
Abstract
Background
Inflammation is involved in the pathogenesis of preeclampsia. Omentin is a newly discovered adipokine that possesses an anti-inflammatory function. The aim of this study was to determine the association of serum omentin-1 concentration with the presence and severity of preeclampsia.
Methods
Serum concentrations of omentin-1 were measured in 128 women with preeclampsia and 96 women with uncomplicated pregnancies using an enzyme-linked immunosorbent assay method.
Results
Patients with preeclampsia had significantly lower serum concentrations of omentin-1 compared to healthy controls. In addition, those patients with severe preeclampsia had significantly lower concentrations of serum omentin-1 compared to those with mild preeclampsia. Simple linear regression analysis showed that in patients with preeclampsia the serum concentrations of omentin-1 showed significant correlation with body mass index (P < 0.001), systolic blood pressure (P < 0.05) and homeostasis model assessment of insulin resistance (P < 0.001).
Conclusion
Decreased concentrations of serum omentin-1 appear to be associated with the presence and severity of preeclampsia.
Introduction
Preeclampsia, which is characterized by new-onset hypertension and proteinuria, is one of the most serious complications of pregnancy. Its prevalence ranges from 3% to 8% of pregnancies and it affects a total of 8.5 million women worldwide. 1 It is the most common cause of maternal and fetal morbidity and mortality. It is the cause of nearly 40% of all births that are delivered before 35 weeks of gestation and is also associated with an increased risk in later-life of death from cardiovascular disease. 2 Several maternal clinical characteristics, including ethnicity, age, parity, multiple pregnancy and a history of preeclampsia in earlier pregnancies, obesity and systematic inflammation status, have all been identified as risk factors for developing preeclampsia. 3
Omentin, a novel adipokine, is secreted mainly by visceral adipose tissue. It is coded by two genes, namely, omentin-1 and omentin-2, and the former gives rise to the major circulating form. 4 Serum omentin-1 concentrations have been shown to be significantly decreased in obese patients, indicating a possible role of omentin-1 in obesity. 5 Recent studies have shown that omentin exerts an anti-inflammatory function by preventing tumor necrosis factor-α (TNF-α)-induced COX-2 expression in vascular endothelial cells. 6 Inflammation plays a key role in the mechanism of preeclampsia. 7 Therefore, it is possible that omentin-1 might be involved in the pathophysiology of preeclampsia.
To our knowledge, few reports have been published on the role of omentin-1 in the pathogenesis of preeclampsia. The aim of the present study was to ascertain whether there is any association between serum omentin-1 concentration and the presence and severity of preeclampsia.
Materials and methods
Patients
A total of 128 women diagnosed with preeclampsia were enrolled in this study. Preeclampsia was defined as maternal systolic blood pressure (SBP) ≥140 mmHg and/or diastolic blood pressure (DBP) ≥90 mmHg measured on two occasions separated by at least 6 h, and proteinuria >300 mg in a 24-h period or qualitative (>1+), after 20 weeks of gestation following the guidelines of the American College of Obstetricians and Gynaecologists. 8 Severe preeclampsia was defined as maternal SBP ≥160 mmHg and/or DBP ≥110 mmHg. Patients were excluded if they had multiple gestation, confirmed diabetes mellitus, chronic hypertension, underlying neoplasm, connective tissue disease, inflammatory or infective disorders, infectious diseases recognized in pregnancy and heart failure. The control group consisted of 96 pregnant women without preeclampsia, matched according to age, body mass index (BMI) and gestational age. The controls had no clinical evidence of gestational or fetal complications during their pregnancies and underwent routine perinatal medical care.
This study was planned according to the ethical guidelines of the Helsinki Declaration and was approved by the Institutional Research Ethics Board of our hospital. All patients provided written informed consent before participating in this study.
