
Abstract
Objective
Irisin, a recently identified myokine, is involved in the protection of mice against obesity and diabetes. This study aims to determine the serum and vitreous concentrations of irisin in patients with diabetic nephropathy and diabetic retinopathy.
Methods
A total of 178 patients with type 2 diabetes mellitus, as well as 22 type 2 diabetes mellitus patients without diabetic retinopathy and 35 patients with proliferative diabetic retinopathy were enrolled in this study.
Results
Serum irisin concentrations were significantly elevated in the control group compared with those in type 2 diabetes mellitus patients. Furthermore, type 2 diabetes mellitus patients with macroalbuminuria exhibited significantly lower serum irisin concentrations than the controls and type 2 diabetes mellitus patients with normoalbuminuria and microalbuminuria. Simple regression analysis showed that the serum irisin concentrations in type 2 diabetes mellitus patients were negatively correlated with age, fasting plasma glucose, homeostasis model assessment of insulin resistance, blood urea nitrogen, creatinine, and positively correlated with creatinine clearance and angiotensin-converting enzyme inhibitors/angiotensin receptor blockers treatment. Proliferative diabetic retinopathy patients showed significantly decreased serum and vitreous irisin concentrations compared with the control group and type 2 diabetes mellitus patients without diabetic retinopathy. Furthermore, decreased serum and vitreous irisin concentrations were found in type 2 diabetes mellitus patients without diabetic retinopathy than those in the controls.
Conclusion
Irisin concentrations are associated with the presence of diabetic nephropathy and diabetic retinopathy.
Introduction
Type 2 diabetes mellitus (T2DM) represents more than 90% of the diabetic population worldwide and contributes to 9% of global mortality corresponding to 4 million deaths per year. 1 Microvascular complications, including diabetic retinopathy (DR) and diabetic nephropathy (DN), affect nearly 60% and 20% of T2DM patients, respectively. 2 Microvascular complications are major causes of morbidity in the diabetic population. 3 The identification of biomarkers for microvascular diseases can provide new aspects about the pathogenesis of diabetic microvascular complications and thus facilitates early diagnosis, prevention and treatment.
Irisin, a recently identified myokine, is secreted upon exercise to promote thermogenesis and decrease body weight in mice. 4 Irisin is released into the circulation by cleavage of fibronectin type III domain containing protein 5 (FNDC5). 4 Circulating irisin significantly decreased in T2DM patients with renal insufficiency which is evaluated by glomerular filtration rate (GFR). 5 Therefore, it is interesting to know whether the serum irisin concentrations are correlated with different stages of albuminuria, as well as the presence and progression of DN. In addition, DR and DN are both diabetic microvascular complications. DR and DN exhibit similar pathogenesis, such as inflammation and oxidative stress. It is then hypothesized that vitreous irisin may be also associated with the development of DR. Thus, we designed two parallel studies to investigative the association of irisin concentrations with the presence of DN and DR, respectively.
Materials and methods
Patients
A total of 178 patients with T2DM were recruited from the inpatient department of Metabolic Disease Hospital of Tianjin Medical University. T2DM was diagnosed according to the American Diabetic Association criteria with a fasting glucose concentration ≥7.0 mmol/L or 2-h postprandial plasma glucose concentration ≥11.1 mmol/L. These patients were then divided into three groups according to urinary albumin excretion (UAE) 6 : those with normoalbuminuria (UAE < 30 mg/24 h; n = 82), those with microalbuminuria (30≤UAE ≤ 300 mg/24 h; n = 58), and those with macroalbuminuria (UAE > 300 mg/24 h; n = 38). Exclusion criteria included the presence of concomitant valvular heart disease, cardiomyopathy, acute renal failure, acute and chronic viral or bacterial infections, asthma, tumours and connective tissue diseases. Patients with type 1 diabetes mellitus were identified based on C-peptide measurements and were excluded from the study. Information about blood pressure treatment with angiotensin-converting enzyme inhibitors (ACEI) and angiotensin receptor blockers (ARB) was collected. Controls included 62 healthy subjects who underwent medical checkup in the medical checking centre. None was receiving medication or dietary supplements, and all had no history of diabetes.
