
Abstract
Background
Angiogenesis is involved in the pathogenesis of diabetic retinopathy. Osteoprotegerin, a recently identified glycoprotein belonging to the tumour necrosis factor receptor superfamily, has been implicated to be correlated with angiogenesis. This study aims to determine whether serum and vitreous concentrations of osteoprotegerin are associated with diabetic retinopathy.
Methods
This study consisted of 254 diabetic patients (100 without diabetic retinopathy, 64 with non-proliferative diabetic retinopathy and 90 with proliferative diabetic retinopathy) and 62 control subjects. Serum and vitreous concentrations of osteoprotegerin were evaluated using enzyme-linked immunosorbent assay method.
Results
Serum and vitreous osteoprotegerin concentrations in proliferative diabetic retinopathy patients were significantly elevated compared with those of the other three groups. Non-proliferative diabetic retinopathy patients showed elevated concentrations of serum and vitreous osteoprotegerin compared with patients without diabetic retinopathy. In addition, control subjects had significantly lower serum and vitreous osteoprotegerin concentrations compared with diabetic patients without retinopathy, non-proliferative diabetic retinopathy patients and proliferative diabetic retinopathy patients.
Conclusions
Serum and vitreous osteoprotegerin concentrations are associated with the presence and severity of diabetic retinopathy.
Introduction
Diabetic retinopathy is one of the leading causes of decreased vision and blindness in industrialized countries. Proliferative diabetic retinopathy is one of the most severe complications of diabetes mellitus. 1 Proliferative diabetic retinopathy is characterized by pericyte loss, microaneurysms, macular edema and subsequently retinal neovascularization, and vitreous haemorrhage. 2 Neovascularization, which is the most important pathogenesis in proliferative diabetic retinopathy, is closely correlated with the vascular, metabolic, endocrine, haematologic and immunological mechanisms by promoting the expression of various inflammatory cytokines and angiogenic factors. 3
Osteoprotegerin, a soluble member of the tumour necrosis factor (TNF) superfamily, regulates bone metabolism by mediating the paracrine signalling between osteoblasts and osteoclasts. 4 Osteoprotegerin prevents the receptor activator of nuclear factor-κB ligand (RANKL), a TNF-family member, from binding to its receptor RANK on osteoclast precursors, thereby to inhibit osteoclast maturation. Osteoprotegerin is predominantly released in the bone, but is also expressed in various tissues, including the lung, heart and blood vessels. 5 Osteoprotegerin has recently been implicated in vascular systems. Osteoprotegerin-deficient mice develop vascular calcifications of the same linear type in the tunica media of similar linear types as those commonly observed in diabetes. 6 Osteoprotegerin directly promotes endothelial cell proliferation in sprouting microvessels, which indicating its role in angiogenesis. 7 Therefore, osteoprotegerin is hypothesized to be involved in the pathogenesis of diabetic retinopathy.
This study aims to determine the association of the serum and vitreous concentrations of osteoprotegerin and the presence and severity of diabetic retinopathy.
Materials and methods
Study population
This cross-sectional study included 254 patients with type 2 diabetes (90 with proliferative diabetic retinopathy, 64 with non-proliferative diabetic retinopathy and 100 without diabetic retinopathy) who underwent pars plana vitrectomy for prolonged vitreous haemorrhage and tractional retinal detachment involving macular lesions. Patients who had previous intraocular surgery, other ocular disorders such as uveitis, glaucoma and corneal neovascularization, other systemic diseases including heart failure, renal failure, haematologic, cardiologic and metabolic disorders other than diabetes, obvious vitreal haemorrhage within the previous three months were excluded from this study. The control group consisted of 62 age-matched non-diabetic patients with retinal detachment who required vitrectomy, but in which the retina was not directly affected by neovascularization. These patients were free of systemic disorders, particularly diabetes, cardiovascular disorders, hypertension, lung disease and cancer. All subjects including patients and healthy controls in this study were all Chinese Han population. All participants provided written informed consents, and the Committee on Medical Ethics of our hospital, in accordance with the Declaration of Helsinki of the World Medical Association, approved the study protocol.
Laboratory methods
Undiluted vitrectomy samples (approximately 0.3 mL) were obtained using a standardized three-port closed vitrectomy technique with manual suction before the infusion set was opened. Blood samples were collected and the vitreous samples were immediately centrifuged at 3000 rotations per minute (rpm) for 10 min at 4℃. The liquid component without sediments was immediately stored at −80℃. The serum and vitreous samples were analyzed for osteoprotegerin using commercially available enzyme-linked immunosorbent assay (R&D Systems Inc., Minneapolis, MN, USA).