Measurements
Various anthropometric (height, weight and blood pressure) investigations together with laboratory analyses were performed. Venous blood was collected after a minimum of a 10-h overnight fast. Serum triglycerides (TG), serum total cholesterol (TC), high-density lipoprotein cholesterol (HDL-C) and low-density lipoprotein cholesterol (LDL-C) were measured using standard biochemical methods. Serum omentin-1 concentration was measured using an enzyme-linked immunosorbent assay (Cusabio Biotech Corporation, USA). Intra and between-assay imprecision (% coefficient of variation (%CV)) were <8% and <10%, respectively. The analytical range was 1.56–100 pg/mL and the sensitivity: 0.39 pg/mL. Homeostasis model assessment of insulin resistance (HOMA-IR) was calculated as insulin reading (µIU/mL) multiplied by plasma glucose concentration (mmol/L) and divided by 22.5. 9
Statistical analysis
Statistical analysis was carried out using SPSS version 13.0 software program (SPSS Inc, Chicago, Illinois). The results were expressed as means ± SEM or median (interquartile range). Data normality was analysed using the Kolmogorov–Smirnov test. The characteristics of the preeclampsia group and the healthy controls were compared using an unpaired t-test or Mann-Whitney U test. Differences between serum omentin-1 concentrations in patients with mild and severe preeclampsia were compared using the Mann-Whitney U test. The correlation between serum omentin-1 concentration and other parameters was analysed using simple linear regression analysis. Multiple stepwise linear regression analysis was then used to determine if there was any association of various factors with serum omentin-1 concentration. P values less than 0.05 were considered to be statistically significant.
Results
Baseline clinical characteristics
Clinical and biochemical characteristics of patients with preeclampsia and controls.
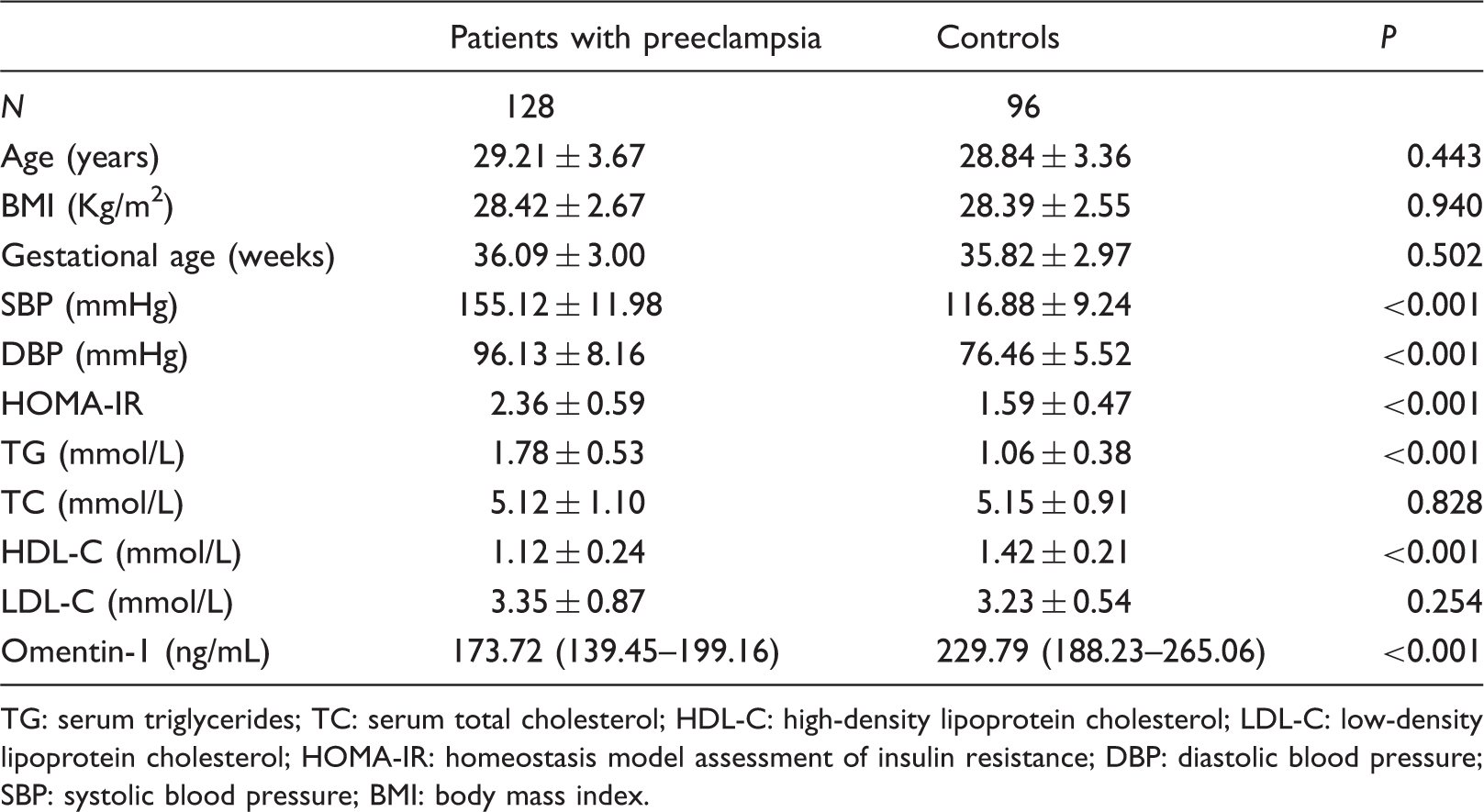
TG: serum triglycerides; TC: serum total cholesterol; HDL-C: high-density lipoprotein cholesterol; LDL-C: low-density lipoprotein cholesterol; HOMA-IR: homeostasis model assessment of insulin resistance; DBP: diastolic blood pressure; SBP: systolic blood pressure; BMI: body mass index.
