
Abstract
Background
Several studies have shown that serum bilirubin has a protective effect against cardiovascular disease and that inflammation plays an important role in its pathogenesis. This cross-sectional study investigated whether there was an association between blood total white blood cell count, a simple indicator of inflammation, and serum total bilirubin concentration in a cohort of an adult population in Taiwan.
Methods
A total of 2458 apparently healthy adults (1246 men and 1212 women) who attended health examination at a medical centre in central Taiwan were enrolled. We collected anthropometric measurements, fasting blood test results, lifestyle habits and medical history.
Results
Total white blood cell counts decreased progressively when the concentrations of total bilirubin increased as demonstrated in the total bilirubin quartiles. Both total bilirubin concentrations and total white blood cell counts showed significant correlations with the components of metabolic syndrome, including triglyceride and high-density lipoprotein cholesterol concentrations. Multivariate linear regression analysis revealed that, for both genders, total bilirubin showed an independent negative correlation with total white blood cell count after adjusting for conventional cardiovascular risk factors.
Conclusions
Higher serum total bilirubin concentrations within the reference range were associated with lower blood total white blood cell counts, regardless of other classical cardiovascular risk factors.
Introduction
An inverse association between serum total bilirubin concentration and the risk of cardiovascular disease (CVD), such as coronary artery disease, ischemic stroke and peripheral arterial disease, has been observed in several epidemiological studies.1–5 It has been proposed that bilirubin, as an end product of haem metabolism, can prevent atherosclerosis through antioxidant activity and lipid oxidation suppression,5–9 especially of low-density lipoprotein cholesterol.7,8,10 In addition, some in vitro human studies demonstrate that bilirubin has anti-inflammatory activities that can inhibit tumour necrosis factor-α-induced upregulation of E-selectin, vascular cell adhesion molecule 1 and intercellular adhesion molecule 1.11,12 Because there is increasing evidence that atherosclerosis is accompanied by inflammation, 13 it is hypothesized that bilirubin may also exert its protective effects on CVD through inflammation reduction. An elevated blood total white blood cell (WBC) count, a simple indicator of inflammation, has been associated with an increased risk of CVD in several epidemiological studies.13–15 However, research on the relationship between serum bilirubin concentration and blood WBC count is lacking. The aim of this cross-sectional study was to evaluate whether blood total WBC count was associated with circulating total bilirubin concentration in a large adult Chinese population attending a routine health examination.
Methods
Subjects and data collection
A total of 4852 adults who attended a self-paid packaged physical check-up from August 2000 to April 2002 at a medical centre in central Taiwan were enrolled in this study. All participating subjects presented to the physical check-up centre after an overnight fast. The medical history, smoking, drinking and exercise habits of all participants were self-reported using a structured questionnaire. Smoking status was divided into never, former and current smoker. Regular exercise was defined as 30 min or more of exercise per day for at least three days a week. Habitual alcohol use was defined as drinking at least once per week. All subjects were weighed in light clothing with no shoes and their heights were also measured. Blood pressure was measured in the right arm using standard mercury sphygmomanometers on sitting position after 5 min of rest. A venous blood sample was taken in the morning after an overnight fast. Total bilirubin, plasma glucose, alanine aminotransferase (ALT), triglyceride, total cholesterol and high-density lipoprotein cholesterol (HDL-C) concentrations were measured using photometric enzymatic methods with a chemistry analyser (Hitachi 7600, Tokyo, Japan) at the central laboratory of the hospital. Creatinine was measured using Jaffe method (Hitachi 7600, Tokyo, Japan), which was calibrated from the isotope dilution mass spectrometry method. The estimated glomerular filtration rate (eGFR) was calculated by the modification of diet in renal disease study equation. 16 Total WBC count was computed using an autoanalyser (Sysmex SE-9000, Kobe, Japan). The internal quality control and external quality assessment of all laboratory methods were acceptable. This study was approved by the Institutional Review Board of Taichung Veterans General Hospital.