Statistical analysis
Statistical analysis was performed using SPSS version 13.0 software (SPSS Inc, Chicago, IL). The results were expressed as means ± standard errors or median (interquartile range). Data normality was analyzed using the Kolmogorov–Smirnov test. Comparisons of the categorical, normally distributed continuous, and not normally distributed continuous variables among the control subjects, diabetic patients without retinopathy, non-proliferative diabetic retinopathy patients and proliferative diabetic retinopathy patients were performed using Chi-square tests, one-way analysis of variance (ANOVA) or Kruskal–Wallis test, respectively. P < 0.05 was considered to be statistically significant.
Results
Baseline clinical characteristics
Clinical and biochemical characteristics of diabetic patients and controls.
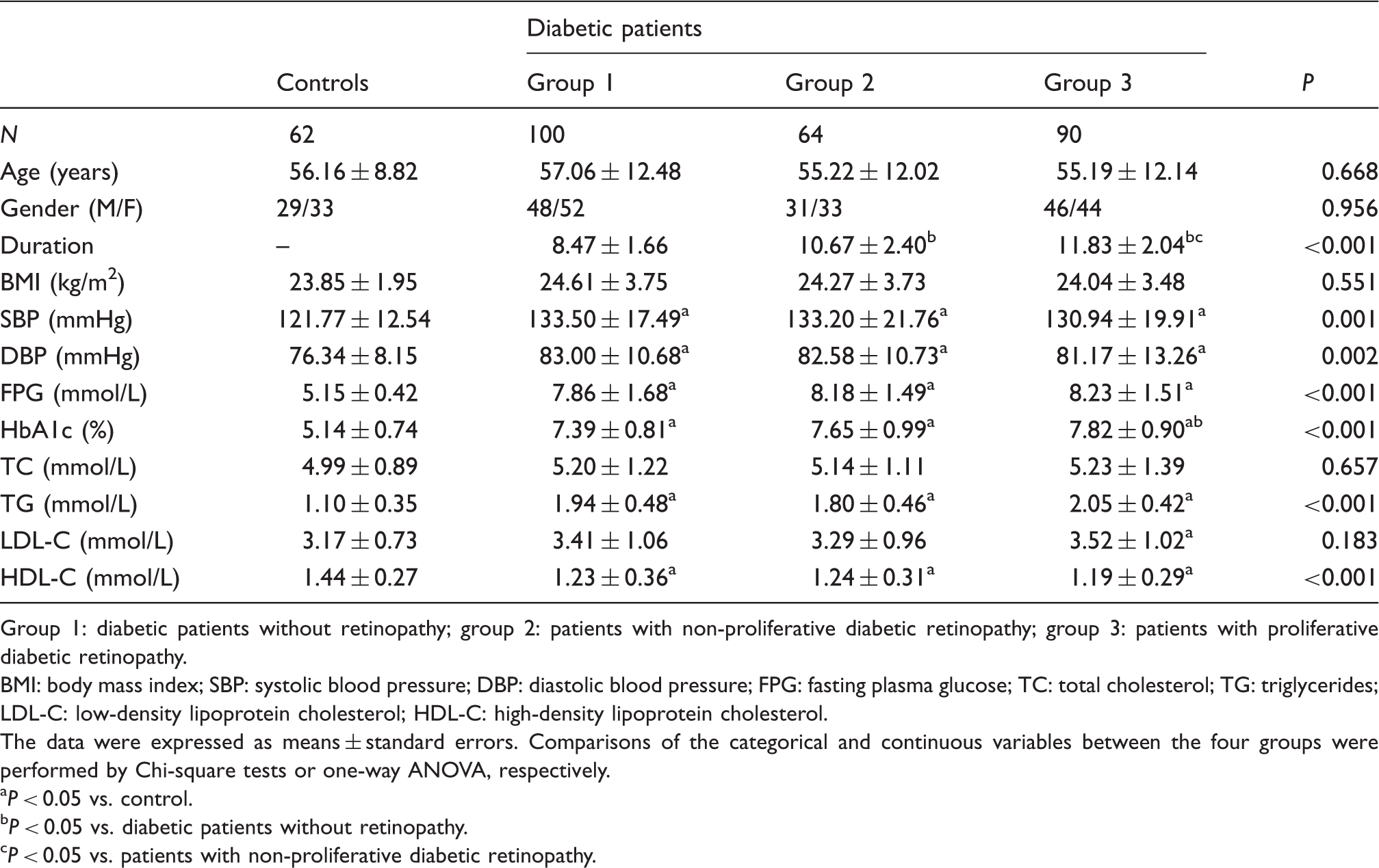
Group 1: diabetic patients without retinopathy; group 2: patients with non-proliferative diabetic retinopathy; group 3: patients with proliferative diabetic retinopathy.