Concentrations of serum omentin-1 in patients with preeclampsia
Serum concentrations of omentin-1 in patients with preeclampsia and healthy pregnant controls are shown in Figure 1. The patients with preeclampsia had significantly lower serum omentin-1 concentrations than the controls (P < 0.001). In addition, patients with severe preeclampsia had significantly lower serum omentin-1 concentrations compared to those with mild preeclampsia (P < 0.001). There was no significant difference in BMI in those patients with mild preeclampsia, compared with those with severe (28.49 ± 2.76 vs. 28.29 ± 2.52 kg/m2, P = 0.691).
Box and whisker plots showing serum concentrations of omentin-1 in healthy controls and patients with preeclampsia. *P < 0.001, versus serum omentin-1 concentrations in healthy controls; #P < 0.001, versus serum omentin-1 concentrations in patients with mild preeclampsia.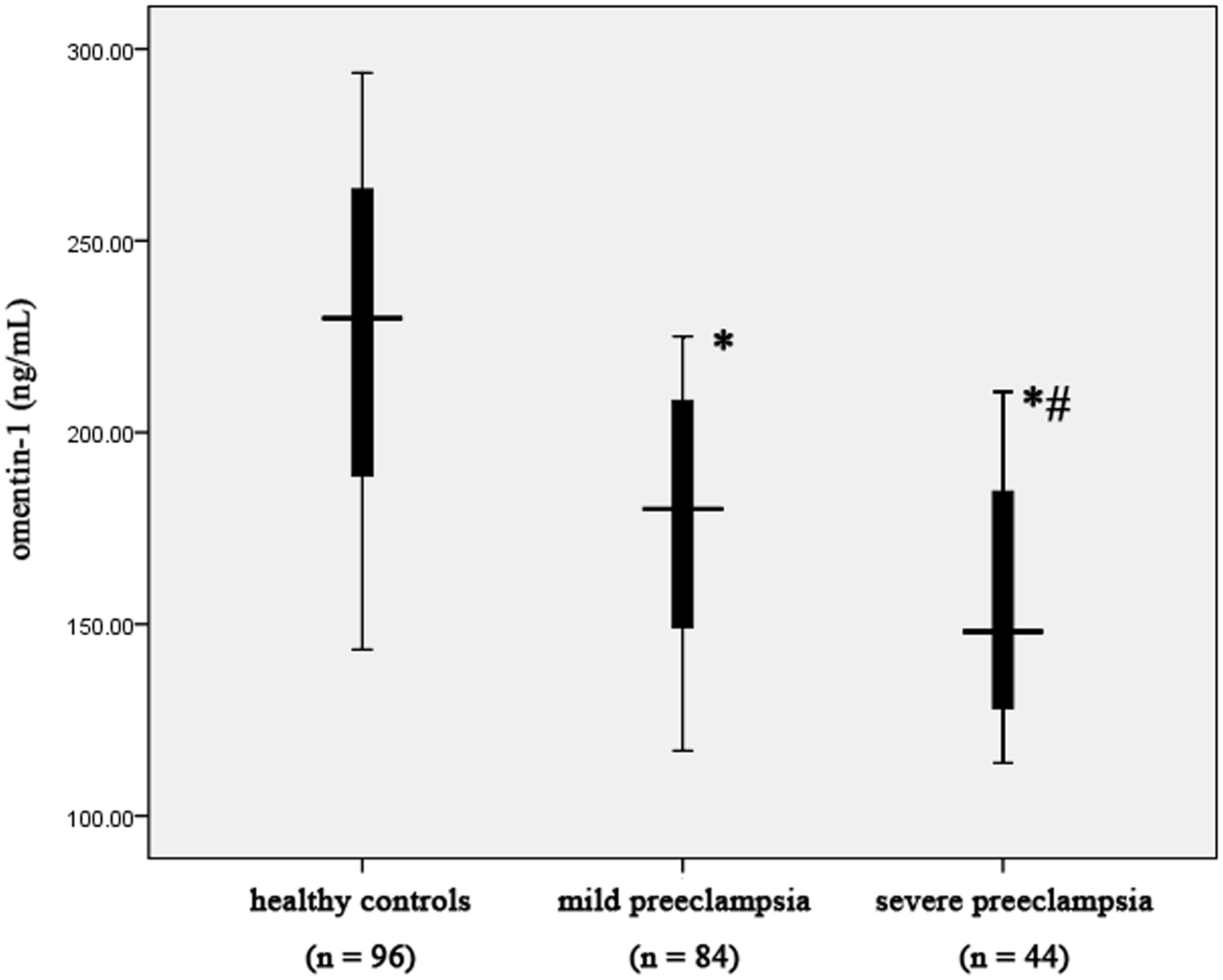
Association of serum omentin-1 concentrations with other clinical characteristics
Linear regression analyses between serum omentin-1 and other clinical parameters.