Because circulating total WBC count and total bilirubin concentration are influenced by several medical disorders, the subjects with the following criteria were excluded: (1) age less than 18 years (n = 8); (2) total WBC counts more than 15 × 109/L or less than 3 × 109/L (to rule out a possible bone marrow disorder, active infection or inflammation) (n = 25); (3) serum ALT concentration more than 40 U/L (n = 766; reference interval: 4–40 U/L); (4) total bilirubin concentration more than 20.52 µmol/L (n = 431; reference interval: 3.42–20.52 µmol/L); (5) chronic hepatitis B infection (n = 619) (defined as hepatitis B virus surface antigen positive); (6) excessive alcohol consumption (n = 203) (defined as more than 14 drinks or 210 g per week in men and more than seven drinks or 105 g per week in women); (7) albumin less than 35 g/L (n = 16; reference interval: 35–50 g/L); (8) alkaline phosphatase more than 190 U/L (n = 80; reference interval: 50–190 U/L); (9) lactate dehydrogenase more than 240 U/L (n = 283; reference interval: 120–240 U/L); (10) eGFR less than 30 mL/min/1.73 m2 (n = 22); (11) using medication for pain relief or hyperuricemia (n = 199) and (12) did not fill out the questionnaire (n = 697). After controlling for exclusion criteria, a total of 2458 subjects (1246 men and 1212 women with a mean age of 51 ± 12 years) were finally analysed.
Statistical analysis
Body mass index (BMI, weight in kilograms/height 2 in metres) was calculated by dividing body-weight by the square of height. Continuous variables measured in this study were expressed as mean values ± standard deviation for normally distributed data and as median (25th–75th percentile) for skewed data (including fasting glucose and triglyceride). Because serum total bilirubin concentration differs significantly by gender, total bilirubin concentrations were divided into quartiles arbitrarily (0<Q1≤8.55, 8.55<Q2≤11.97, 11.97<Q3≤15.39 and 15.39<Q4≤20.52 µmol/L for men; 0<Q1≤6.84, 6.84<Q2≤10.26, 10.26<Q3≤13.68 and 13.68<Q4≤20.52 µmol/L for women) to examine the difference in WBC count and the other clinical variables by using p for trend. The χ2 test for linear trend was used for categorical risk