BMI: body mass index; SBP: systolic blood pressure; DBP: diastolic blood pressure; FPG: fasting plasma glucose; TC: total cholesterol; TG: triglycerides; LDL-C: low-density lipoprotein cholesterol; HDL-C: high-density lipoprotein cholesterol.
The data were expressed as means ± standard errors. Comparisons of the categorical and continuous variables between the four groups were performed by Chi-square tests or one-way ANOVA, respectively.
P < 0.05 vs. control.
P < 0.05 vs. diabetic patients without retinopathy.
P < 0.05 vs. patients with non-proliferative diabetic retinopathy.
Serum and vitreous osteoprotegerin concentrations between the three groups
Serum and vitreous osteoprotegerin concentrations between the four groups.
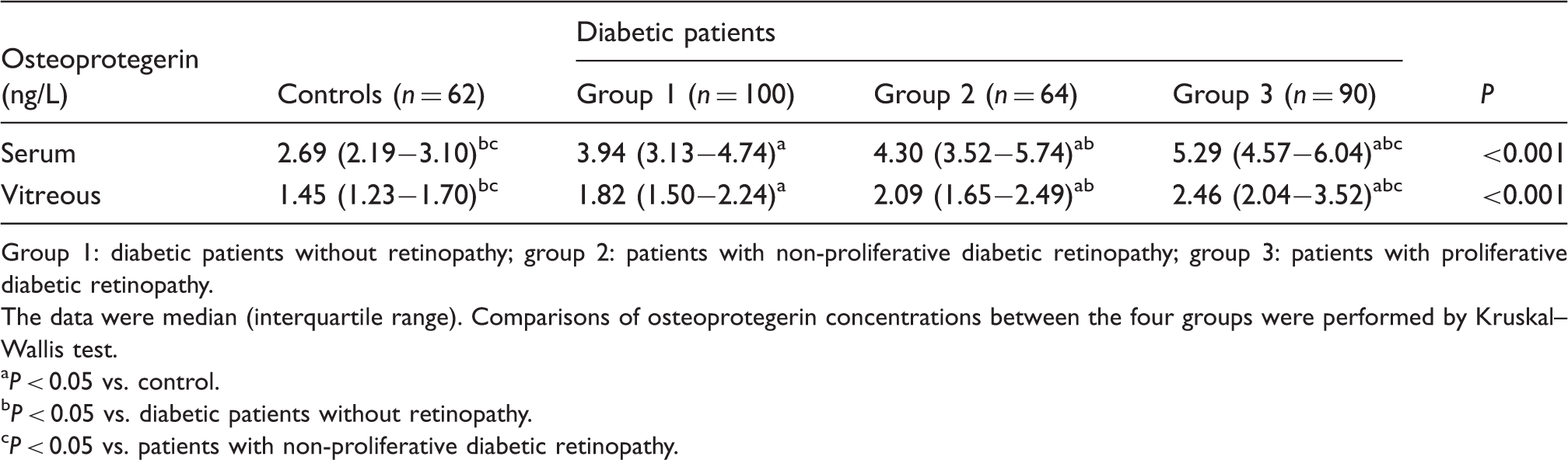
Group 1: diabetic patients without retinopathy; group 2: patients with non-proliferative diabetic retinopathy; group 3: patients with proliferative diabetic retinopathy.
The data were median (interquartile range). Comparisons of osteoprotegerin concentrations between the four groups were performed by Kruskal–Wallis test.
P < 0.05 vs. control.
P < 0.05 vs. diabetic patients without retinopathy.
P < 0.05 vs. patients with non-proliferative diabetic retinopathy.
Discussion
In the present study, proliferative diabetic retinopathy and non-proliferative diabetic retinopathy patients had significantly higher serum and vitreous osteoprotegerin concentrations than the healthy controls. To the best of our knowledge, this is the first cross-sectional study that demonstrates the association of serum and vitreous osteoprotegerin concentrations with the presence of diabetic retinopathy.