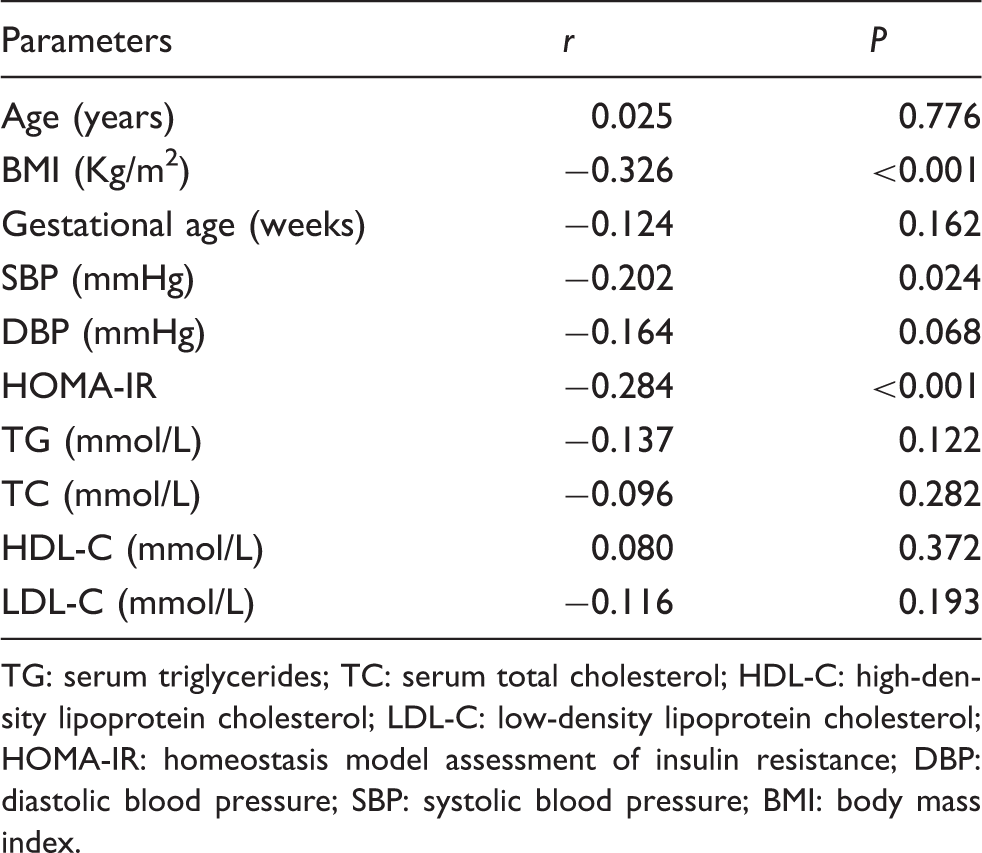
TG: serum triglycerides; TC: serum total cholesterol; HDL-C: high-density lipoprotein cholesterol; LDL-C: low-density lipoprotein cholesterol; HOMA-IR: homeostasis model assessment of insulin resistance; DBP: diastolic blood pressure; SBP: systolic blood pressure; BMI: body mass index.