factors. One-way analysis of variance and Kruskal–Wallis test were used to assess the trend for continuous risk factors. Correlations between total WBC count and the components of metabolic syndrome were assessed using Pearson or Spearman tests. In addition, multiple linear regression analyses were performed to assess the independent relationship between circulating total WBC count and total bilirubin concentration with adjustment for possible confounding factors, including age, biochemical and anthropometric variables, smoking, drinking and exercise habits. All statistical analyses were performed with the Statistical Package for the Social Sciences statistical software package for Windows, version 12.0 (SPSS Inc., Chicago, IL, USA), and a two-tailed p value of < 0.05 was considered statistically significant.
Results
Clinical characteristics of study subjects.
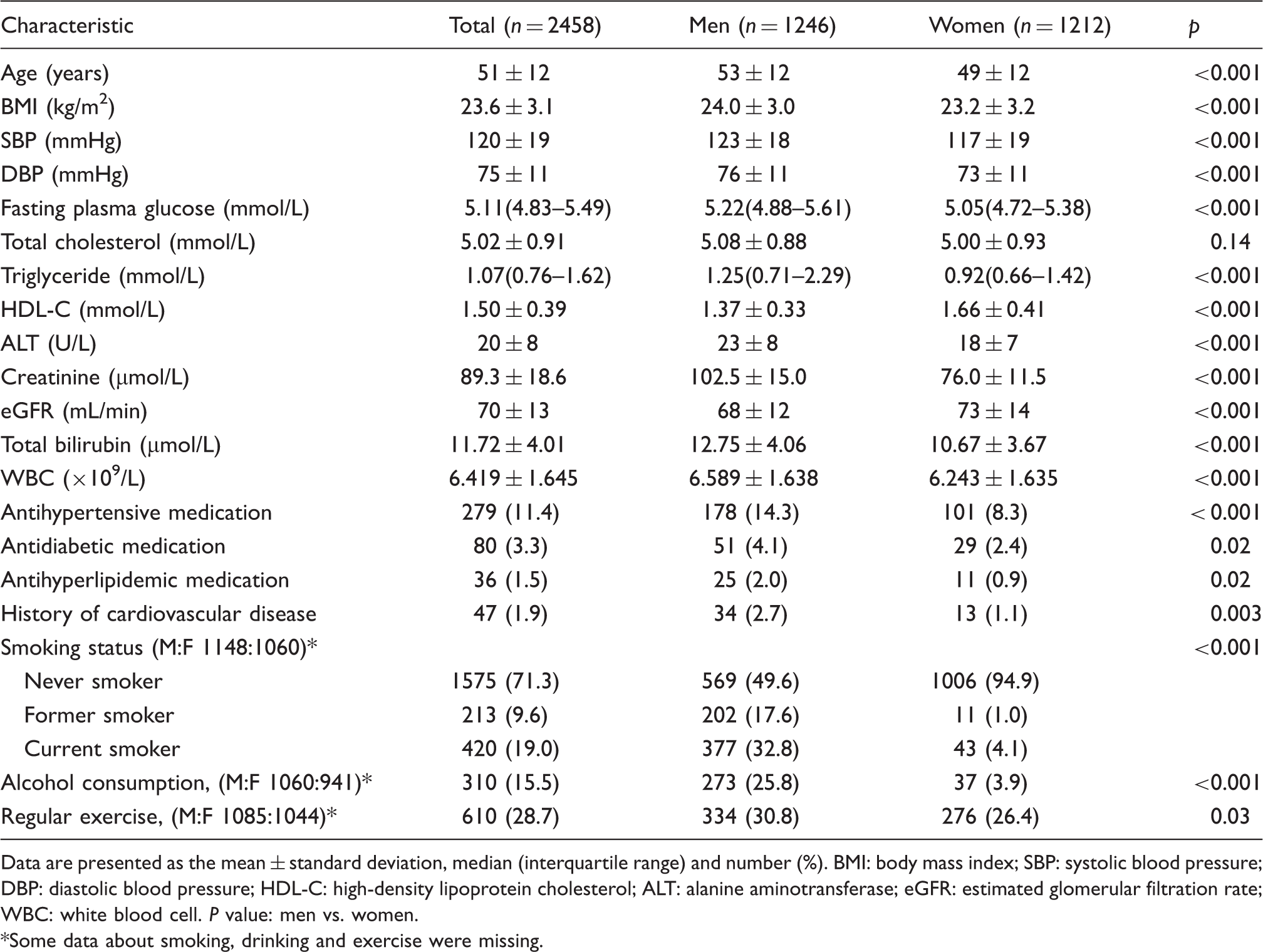
Data are presented as the mean ± standard deviation, median (interquartile range) and number (%). BMI: body mass index; SBP: systolic blood pressure; DBP: diastolic blood pressure; HDL-C: high-density lipoprotein cholesterol; ALT: alanine aminotransferase; eGFR: estimated glomerular filtration rate; WBC: white blood cell. P value: men vs. women.
Some data about smoking, drinking and exercise were missing.
Characteristics according to the quartiles of total bilirubin in men.
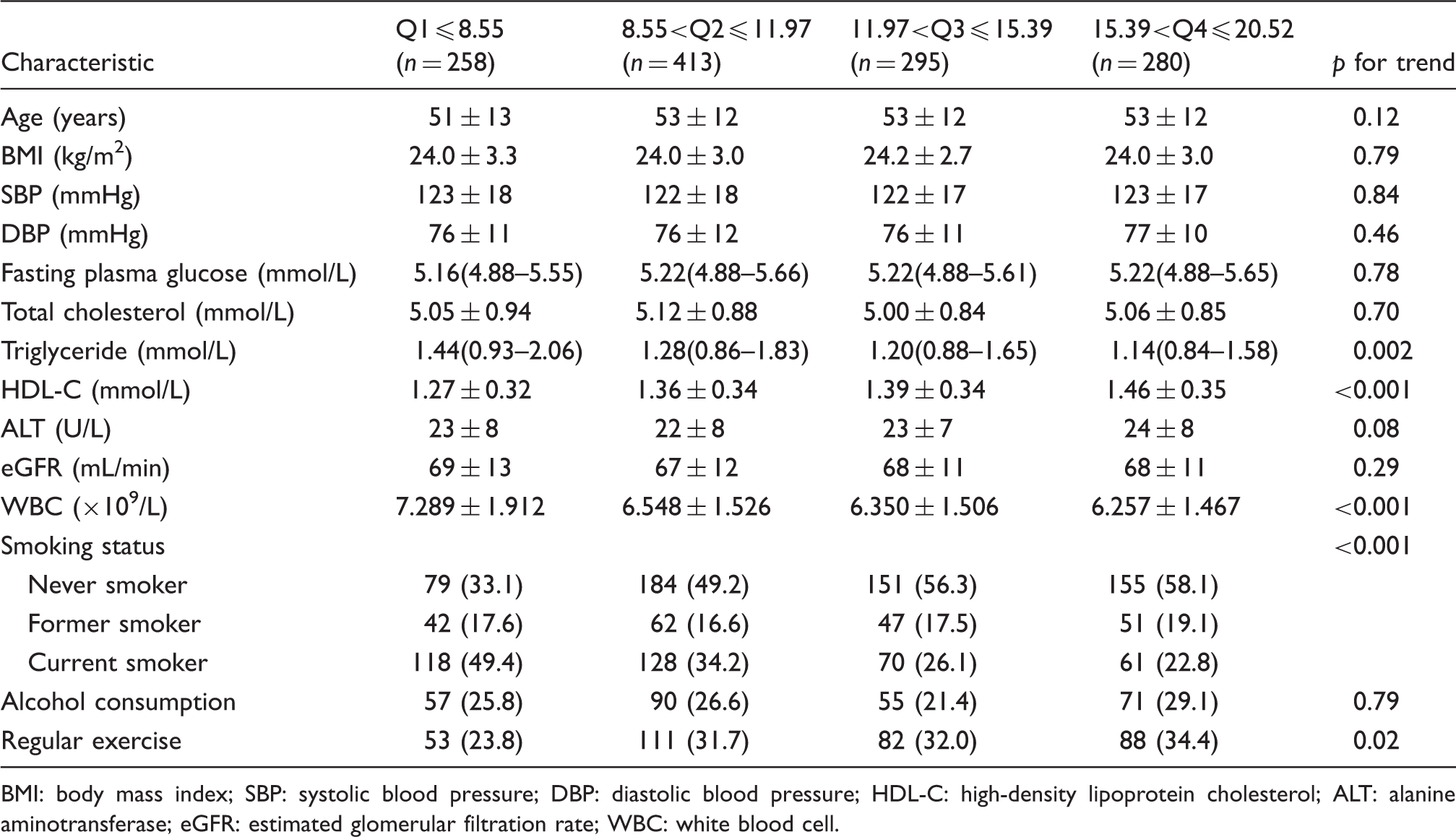
BMI: body mass index; SBP: systolic blood pressure; DBP: diastolic blood pressure; HDL-C: high-density lipoprotein cholesterol; ALT: alanine aminotransferase; eGFR: estimated glomerular filtration rate; WBC: white blood cell.
Characteristics according to the quartiles of total bilirubin in women.
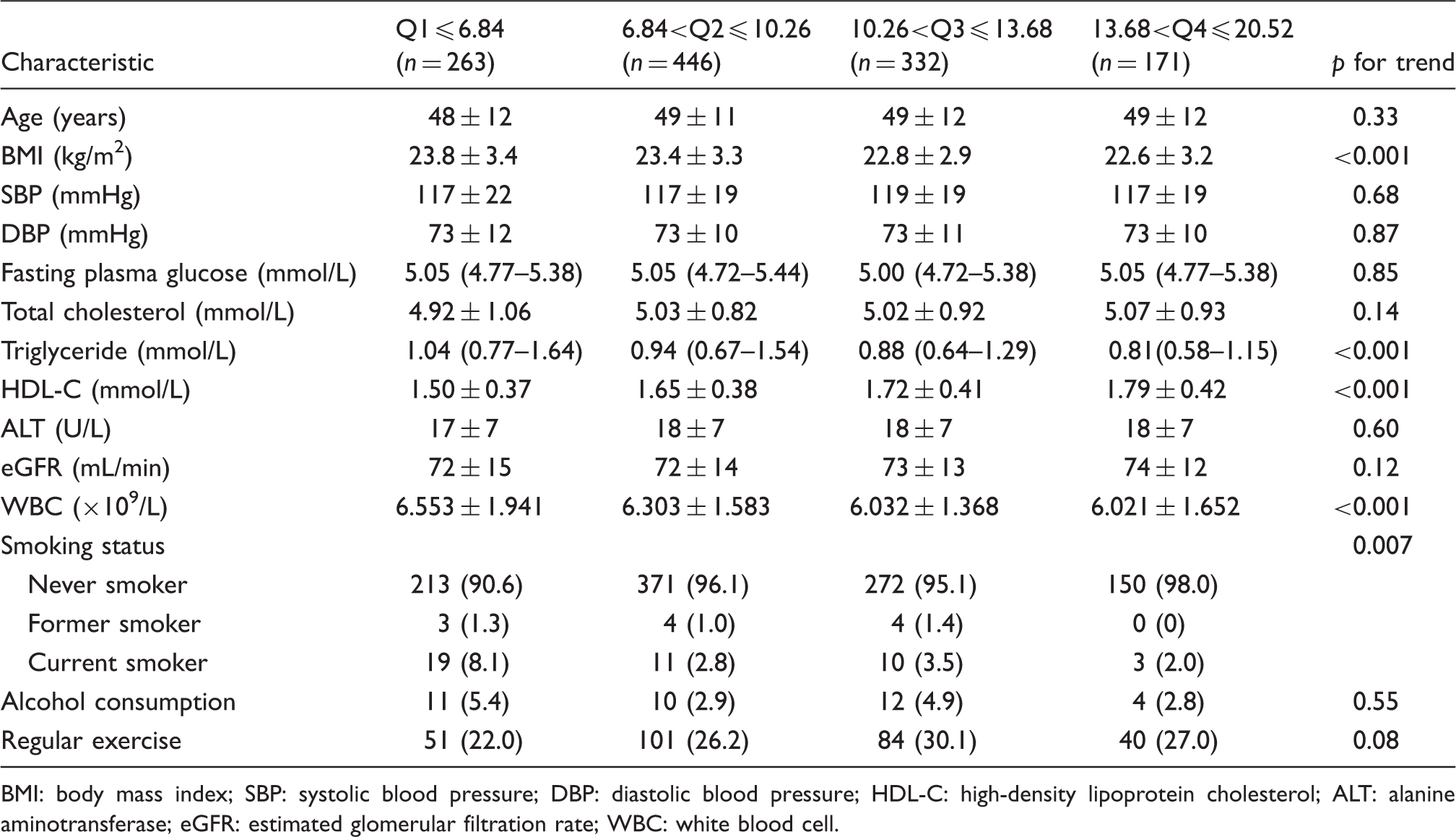
BMI: body mass index; SBP: systolic blood pressure; DBP: diastolic blood pressure; HDL-C: high-density lipoprotein cholesterol; ALT: alanine aminotransferase; eGFR: estimated glomerular filtration rate; WBC: white blood cell.
Multiple linear regression using total WBC count (×109/L) as the dependent variable.
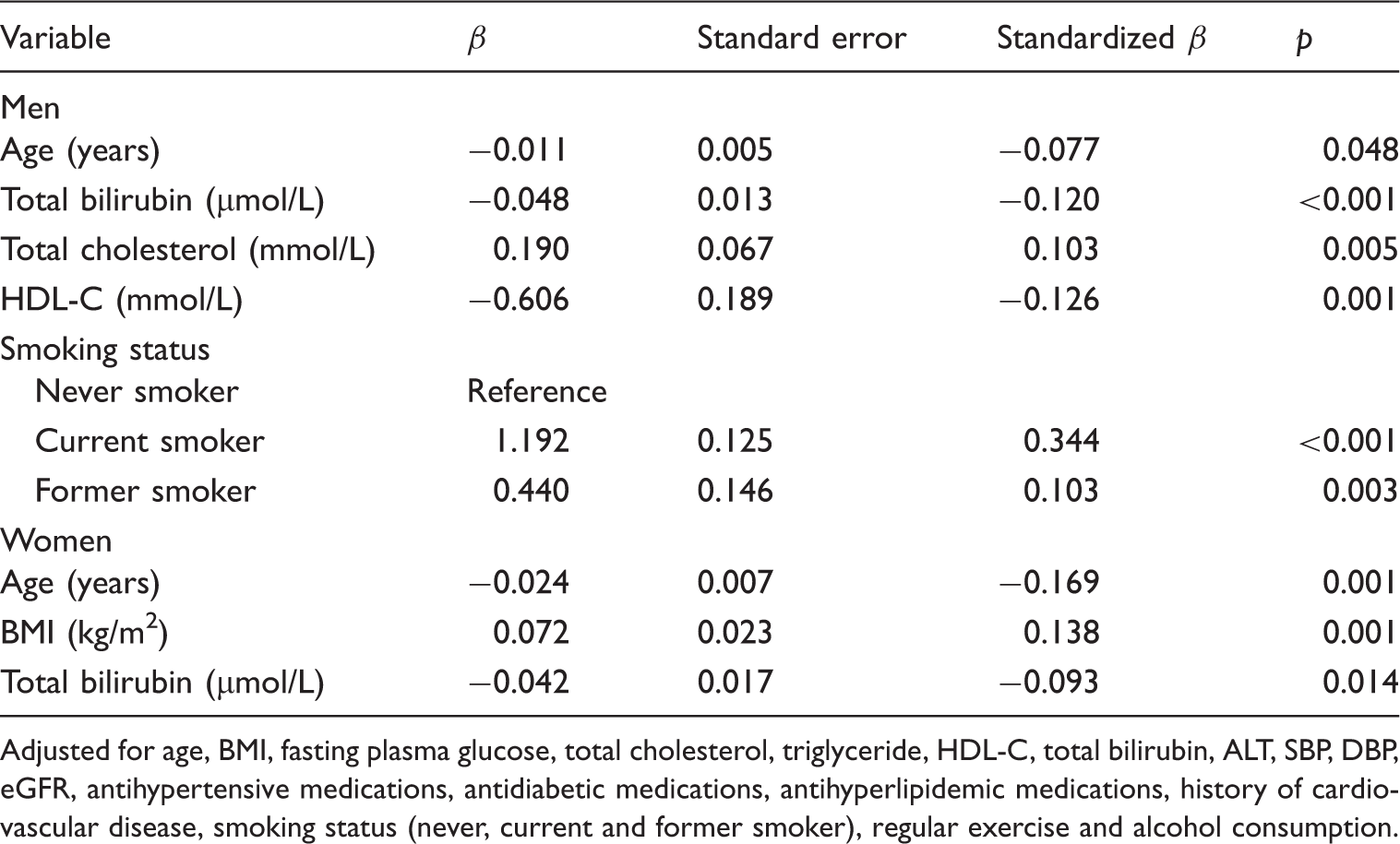
Adjusted for age, BMI, fasting plasma glucose, total cholesterol, triglyceride, HDL-C, total bilirubin, ALT, SBP, DBP, eGFR, antihypertensive medications, antidiabetic medications, antihyperlipidemic medications, history of cardiovascular disease, smoking status (never, current and former smoker), regular exercise and alcohol consumption.
In male subjects, we found that current smokers and former smokers had higher total WBC counts than never smokers after controlling for aforementioned confounders (Table 4).
Discussion
This cross-sectional study in a cohort of a Chinese population demonstrated that the serum total bilirubin concentration within the reference range correlated negatively with blood total WBC count, triglyceride concentration, and smoking and correlated positively with HDL-C concentration in both men and women. After controlling for age, BMI, lipids, glucose, lipid lowering medications, antihypertensive and antidiabetic agents, blood pressure, ALT, eGFR, previous CVD and lifestyle habits such as smoking, drinking and physical activity, the association between blood total WBC count and serum total bilirubin concentration remained valid.
