
Abstract
Diabetic ketoacidosis (DKA) is the hallmark of absolute insulin deficiency, occurring predominantly in people with type 1 diabetes. It is a major cause of diabetes-related morbidity. Glucose is unable to enter cells on account of the lack of insulin, with consequent hyperglycaemia. At the same time, there is an increase in lipolysis (release of free fatty acids from adipose tissue), another process controlled by insulin. The free fatty acids are converted into ketone bodies – mainly acetoacetate and β-hydroxybutyrate – to form alternative energy substrates. 1
For many years, there was no formal way to diagnose DKA other than by measuring blood glucose concentrations and dipping the urine to check for the presence of ketones. In addition, the presence of a metabolic acidosis could be confirmed, either by means of arterial blood gas analysis, or measurement of bicarbonate on venous plasma or serum. β-hydroxybutyrate is the predominant ketone in DKA and is the major contributor to the acidosis. However, the urine ketone stick test (Ketostix®, Bayer Diabetes, Berkshire, UK) uses a nitroprusside reaction and gives a semi-quantitative measure of acetoacetate, but not β-hydroxybutyrate. This is important because β-hydroxybutyrate is the predominant ketone in DKA and the major contributor to the acidosis. In addition, β-hydroxybutyrate is oxidized to acetoacetate as the ketosis resolves. Thus, if urinary urine ketone stick tests alone are used to guide treatment, a false impression may be gained that the ketoacidosis is not resolving. 2 A further limitation of urine ketone measurement is that it measures the average concentration in the urine held in the bladder since the last void. Patients with DKA are usually dehydrated on admission, and may not urinate spontaneously for several hours (some may require catheterization). This may lead to further difficulties evaluating the current biochemical state of the patient.
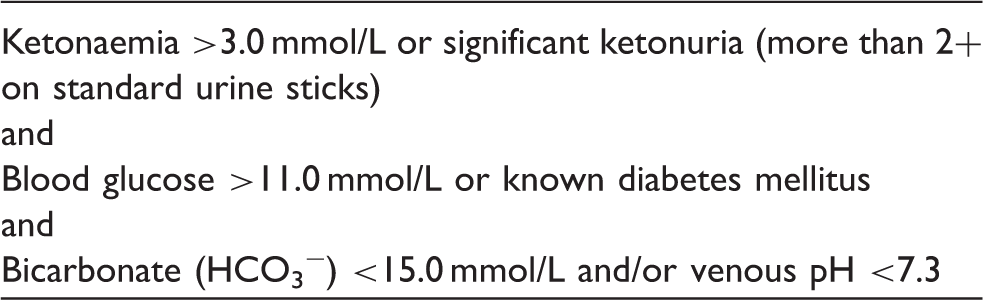
The diagnostic criteria for diabetic ketoacidosis advocated by the Joint British Diabetes Society Inpatient Care Group.
In the UK, two point-of-care testing (POCT) meters are widely used to measure blood ketone concentrations: the GlucoMen LX Plus (A Menarini Diagnostics, Wokingham, Berkshire, UK) and the Freestyle Optium Neo (Abbott Diabetes Care, Maidenhead, Berkshire, UK). The GlucoMen LX Plus clearly states in its product insert that the GlucoMen LX ß-Ketone sensors ‘should not be used to diagnose diabetes, DKA or to test new-born babies’. 7 However, elsewhere, under prevention and detection of DKA, measurement of capillary ketones is advocated if the blood glucose concentration is raised. Indeed, the meter automatically prompts ketone measurement if the glucose concentration is >13.9 mmol/L. (It also suggests that if the ketone concentration is >1.5 mmol/L, the patients’ health care team should be contacted immediately.) Thus there is an apparent contradiction: the ketone sensor should not be used to diagnose DKA, but should be used to detect if someone is at risk of developing it (on account of hyperglycaemia).
Data presented at the 2013 Diabetes UK Annual Professional Conference showed that the JBDS guideline had been adopted or adapted by over 85% of all UK hospitals, indicating widespread support for its use. 8 However, there has been criticism by some about the recommendation to measure blood ketones at the point of care rather than in the laboratory. This criticism is based in part on potentially poor performance of point-of-care equipment at high ketone concentrations, with some data showing that there is not a ‘straight line relationship’ between blood and plasma ketone concentrations. On the basis of these findings, the authors recommended that the Abbott Precision Xceed Pro ketone meter should not be used to guide treatment when the ketone concentrations exceeded 5 mmol/L. 9 Data for the GlucoMen LX Plus meter show that at a ketone concentration of 0.2 mmol/L, SD is 0.02 and coefficient of variation (CV) 10.1%, and that at a ketone concentration of 7.71 mmol/L, SD is 0.228 and CV 3% (data on file from A Menarini Diagnostics Ltd). Similarly, for the Abbott ketone meter, at a β-hydroxybutyrate concentration of 0.34 mmol/L, SD is given as 0.03 (no CV data supplied); at the highest quoted concentration (6.32 mmol/L) no SD is given (CV 3.1%) (data on file, Abbot Laboratories Ltd).
In a diabetic patient who is hyperglycaemic and acidotic, any ketone value of >3 mmol/L is enough to give a diagnosis of DKA. In addition, whilst clinical decisions are based in part on the rate of decline of ketones, this alone is rarely – if ever – used in isolation: other factors, such as the rate of decline in glucose, or the change in pH, are also used to guide management decisions. (In a similar way, for many years arterial blood gases were seen as the best way to determine acid-base status, but venous gases are now widely used because the difference between the two sites is not large enough to affect clinical decisions. 10 ) It is only when ketone concentrations drop to 0.5 mmol/L or less, i.e. well within the acceptable range of the meter use, that the management of DKA (specifically, changing from a fixed rate intravenous insulin infusion to a variable rate 4 ) may depend on ketone measurement. It is clearly essential that clinicians using POCT equipment are aware of the inherent dangers of relying on a single measurement to guide treatment in a life-threatening condition. In addition, staff must be trained in the use of blood glucose and ketone meters in line with local POCT policy and demonstrate continuing competency in their use. Finally, initial training with regular updates and/or revalidation should be implemented for all health care staff using POCT equipment and managed in line with local laboratory guidance, and POCT meters should be regularly checked with internal quality control material and participation in external quality assurance must be undertaken.
In summary, advances in technology and a better understanding of the pathophysiology of DKA have led to a move away from traditional markers of disease severity to focus more on the major problem – the hyper-ketonaemia and resultant acidosis in DKA. The use of POCT equipment is now widely accepted among clinicians specializing in diabetes following the introduction of the JBDS guideline in 2010. Limitations of POCT blood ketone quantitation are acknowledged, but its potential advantages are substantial and seem to outweigh concerns around margins of error with absolute values. It is likely, therefore, with the improvement in technology that the use of these bedside testing meters is likely to increase.
Footnotes
Acknowledgements
I am grateful to the medical information departments of Abbot Laboratories Ltd and A Menarini Diagnostics for the help in supplying me with the data on their meters.
Declaration of conflicting interests
KD was the lead author on the second edition of the JBDS guideline on the management of DKA in adults referred to in the text. KD is a full time employee of the UK National Heath Service.
Funding
Travel to meetings for the writing group during production of the guideline was paid for by Diabetes UK.
Ethical approval
Not required.
Guarantor
KD.
Contributorship
KD is the sole author.