To investigate serum and vitreous irisin concentrations in DR patients, we performed another study in Tianjin Eye Hospital where large samples of patients for eye disease and surgery were included
This study was approved by the research ethics committee of Metabolic Disease Hospital of Tianjin Medical University and Tianjin Eye Hospital
Measurements
Weight, height, systolic blood pressure (SBP) and diastolic blood pressure (DBP) were measured. Serum was obtained from the blood samples through centrifugation and stored at −80℃ until analysis. Serum triglycerides (TG), serum total cholesterol (TC), high-density lipoprotein cholesterol (HDL-C), low-density lipoprotein cholesterol (LDL-C), fasting plasma glucose (FPG), blood urea nitrogen (BUN) and creatinine (Cr) were tested using an auto biochemistry instrument (Hitachi 7170, Tokyo, Japan). UAE was detected by an auto biochemistry instrument (Hitachi 7170, Tokyo, Japan) (coefficient of variations [CVs] for intra assay: 4–5%; CVs for inter assay: 10–16% [detected among the concentrations ranged from 0.1 to 300 mg/24 h]; detection limit range: 0.1–300 mg/24 h). Blood HbA1c concentrations were measured through high-performance liquid chromatography. Serum insulin and urine albumin were measured by radioimmunoassay method (Diagnostic Products Corporation, Los Angeles, CA). Vitreous samples were collected undiluted using manual suction to a syringe through the aspiration line of vitrectomy before opening the infusion line. The vitreous samples were transferred on ice and then centrifuged, and the supernatants were stored at −80℃ until analysis. Serum and vitreous irisin concentrations were measured using an enzyme-linked immunosorbent assay (Phoenix Pharmaceuticals, Inc, USA) (coefficient of variations [CVs] for intra assay: 5–7%; CVs for inter assay: 12–15% [detected among the concentrations ranged from 0.1–1000 ng/mL]; detection limit range: 0.1–1000 ng/mL). BMI was calculated as weight in kilograms divided by height squared in metres (kg m−2). The homeostasis model assessment of insulin resistance (HOMA-IR) was calculated as the fasting insulin (µIU/mL) multiplied by plasma glucose concentration (mmol/L) and divided by 22.5. Creatinine clearance (Ccr) was calculated using the Cockroft-Gault formula. 7
Statistical analysis
Sample size was determined by power analysis and sample size software with α of 0.05 and power of 90%. Therefore, a minimum of 25 and 20 subjects in each group would detect a difference in irisin concentrations for DN and DR study, respectively. Data were displayed as means ± SD or median (interquartile range). Data normality was analysed using the Kolmogorov-Smirnov test. The following tests were performed to determine the differences among the three groups of patients with T2DM and control subjects: Chi-square tests to determine the differences between gender and ACEI/ARB treatment; Kruskal-Wallis test to determine the differences among Ccr, UAE and serum irisin concentrations or one-way ANOVA to determine the differences among the other characteristics. Furthermore, the differences of gender, serum and vitreous irisin concentrations as well as the other characteristics between PDR patients, T2DM patients without DR and controls were compared by Chi-square tests, Kruskal-Wallis test or one-way ANOVA, respectively. The correlation between serum irisin and other parameters was analysed using Spearman correlation analysis. Then a multiple stepwise linear regression analysis was used to determine the contribution of various factors to serum irisin. Statistical analysis was carried out using SPSS (version 13.0) software program (SPSS Inc, Chicago, Illinois). Differences were considered significant at P < 0.05.
Results
Baseline clinical characteristics of T2DM patients and controls
Clinical characteristics of T2DM patients and controls.
