
Abstract
Acute promyelocytic leukemia, a subtype of acute myeloid leukemia, is highly curable. In subgroup of patients with non-high-risk acute promyelocytic leukemia, intravenous arsenic trioxide plus all-trans-retinoic acid is considered the preferred regimen for acute promyelocytic leukemia. Recently, there are interests in the use of the oral form of arsenic, named the Realgar-Indigo naturalis formula, but the data on its efficacy and safety are still relatively limited. The current study was conducted with the aims to identify and summarize the results of all available randomized-controlled studies. A systematic review was conducted in the 2 major databases, utilizing the terms for arsenic and acute promyelocytic leukemia. Eligible studies had to be randomized-controlled studies that compared efficacy and/or adverse effects of oral arsenic versus intravenous arsenic for treatment of patients with acute promyelocytic leukemia. The Mantel-Haenszel method was used to pool the effect estimates and 95% confidence intervals of the included studies together. A total of 4 randomized controlled studies with 482 patients with acute promyelocytic leukemia (258 in Realgar-Indigo naturalis formula group and 224 in intravenous arsenic trioxide group) were included in the meta-analysis. The chances of achieving complete remission were numerically higher in the Realgar-Indigo naturalis formula group but the difference was not statistically significant (pooled odds ratio: 4.59, 95% CI: 0.74-28.57, I 2 = 0%). Similarly, other efficacy outcomes, including 30-day mortality rate, overall survival, and event-free survival, also tended to favor the Realgar-Indigo naturalis formula group but the difference was not statistically significant. There was no significant difference in the chance of developing differentiation syndrome, cardiac complications, grades 3 to 4 liver toxicity, grades 3 to 4 renal toxicity, and infection between the 2 groups. The results may suggest that all-trans-retinoic acid plus oral Realgar-Indigo naturalis formula regimen is, at minimum, not a worse alternative to the standard all-trans-retinoic acid plus intravenous intravenous arsenic trioxide regimen for treatment of acute promyelocytic leukemia, especially for patients with low-to-intermediate risk.
Introduction
Acute promyelocytic leukemia (APL) is a subtype of acute myeloid leukemia that is highly curable. The standard treatment for APL, combination of all-trans-retinoic acid (ATRA) and chemotherapy, yields a high rate of complete remission (CR) and can reduce the rate of disseminated intravascular coagulation. 1 However, in the subgroup of patients with non-high-risk APL, defined as white blood cell at diagnosis <10 000/μL, 2 arsenic trioxide (ATO) plus ATRA is considered the preferred regimen because studies have demonstrated that patients who received ATRA plus ATO had a higher rate of CR, event-free survival (EFS), and overall survival (OS) as well as a lower cumulative incidence of relapse (CIR) than those who received ATRA plus chemotherapy. 3 -5 In fact, the National Comprehensive Cancer Network guideline recommends ATRA in combination with intravenous ATO as the preferred induction regimen for patients with low-risk APL (and recommends ATRA plus anthracycline-containing chemotherapy as an alternative). 6 The major concern for the treatment with ATRA and/or ATO is the development of a life-threatening complication, the APL differentiation syndrome, which can occur during the first days or weeks of treatment.
More recently, there are interests in the use of the oral form of arsenic, named the Realgar-Indigo naturalis formula (RIF). Studies have suggested that the ATRA plus oral RIF regimen has a comparable efficacy to ATRA plus intravenous ATO regimen 7 -10 but is associated with a lower medical cost and shorter length of hospital stay. 7,11 Nonetheless, the data on the efficacy and safety of oral RIF are still relatively limited and, therefore, its role in treatment of APL is still not well-established. 6 The current systematic review and meta-analysis was conducted with the aims to identify and summarize the results of all available randomized-controlled studies that compared the efficacy and/or adverse effects of ATRA plus oral RIF regimen versus ATRA plus intravenous ATO regimen in patients with APL.