Osteoprotegerin, a member of the TNF receptor superfamily, has been originally characterized based on its ability to suppress osteoclast formation. Osteoprotegerin binds to the receptor activator of RANKL, thereby blocking its activity and negatively affecting osteoclast differentiation. 8 In addition to its role in bone metabolism, osteoprotegerin has recently been implicated in the vascular system. 9 Recent studies have indicated that osteoprotegerin is associated with the development of diabetes. Serum osteoprotegerin increased early after the diabetes induction in both apoE-null and littermate mice, and is positively correlated with blood glucose concentrations. 10 Serum osteoprotegerin concentrations were found to be elevated in patients with type 2 diabetes 11 and type 1 diabetes. 12 These results point to the role of osteoprotegerin in the mechanism of diabetes.
Previous studies have mainly focused on the association of serum osteoprotegerin concentrations with the macrovascular complications of diabetes. Serum osteoprotegerin concentrations were significantly higher in diabetic patients with a combination of microalbuminuria and coronary artery disease than in those with microalbuminuria alone. 13 Elevated serum osteoprotegerin concentrations were association with silent myocardial ischemia in type 2 diabetes. 14 Plasma osteoprotegerin was significantly increased in diabetic patients with carotid and peripheral arterial diseases compared with patients without those diseases. 15 In addition, osteoprotegerin concentrations were statistically higher in diabetic patients with neuropathy than those without neuropathy.16,17 Recent investigations have been performed on the association of serum osteoprotegerin with diabetic microvascular complications, especially diabetic nephropathy. Osteoprotegerin concentrations were found to be significantly higher in the microalbuminuric subgroup of diabetic patients compared with the normoalbuminuric subgroup. Osteoprotegerin concentrations in the macroalbuminuria subgroup were significantly higher than those in the normoalbuminuria and albuminuria subgroups. 18 In addition, the current study indicates that proliferative diabetic retinopathy and non-proliferative diabetic retinopathy patients had significantly higher serum and vitreous osteoprotegerin concentrations compared with healthy controls, suggesting the important role of osteoprotegerin in diabetic retinopathy, another diabetic microvascular complication. Similar results were found in another study, in which the serum osteoprotegerin was significantly higher in the patients with diabetic maculopathy compared with subjects with normal glucose tolerance. 19 It is summarized that osteoprotegerin is closely related with diabetic macrovascular and microvascular complications.
The mechanism of the differences in the serum and vitreous osteoprotegerin concentrations between the three subgroups of diabetic patients is not clear. Diabetic retinopathy is always accompanied with diabetic nephropathy. Therefore, we hypothesized that the differences in osteoprotegerin concentrations may be resulted from the slower clearance of osteoprotegerin with prolonged duration of diabetic status.
Angiogenesis is a key process in diabetic retinopathy development. Osteoprotegerin is correlated with angiogenesis. Osteoprotegerin induces endothelial colony-forming cells (ECFC) activation and is a positive regulator of microvessel formation in vivo. 20 Osteoprotegerin/RANK/RANKL axis may be involved in vasculogenesis and strongly support a modulatory role in tissue revascularization. 20 Osteoprotegerin may interact with ECFC, thereby inducing an antiadhesive effect and promoting ECFC migration through a stromal cell-derived factor-1 (SDF-1)/CXCR4-dependent pathway. 21 Therefore, osteoprotegerin may be involved in the pathogenesis of diabetic retinopathy by promoting angiogenesis process. Another study showed that osteoprotegerin gene polymorphism is associated with diabetic retinopathy in Slovenian patients with type 2 diabetes. 22 This indicates that osteoprotegerin may contribute to the development of diabetic retinopathy through a genetic mechanism.
The limitation of the present study should be considered. First, the sample size is not large enough to reach definitive conclusions. Further studies with larger sample sizes are warranted. Second, this study is of a cross-sectional design, and the causative relation must be confirmed by future longitudinal studies.
In conclusion, serum and vitreous osteoprotegerin concentrations are correlated with the presence of diabetic retinopathy. Serum and vitreous osteoprotegerin concentrations may serve as new biomarkers in addition to the traditional methods for assessing the risk of diabetic retinopathy.
Footnotes
Declaration of conflicting interests
None declared
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Ethical approval
The ethics committee of The Second Affiliated Hospital of Soochow University (2013SAHSU0167).
Guarantor
Contributorship
GY and SB researched literature and conceived the study. GY, XJ and JJ were involved in protocol development, gaining ethical approval, patient recruitment and data analysis. GY wrote the first draft of the manuscript. All authors reviewed and edited the manuscript and approved the final version of the manuscript.