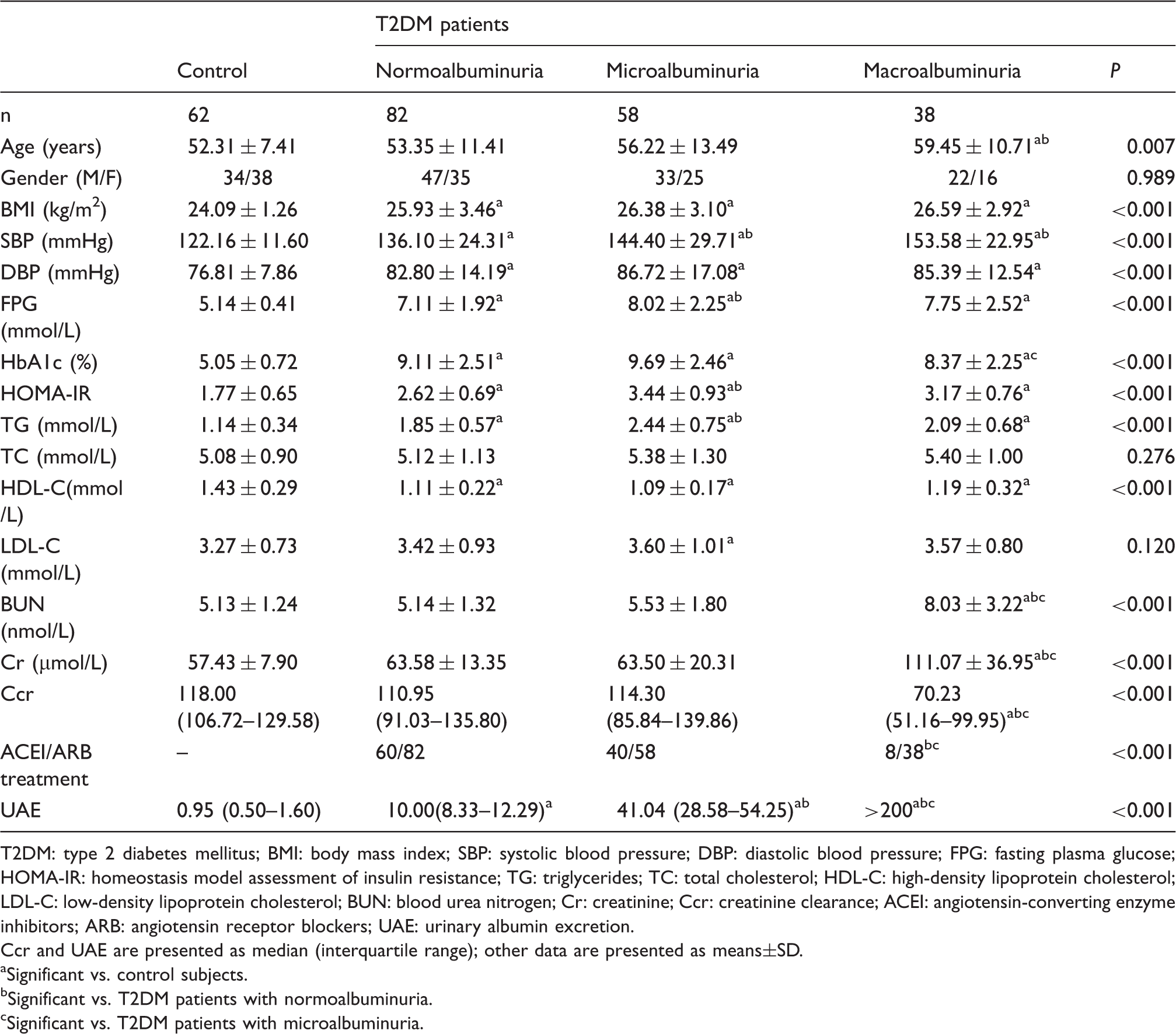
T2DM: type 2 diabetes mellitus; BMI: body mass index; SBP: systolic blood pressure; DBP: diastolic blood pressure; FPG: fasting plasma glucose; HOMA-IR: homeostasis model assessment of insulin resistance; TG: triglycerides; TC: total cholesterol; HDL-C: high-density lipoprotein cholesterol; LDL-C: low-density lipoprotein cholesterol; BUN: blood urea nitrogen; Cr: creatinine; Ccr: creatinine clearance; ACEI: angiotensin-converting enzyme inhibitors; ARB: angiotensin receptor blockers; UAE: urinary albumin excretion.
Ccr and UAE are presented as median (interquartile range); other data are presented as means±SD.
Significant vs. control subjects.
Significant vs. T2DM patients with normoalbuminuria.
Significant vs. T2DM patients with microalbuminuria.
Serum irisin concentrations in DN patients
Figure 1 shows the serum irisin concentrations in T2DM patients and healthy controls. Serum irisin concentrations were significantly elevated in the control group compared with those in T2DM patients. Furthermore, T2DM patients with macroalbuminuria demonstrated significantly lower concentrations of serum irisin than the other three groups. However, no significant differences in the serum irisin concentrations were observed between T2DM patients with normoalbuminuria and those with microalbuminuria.