Materials and Methods
Data Sources and Searches
The search strategy, which is provided as Supplementary Data 1, involved 2 investigators (NS and WO) independently searching for studies published before October 10, 2018 in the MEDLINE and EMBASE databases. The search terms used were the terms related to arsenic and APL. The references of the included studies were also manually reviewed to identify further eligible studies. This meta-analysis was compiled in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses statement, which is available as Supplementary Data 2. 12
Selection Criteria and Data Extraction
Studies that are eligible for the meta-analysis must fulfill the following criteria: (1) randomized-controlled studies that compared the efficacy and/or adverse effects of oral versus intravenous arsenic for treatment of APL and (2) reported any of the outcomes of interest, which could be either efficacy (CR, induction mortality, EFS, OS, or CIR) or adverse effects (the rate of differentiation syndrome after induction therapy, the rates of cardiac events, grades 3-4 liver toxicity, grades 3-4 renal toxicity, infection during treatment, bleeding events, or thrombotic events). We excluded nonrandomized studies, observational studies, case series, case report, and review. This process of determination of eligibility was independently performed by the same 2 investigators. If different decisions regarding the eligibility of a particular article were made, the article in question was jointly discussed with the third investigator (NJ) until a consensus decision was reached.
A standard study record form was used by the 2 investigators in order to extract the publication information, methodology, baseline characteristics of participants, and the outcomes of interest from each of the included studies. The 2 investigators performed this process independently, and the extracted data were subsequently cross-checked to ensure accuracy.
Outcome Definitions
The CR criteria included a bone marrow blast count of <5%, the absence of circulating blasts and blasts with Auer rods, the absence of an extramedullary disease, an absolute neutrophil count of ≥1.0 × 109/L, and a platelet count of ≥100 × 109/L. 13 The OS rate was defined as the time between induction therapy and the time of death or last follow-up. The EFS rate was defined as the time interval from the diagnosis to the date of primary refractory disease, molecular and hematologic relapse, or death from any cause. 13 Relapse was estimated in cases of patients who achieved CR using a cumulative incidence function with respect to the competing risks. Differentiation syndrome consisted of the presence of signs and symptoms of fever, lung infiltrates, respiratory failure, pericardial effusion, pleural effusions, weight increase caused by fluid retention, and acute renal failure. The syndrome commonly occurs within the first 2 weeks after the first induction treatment in patients with APL. 14 Cardiac events, grades 3 to 4 liver toxicity, grades 3 to 4 renal toxicity, infection, bleeding events, and thrombotic events were defined according to common terminology criteria for adverse events. 15
Quality Assessment of the Included Studies
The Jadad quality assessment scale was used to evaluate the quality of the included randomized-controlled studies. 16
Statistical Analysis
The Mantel-Haenszel method was used to pool the effect estimates and 95% confidence intervals of the included studies together. 17 Cochran Q test was calculated and the statistical heterogeneity across the included studies was estimated using the I 2 statistic. The 4 levels of heterogeneity were as follows: (1) I 2 value of 0% to 25% indicated insignificant heterogeneity; (2) I 2 value of 26% to 50% represented low heterogeneity; (3) I 2 value of 51% to 75% represented moderate heterogeneity; and (4) I 2 value of 76% to 100% represented high heterogeneity. 18 Because of the high likelihood of between-study heterogeneity, random-effects model was utilized rather than fixed-effects model. Statistical significance was defined as P values of less than .05. Funnel plot was planned to be created and used for the assessment for publication bias (if there were enough included studies). All statistical analyses were performed using Review Manager 5.3 software from the Cochrane Collaboration (London, United Kingdom).
Results
The search strategy yielded 485 potentially relevant articles (MEDLINE, 65 articles; and EMBASE, 420 articles). Initially, a total of 54 articles were excluded because of duplication. The titles and abstracts of the remaining 431 articles were reviewed which resulted in further exclusion of additional 416 articles for the following reasons: (1) ineligible article type (case report, review, meta-analysis, comments, or editorial); (2) the studies were not performed on patients with APL; (3) the studies did not compare RIF group with ATO group; and (4) the studies did not report the primary outcome of interest. The remaining 15 articles underwent a full-length review, and 11 articles were excluded because of the reasons similar to the first round. Finally, 4 randomized controlled studies met the eligibility criteria and were included in the meta-analysis. 7 -10 A flow chart of the literature review and selection process is illustrated as Figure 1.

The literature review and selection process.
Baseline Patient Characteristics
A total 482 patients with APL were included (258 received RIF and 224 received ATO). There were more males than females in both groups with the age range of 1 to 60 years. The first 2 studies included both adult and pediatric patients, 8,9 while the third one is only based on pediatric 7 and the fourth on adult patients. 10 Moreover, studies from Wang et al 9 and Zhu et al 10 were selectively conducted in “non-high risk APL” population, while the others also included “high-risk” patients. According to the Sanz risk classification, 88.8% of the patients in the RIF group and 82.6% of the patients in the ATO group had low-to-intermediate risk APL. 19 Table 1 demonstrates the baseline characteristics, study period, methodology, and quality assessment of the included studies. Table 2 describes the chemotherapy regimens utilized by those studies.
