree of exposure.
Measurement of trace elements in longitudinal sections of hair has been used to gauge the approximate time course of exposure using the known growth rate of hair per month. Acute arsenic poisoning may be associated with excessive sweating, and in such cases, concentrations of arsenic in hair may be due to contamination of arsenic in sweat as well as incorporation systemically so making interpretation more difficult. 15 However, in the current case, excessive sweating was not reported and so longitudinal hair analysis was undertaken. A head hair arsenic concentration of 71 µg/g (reference values <0.15 µg/g 16 ) was found in the 3-mm head hair sample cut closest to the scalp. This is high and in keeping with previous reports of fatal arsenic poisonings, for example 10, 94, 147 and 400 µg/g found in four cases17,18 and results from 28 to 226 µg/g and 7.4 to 37 µg/g in sections along the length of hair in two case reports.17,19 The victim’s hair was 25 mm long representing around the last 10 weeks of his life based on an average growth rate of approximately 10.6 mm/month. 20 Arsenic concentrations were high along the length suggesting he had been poisoned over this entire time period. This is in accord with the duration of his symptoms which started approximately 70 days before his death. Unfortunately, his hair was not long enough to give an indication of when the exposure started. The arsenic concentrations increased incrementally from the distal end along the 3 mm lengths of hair analysed, suggesting that the amount of arsenic absorbed increased over time. This is also consistent with the chronic presentation of his symptoms.
The liver arsenic concentration in this case was 39 µg/g (reference range: <0.013 µg/g 21 ). Previous reports of fatal arsenic poisoning reported liver concentrations of 15 µg/g, 5 30 µg/g, 22 226 µg/g, 19 147 µg/g 23 and an average of 81.7 µg/g (range: 5 to 400 µg/g) in a series of 19 cases. 7
The arsenic concentrations found in the blood, urine, liver and hair tissues collected are therefore in keeping with previously reported cases of fatal arsenic poisoning. Such concentrations could be achieved accidentally through inadvertent exposure from food, water, medication or in the workplace. However, the victim was a businessman and not occupationally exposed in processes, such as semiconductor manufacture, academic research, use of arsenic containing wood preservative or other work in which arsenic is used, nor was he being treated with an arsenical medication. 24
The concentration of arsenic is negligible in foodstuffs with the exception of seafoods in which it may be as high as 27 µg/g in the case of oysters and 40 µg/g in seabass. Consequently, following a fish or shellfish meal, high concentrations in excess of 13 µmol/L 23 and 29 µmol/L 25 (reference limit <0.25 µmol/L) have been reported. The main food sources of arsenic are in the form of non-toxic compounds; arsenobetaine and arsenocholine in fish and shellfish and arsenosugars in seaweed. Arsenobetaine is rapidly excreted unchanged in the urine, 26 and while arsenocholine and arsenosugars are metabolised, toxic inorganic arsenic species are not among the metabolites. 13 The results from the urine speciation undertaken in this case show arsenobetaine in relatively low concentrations so excluding seafood as the source of arsenic.
The high concentrations of inorganic As3+ and As5+ are suggestive of exposure to inorganic arsenic. There is individual variation in the ability to methylate inorganic arsenic, and there may be a difference in methylation processes depending on the route of exposure. In an attempted suicide attempt using arsenic trioxide, trivalent arsenic was the major peak but in an inhaled dust exposure more that 50% of the total arsenic was methylated in the urine sample. 25 In the present case, very high concentrations of both monomethyl arsenic and dimethyl arsenic were detected indicating considerable detoxification of inorganic arsenic by methylation had occurred. The unidentified peak was thought to be dimethylthioarsenic which has a high degree of cytotoxicity being possibly more toxic than arsenite. 27 Although biological pathways are not fully understood, current research suggests dimethylthioarsenic is produced following exposure to inorganic arsenic. 28
The victim had spent time in Pakistan where concentrations of inorganic arsenic in water from bore wells are elevated compared to the UK.29,30 For example, in a report of 330 Pakistani subjects, the median urine concentration was 1.6 µmol/L in exposed individuals but these ranged up to 28.9 µmol/L (2166 µg/L). 31 In another study, urine concentrations as high as 24.6 µmol/L were found. 32 Although urine arsenic concentrations are usually lower than those found in fatal poisoning, on occasions this is not the case. However, individuals imbibing arsenic in drinking water over long time periods have chronic exposure resulting in skin pigmentation, keratosis and increased risk of skin cancer.33,34 In addition, an inconceivably high volume of water would have to be drunk in order to accumulate an acute lethal dose estimated to be 100 to 300 mg 35 ; in the two studies mentioned above, the maximum arsenic concentrations in water were 332 µg/L and 1840 µg/L. Rice grown and cooked in arsenic-containing water has also been shown to have high inorganic arsenic concentrations (up to 482 µg/g). 36 However, again this would result in chronic arsenic poisoning and unrealistically large quantities of rice would require to be eaten to attain a lethal dose.
The natural history of the case presented is in keeping with an acute arsenic poisoning which is associated with symptoms of nausea, vomiting, diarrhoea and often abdominal pain, tachycardia and profound hypotension. 15 The victim also gave a history of weight loss and peripheral neurological symptoms which have also been described in previous cases of fatal arsenic poisoning.12,19 His apparent wellness prior to his sudden death is also consistent with arsenic poisoning since death may be preceded by a period of perceived wellness.11,13,17
In the case presented, there were relatively few post-mortem findings compared with previous cases in which generalized oedema, congestion and fluid accumulation of visceral organs and haemorrhagic inflammatory changes in the gastrointestinal tract have been reported.6,17,19 This case differs in that the longitudinal hair arsenic concentrations indicate that poisoning took place over an extended time period whereas most post-mortem reports in cases of arsenic poisoning have been reported following death from acute exposure.
In order to conclude that arsenic poisoning is as a result of intentional poisoning, three specific criteria must be satisfied: that arsenic is present in toxic concentrations in tissues, its presence could not be accounted for by alternative incidental possibilities and that the observed symptoms are consistent with previously reported fatal cases. 37 In this case, all the three conditions were satisfied and so it was concluded that death was a result of intentional fatal arsenic poisoning. Arsenic is readily purchased in the countries the patient had visited being the toxic agent in many rodenticides. Arsenic poisoning occurred over a period of around two months making suicide unlikely.
Footnotes
Acknowledgements
Dimethylthioarsenic was synthesised and kindly gifted by Kevin Francesconi (University of Graz, Austria).
Declaration of conflicting interest
None.
Funding
None.
Ethical Approval
The North Glasgow Hospitals Trust Ethics Group confirmed that ethical approval was not required.
Guarantor
AD.
Contributorship
AD performed the initial arsenic analysis and wrote the manuscript. JM and EL provided ![]() and performed the speciation analysis and checked the final manuscript. AT provided expert advice and checked the manuscript. JMcA provided forensic and post-mortem information and checked the final manuscript. SA provided clinical information and checked the final manuscript.
and performed the speciation analysis and checked the final manuscript. AT provided expert advice and checked the manuscript. JMcA provided forensic and post-mortem information and checked the final manuscript. SA provided clinical information and checked the final manuscript.