Serum irisin concentrations in T2DM patients and healthy controls. Healthy subjects exhibited significantly elevated serum irisin concentrations compared with T2DM patients. Furthermore, T2DM patients with macroalbuminuria demonstrated significantly lower concentrations of serum irisin compared with the other three groups. However, no significant differences in serum irisin concentrations were found between T2DM patients with normoalbuminuria and microalbuminuria. (a) Significant versus control subjects. (b) Significant versus T2DM patients with normoalbuminuria. (c) Significant versus T2DM patients with microalbuminuria. The central box represents the values from the lower to the upper quartile (25 to 75%). The middle line represents the median. The horizontal line extends from the minimum to the maximum value.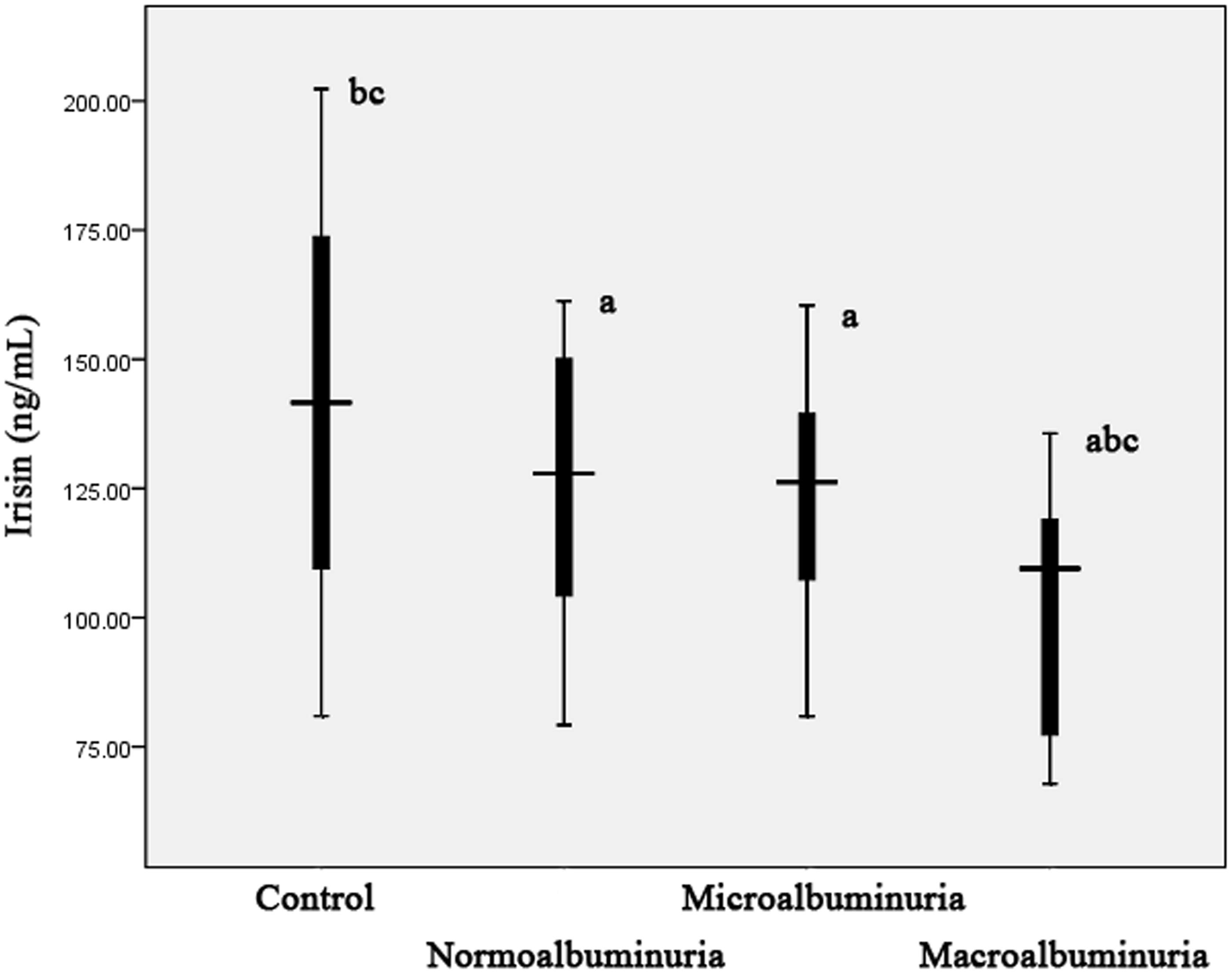
Association of serum irisin concentrations with other clinical characteristics
Simple regression analyses between serum irisin and various parameters.