Characteristics of the Studies Included in the Meta-Analysis.

Abbreviations: ATO, arsenic trioxide; APL, acute promyelocytic leukemia; F, female; M, male; RIF, Realgar-Indigo naturalis formula; WBC, white blood cell.
Treatment Regimens Utilized by the Included Studies.

Abbreviations: AC, cytarabine; ATRA, all-trans-retinoic acid; ATO, arsenic trioxide; D, day; HCR, hematologic complete remission; HCRp, HCR with incomplete platelet recovery; IT, intrathecal injection; MA, mitoxantrone; MTX, methotrexate; RIF, Realgar-Indigo naturalis formula; 6MP, 6-mercaptopurine.
a Plus IT AC and dexamethasone D1 of each consolidation.
Treatment Response and Long
-
Term Outcomes
The chances of achieving CR were numerically higher in the RIF group but the difference was not statistically significant (pooled odds ratio [OR]: 4.59, 95% CI: 0.74-28.57, P = .10, I 2 = 0%; Figure 2A). 7,8,10 The risk of 30-day mortality after the commencement of induction therapy was also lower in the RIF group but the difference was not statistically significant (pooled OR: 0.22, 95% CI: 0.04-1.36, P = .10, I 2 = 0%; Figure 2B). 8,10 Long-term outcomes (OS, EFS, and CIR) were reported by 3 studies (although the duration of follow-up varied from 2 years to 5 years). The chance of OS was numerically higher in the RIF group than in the ATO group, although the result did not reach statistical significance (pooled OR of 5.48, 95% CI: 0.91-32.86, P = .06, I 2 = 0%; Figure 3A). 7,8,10 Similar result was observed for the chance of EFS that was numerically higher among patients who received RIF but without statistical significance (pooled OR: 2.87, 95% CI: 0.73-11.33, P = .13, I 2 = 0%; Figure 3B). 7,8,10 On the other hand, the risk of relapse (CIR) was numerically higher in the RIF group but, again, the difference was not statistically significant (pooled OR: 1.58, 95% CI: 0.20-12.44, P = .66, I 2 = 0%; Figure 3C). 8,10
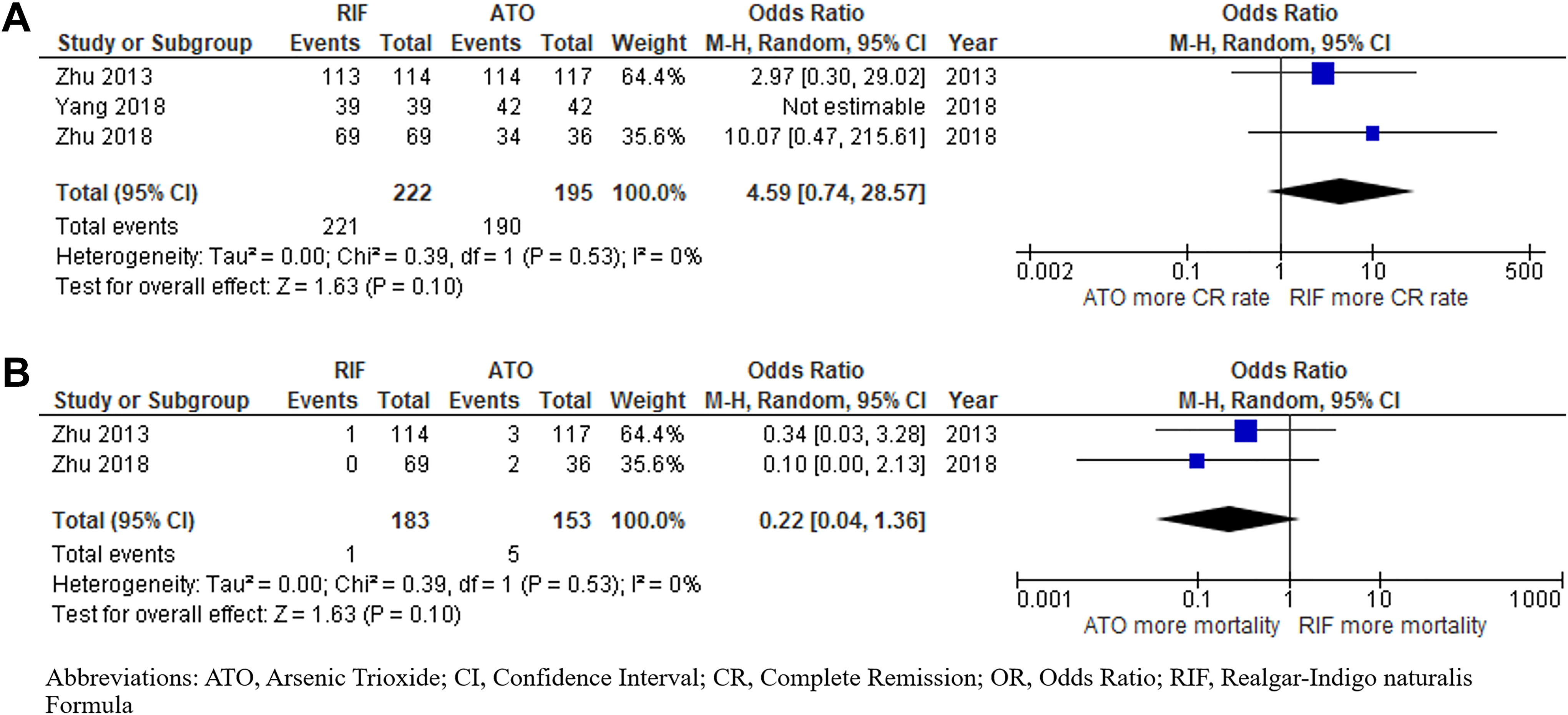
Forest plots of studies that compared the chance of (A) complete remission; and (B) 30-day mortality among patients who received RIF versus ATO. ATO indicates arsenic trioxide; RIF, Realgar-Indigo naturalis formula.