Discussion
In the present study, we found that patients with preeclampsia had significantly lower serum omentin-1 concentrations compared to controls. Also, serum concentrations of omentin-1 were significantly lower in those patients with severe preeclampsia compared to those with mild preeclampsia. In addition, serum omentin-1 concentrations showed a negative correlation with BMI, SBP and HOMA-IR. To our knowledge, this is the first study to demonstrate the association of serum omentin-1 concentration with the presence and severity of preeclampsia.
Because preeclampsia is associated with significant cardiovascular morbidity and mortality, there is a need to identify those pregnancies that are at risk of preeclampsia at an early stage of pregnancy, so that preventative treatment may be started early. The use of biomarkers in early diagnosis of disease and in monitoring of treatment is well established for many disease processes. Recent studies have suggested that adipokines may have a role in the pathogenesis of preeclampsia. Adipokines are cell signalling proteins produced by adipocytes in adipose tissue, which influence glucose and lipid metabolism. They include TNF-α, interleukin-6 (IL-6), leptin, resistin, visfatin and chemerin. 10 They play important roles in the development of obesity, metabolic syndrome, diabetes and cardiovascular disease. 11 Studies on preeclampsia have shown that serum concentrations of IL-6, 12 leptin, 13 visfatin, 14 adiponectin 13 and chemerin 15 are associated with the presence of preeclampsia. The results of the present study have shown that patients with preeclampsia had significantly lower serum omentin-1 concentrations compared to healthy pregnant controls, suggesting a potential role of omentin-1 in the pathophysiology of preeclampsia. Moreover, serum omentin-1 concentrations were significantly lower in patients with severe preeclampsia compared to those with mild preeclampsia. Also, our study showed that serum omentin-1 concentration correlated with the severity of preeclampsia. Taken together, these findings suggest that serum omentin-1 concentrations may act as an independent biomarker for the presence and severity of preeclampsia.
The imbalance between angiogenic and antiangiogenic factors in the pathogenesis of preeclampsia has attracted considerable attention in the past decade. 16 A variety of angiogenic factors are produced from the human placenta. The most important one is vascular endothelial growth factor (VEGF). Omentin-1 may significantly decrease VEGF-induced endothelial cell migration and angiogenesis in human microvascular endothelial cells. 17 This finding suggests that omentin-1 may serve as antiangiogenic regulator and be involved in the pathogenesis of preeclampsia through possible antiangiogenic effects.
Omentin has been shown to act as an anti-inflammatory mediator and in one study has been shown to inhibit TNF-induced vascular inflammation in human endothelial cells. 6 In another report, omentin also inhibited TNF-α-induced vascular cell adhesion molecule-1 expression by preventing the activation of p38 and JNK at least in part through the inhibition of superoxide production. 18 In addition, serum omentin-1 concentrations have been shown to be negatively correlated with concentrations of inflammatory molecules including TNF-α, IL-6 and C-reactive protein.19,20 Taken together, these results suggest that omentin may play a role in the process of anti-inflammation. Given that inflammation may have a potential role in preeclampsia, omentin-1 may be therefore involved in the development of preeclampsia via the inhibitory function of the inflammatory pathway.
In previous studies, serum omentin concentrations have been shown to have a negative association with BMI, SBP and HOMA-IR.19,21 These findings were confirmed in the present study. Obesity, insulin resistance and hypertension are multiple compounding factors of the metabolic syndrome. Therefore, it is possible that omentin-1 may be involved in the development of the metabolic syndrome. The metabolic syndrome is closely associated with preeclampsia. 22 Given that obesity and particularly central adiposity are potent risk factors for preeclampsia, it is therefore possible that omentin-1 may have some involvement in the relationship of the metabolic syndrome and preeclampsia.
In conclusion, we acknowledge the limitations of the present case–control study, in particular, the small sample size. However, despite this, we have shown that (1) circulating concentrations of omentin-1 are significantly lower in patients with preeclampsia compared to controls, and (2) circulating concentrations of omentin-1 are significantly lower in patients with severe preeclampsia compared to those with mild. We therefore believe that a prospective cohort study should be undertaken, involving a larger population than the present study. Such a study may be more informative and reveal the true extent of association between serum concentrations of omentin-1 and preeclampsia.
Footnotes
Declaration of conflicting interests
None declared.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Ethical approval
The ethics committee of Jinan Military General Hospital (2013JMGH028).
Guarantor
TH.
Contributorship
HL, JW and TH researched literature and conceived the study. LS, YL and NT were involved in protocol development, gaining ethical approval, patient recruitment and data analysis. HL and HW wrote the first draft of the manuscript. All authors reviewed and edited the manuscript and approved the final version of the manuscript.