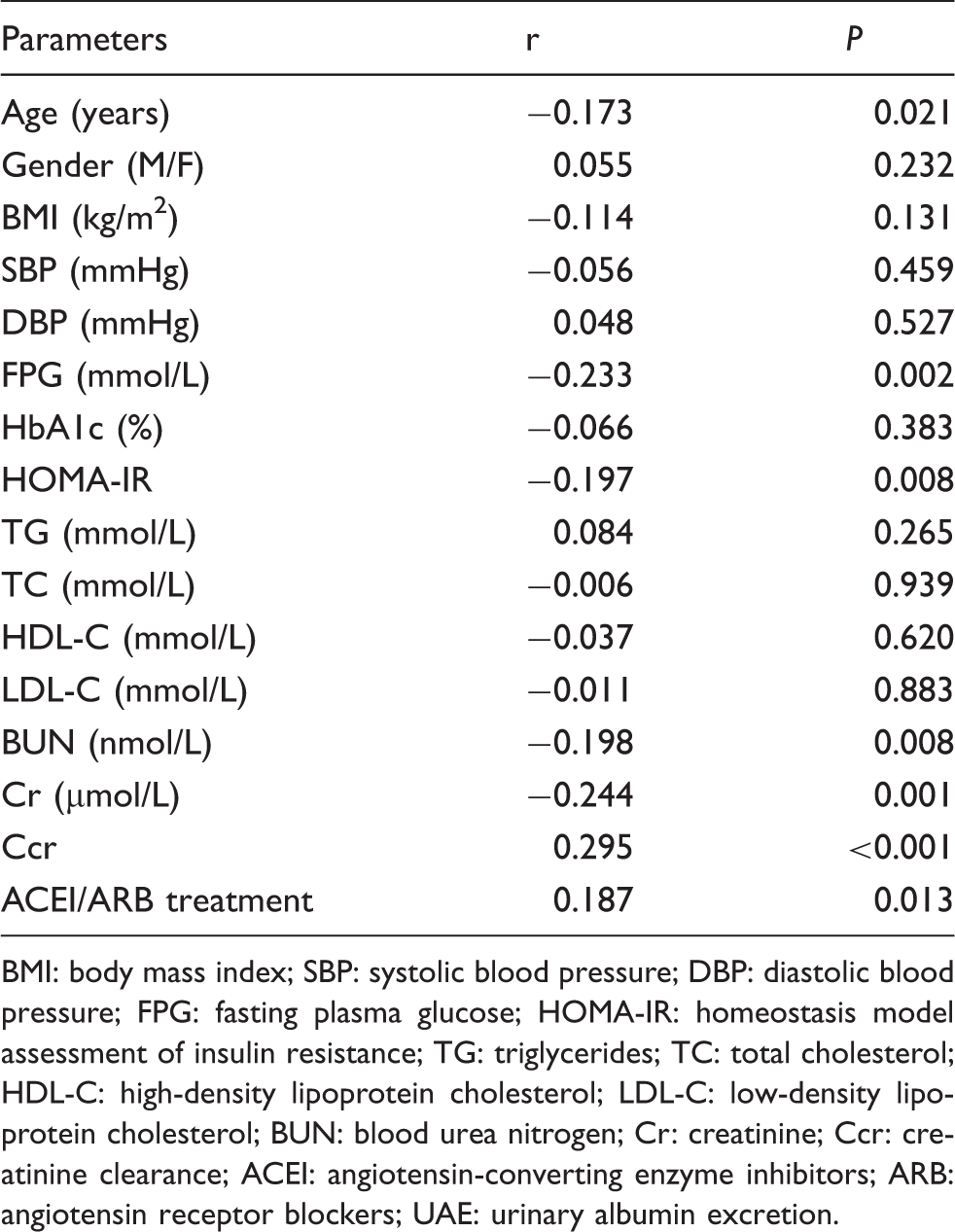
BMI: body mass index; SBP: systolic blood pressure; DBP: diastolic blood pressure; FPG: fasting plasma glucose; HOMA-IR: homeostasis model assessment of insulin resistance; TG: triglycerides; TC: total cholesterol; HDL-C: high-density lipoprotein cholesterol; LDL-C: low-density lipoprotein cholesterol; BUN: blood urea nitrogen; Cr: creatinine; Ccr: creatinine clearance; ACEI: angiotensin-converting enzyme inhibitors; ARB: angiotensin receptor blockers; UAE: urinary albumin excretion.
Baseline clinical characteristics of PDR patients, T2DM patients without DR and controls
Clinical characteristics of PDR patients, T2DM patients without DR and the controls.