Forest plots of studies that compared the chance of (A) overall survival; (B) event-free survival; and (C) cumulative incidence of relapse among patients who received RIF versus ATO. ATO indicates arsenic trioxide; RIF, Realgar-Indigo naturalis formula.
Adverse Effects
The risk of the development of differentiation syndrome was not significantly different between the groups with the pooled OR comparing the RIF group to the ATO group of 0.65 (95% CI: 0.37-1.13, P = .13, I 2 = 0%; Figure 4). 7 -10 Only the study by Zhu et al 10 reported the median time of onset of differentiation syndrome (8 days in the RIF group and 6 days in the ATO group). Similarly, the rates of other adverse effects were not significantly different between the groups which included cardiac complication (pooled OR: 0.44, 95% CI: 0.05-3.68, P = .45, I 2 = 0%; Figure 5A), 7,10 grades 3 to 4 liver toxicity (pooled OR: 0.78, 95% CI: 0.40-1.53, P = .47, I 2 = 0%; Figure 5B), 7,8,10 grades 3 to 4 renal toxicity (pooled OR: 0.19, 95% CI: 0.02-1.73, P = .14, I 2 = 0%; Figure 5C),8,10 infections during treatment (pooled OR: 0.67, 95% CI: 0.44-1.02, P = .06, I 2 = 0%; Figure 6A),7,8,10 and bleeding (pooled OR: 1.30, 95% CI: 0.60-2.80, P = .51, I 2 = 0%; Figure 6B).7,10

Forest plots of studies that compared the risk of differentiation syndrome among patients who received RIF versus ATO. ATO indicates arsenic trioxide; RIF, Realgar-Indigo naturalis formula

Forest plots of studies that compared the risk of (A) cardiac complications; (B) grades 3 to 4 liver toxicity; and (C) grades 3 to 4 renal toxicity among patients who received RIF versus ATO. ATO indicates arsenic trioxide; RIF, Realgar-Indigo naturalis formula.

Forest plots of studies that compared the risk of (A) infections and (B) bleeding events among patients who received RIF versus ATO. ATO indicates arsenic trioxide; RIF, Realgar-Indigo naturalis formula.
Evaluation for Publication Bias
Funnel plot was planned to be used for the evaluation of publication bias. However, the plot was eventually not created because of the small number of the included studies that would critically limit the interpretability of this plot.