The possible mechanisms for the association between serum total bilirubin and blood total WBC count may be multiple and protean. First, in vitro human and animal studies have reported an inverse relationship between circulating total bilirubin and several inflammatory markers, such as lipopolysaccharide-induced interleukin-1β, C-reactive protein, soluble CD40 ligand and P-selectin concentrations, all of which may be involved in the regulation of inflammation and/or WBC production.17–20 Our findings were consistent with these studies, suggesting an anti-inflammatory activity of bilirubin. Increased total bilirubin concentrations might also reflect the enhanced activity of haem oxygenase, an enzyme that catalyses haem degradation with several enzymatic byproducts released, including carbon monoxide, ferrous iron and biliverdin/bilirubin, all of which have established antioxidant and anti-inflammatory properties 21 ; therefore, higher total bilirubin concentrations potentially reduced haem-induced cell injury. Second, the decreased serum total bilirubin concentrations could be an effect of an elevated blood total WBC count, which enhances cellular oxidative stresses that can lead to the consumption of natural antioxidants. 22 Third, the association between serum total bilirubin concentration and blood total WBC count might be explained by an indirect linking factor. Serum total bilirubin concentrations have been reported in epidemiologic surveys to be negatively correlated with several cardiovascular risk factors, including obesity, blood glucose and lipid concentrations and blood pressure.18,23–25 It has been proposed that the inverse relationship between serum total bilirubin and metabolic syndrome features is due to the regulatory effects of bilirubin upon insulin resistance, a core defect in the pathogenesis of metabolic syndrome. 18 In vivo animal studies displayed that bilirubin could increase the expression of adiponectin, an adipocytokine with properties that improve insulin sensitivity26,27; however, it is also known that individuals with an elevated blood total WBC count have an increased risk of developing metabolic syndrome because chronic inflammation can induce insulin resistance.28–31 Therefore, metabolic syndrome and/or insulin resistance could underlie the observed association between serum total bilirubin and blood total WBC.
Several epidemiologic studies have reported that people with Gilbert’s syndrome, subjects with high normal or just above normal serum total bilirubin concentrations have a lower risk of coronary artery disease and carotid plaque formation.9,19 Accordingly, it may be beneficial to increase circulating total bilirubin concentration through pharmacologic or non-pharmacologic interventions to attain a protective effect on cardio- or cerebral vascular disease. 3 In contrast, if low serum total bilirubin concentration was coincidentally associated with elevated blood total WBC count and the other established cardiovascular risk factors, such as hyperglycaemia, dyslipidemia, hypertension and obesity, the circulating total bilirubin would be merely a marker of CVDs and therapeutic targeting at bilirubin would be fruitless.
In line with previous studies,32–34 our study showed that smoking is associated with decreased serum total bilirubin concentration and increased blood total WBC count. Possible mechanisms include bilirubin overconsumption by free radical species related to cigarette smoking 35 and upregulation of enzymes involved in bilirubin metabolism. 36 Therefore, smoking may increase CVD risk by lowering serum total bilirubin concentrations and increasing inflammation. 2 However, the association between blood total WBC count and smoking status was not observed in women, probably due to too low prevalence of smokers in the female subjects to detect a true association.
Our study had several limitations. First, the cross-sectional nature of this study did not allow for the determination of the temporal association of bilirubin with WBC or allow conclusions regarding causation. Second, there was no measurement of C-reactive protein or other specific markers of inflammation; however, given the close association between C-reactive protein and the blood total WBC count, we measured the WBC count rather than other inflammatory markers because it is one of the most common laboratory tests. Third, serum bilirubin concentrations and blood WBC counts were measured only once and serum bilirubin might exhibit significant within-subject variation. 37 However, all subjects were examined in the morning after an overnight fast (≥8 h). In addition, we excluded those subjects with potential hepatobiliary diseases and illness associated with haematological abnormalities to minimize these possible confounders. Fourth, serum total bilirubin concentration may be influenced by hereditary factors, 38 food intake habits, 39 which were not examined in this study. Finally, our subjects consisted of participants who attended a self-paid packaged physical check-up at our hospital; although large in number, this sample might differ from the general population regarding socioeconomic factors, race and culture.
In conclusion, our study found that increased serum total bilirubin concentrations within the reference range were associated with lower blood total WBC counts in both men and women in Taiwan. The results suggested that the subjects with increased circulating total bilirubin concentrations have a lower risk of inflammation, although the exact causal relationship of this association still requires further investigation.
Footnotes
Declaration of conflicting interests
None declared.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Ethical approval
The Institutional Review Board of Taichung Veterans General Hospital approved this study (protocol no: CE11028).
Guarantor
WDC.
Contributorship
WDC and YYW – conception, design, sample collection and assembly of data. WNT, WDC, SYL and WHS – analysis and interpretation of the data. WNT – the first draft of the manuscript. JTL – the accuracy of the laboratory methods. All authors reviewed and edited the manuscript and approved the final version of the manuscript.
Acknowledgements
We would like to thank Dr. Chia-Lin Lee and Biostatistics Task Force of Taichung Veterans General Hospital for statistical support.