Discussion
This is the first systematic review and meta-analysis to summarize all available randomized controlled studies that compared the efficacy and adverse effects of ATRA plus oral RIF regimen versus ATRA plus intravenous ATO regimen for the treatment of APL. The majority of participants in those studies were patients with low-to-intermediate risk APL. The pooled analysis found that clinical outcomes, including CR, 30-day mortality, EFS, and CIR, of patients in both groups were similar, suggesting that efficacy of the 2 regimens was comparable. Similarly, the rate of complications, including differentiation syndrome, cardiac complications, grades 3 to 4 liver toxicity, grades 3 to 4 renal toxicity, and bleeding, was not different between the 2 groups. These results may suggest that ATRA plus oral RIF regimen is, at minimum, not a worse alternative to the standard ATRA plus intravenous ATO regimen for patients with non-high-risk APL. However, the former regimen is associated with a lower cost, shorter hospital stay, and higher quality of life, which could be the appealing reasons for clinicians to use this oral therapy in practice. 11,20 There is also a study suggesting the feasibility of switching ATO to RIF treatment in a second stage of induction therapy. 21 In addition, RIF is also effective as reinduction and maintenance therapy for patients with relapsed APL. 22
The main limitation of the current systematic review and meta-analysis was the limited number of included studies, and one may argue that the nonsignificant results were the function of the limited number of participants rather than the true similarity between the regimens. However, it should be noted that almost all of the results are trending in favor of the ATRA plus oral RIF regimen, including 4.6 times higher chance of achieving CR, 5.5 times higher chance of OS, 2.9 times higher chance of EFS, 35% lower chance of differentiation syndrome, 56% lower chance of cardiac complication, 22% lower chance of liver toxicity, 81% lower chance of renal toxicity, and 33% lower chance of infection. Therefore, it is unlikely that our conclusion that ATRA plus oral RIF regimen is not worse than the standard ATRA plus intravenous ATO regimen would change even if data from additional future randomized controlled studies are available. Another limitation related to the small number of included studies was the inability to perform evaluation for publication bias. Last, approximately 10% of patients included in this meta-analysis had high-risk APL. Since the primary focus of the current study was to study the utility of oral RIF among patients with non-high-risk APL, the inclusion of patients with high-risk APL may have skewed the effect estimates. Unfortunately, subgroup analyses of only patients with non-high-risk APL could not be performed because the included studies did not provide subgroup data on those outcomes of interest.
Conclusion
The current systematic review and meta-analysis study found no significant difference in clinical outcomes among patients with APL who received ATRA plus oral RIF regimen versus those who received standard ATRA plus intravenous ATO regimen. The results may suggest that ATRA plus oral RIF regimen is, at minimum, not a worse alternative.
Supplemental Material
Supplementary_data_1_APL - Efficacy and the Adverse Effects of Oral Versus Intravenous Arsenic for Acute Promyelocytic Leukemia: A Meta-Analysis of Randomized-Controlled Studies
Supplementary_data_1_APL for Efficacy and the Adverse Effects of Oral Versus Intravenous Arsenic for Acute Promyelocytic Leukemia: A Meta-Analysis of Randomized-Controlled Studies by Natthaporn Sasijareonrat, Nikolaus Jahn, Patompong Ungprasert and Weerapat Owattanapanich in Technology in Cancer Research & Treatment
Supplemental Material
Supplementary_Data_2_APL - Efficacy and the Adverse Effects of Oral Versus Intravenous Arsenic for Acute Promyelocytic Leukemia: A Meta-Analysis of Randomized-Controlled Studies
Supplementary_Data_2_APL for Efficacy and the Adverse Effects of Oral Versus Intravenous Arsenic for Acute Promyelocytic Leukemia: A Meta-Analysis of Randomized-Controlled Studies by Natthaporn Sasijareonrat, Nikolaus Jahn, Patompong Ungprasert and Weerapat Owattanapanich in Technology in Cancer Research & Treatment
Footnotes
Authors’ Note
All authors designed the study. NS and WO manually reviewed the potential articles, selected the included studies, collected the data, and drafted the manuscript. WO performed the statistical analyses. NJ and PU made critical revisions to the manuscript. N.S. and WO revised the final manuscript. All authors read and approved the final manuscript. The data sets used and/or analyzed during the current study are available from the corresponding author on reasonable request. The need for ethics approval by an institutional board review was waived as this study does not directly involve human subjects.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
Abbreviations
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.