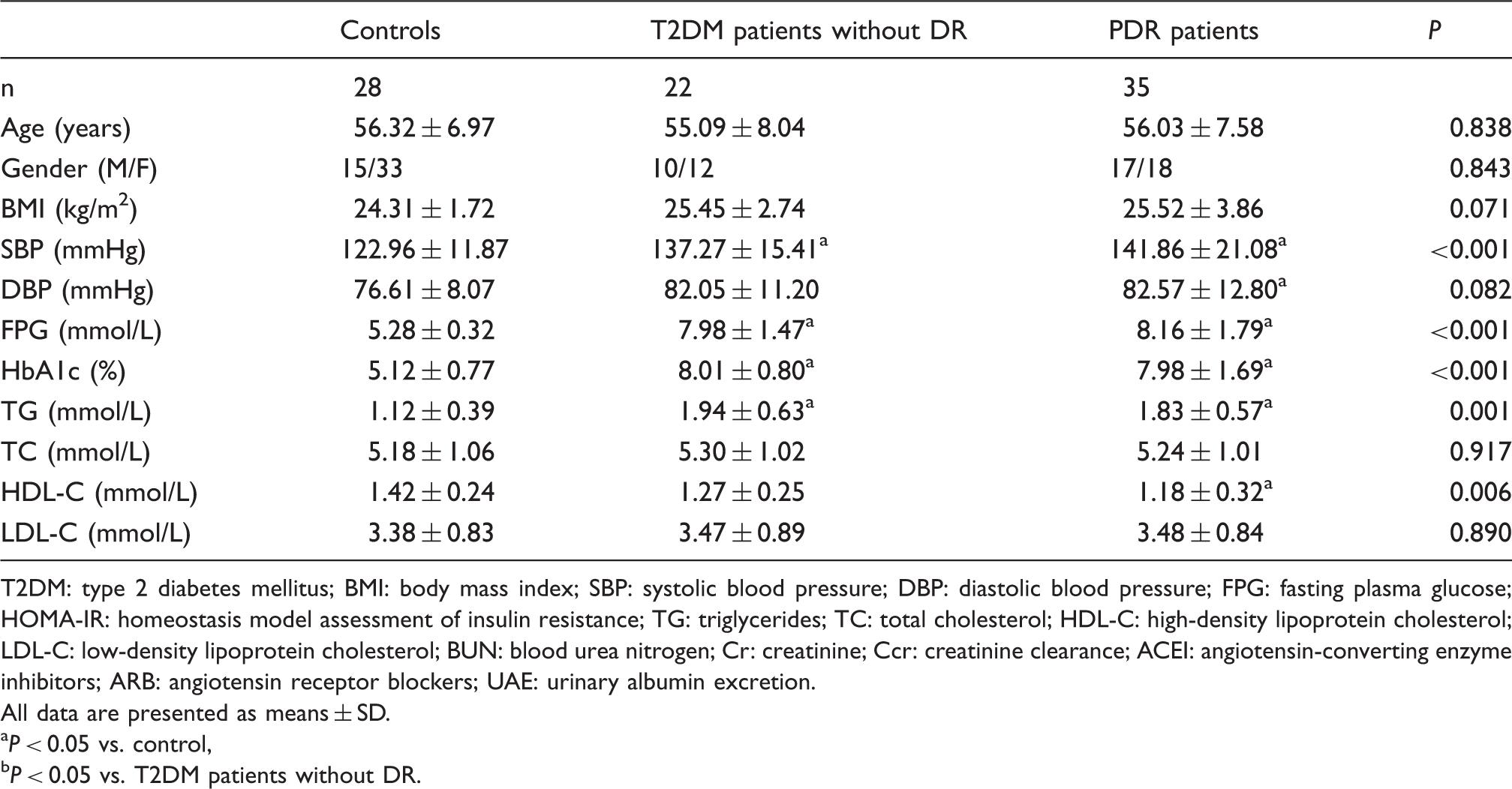
T2DM: type 2 diabetes mellitus; BMI: body mass index; SBP: systolic blood pressure; DBP: diastolic blood pressure; FPG: fasting plasma glucose; HOMA-IR: homeostasis model assessment of insulin resistance; TG: triglycerides; TC: total cholesterol; HDL-C: high-density lipoprotein cholesterol; LDL-C: low-density lipoprotein cholesterol; BUN: blood urea nitrogen; Cr: creatinine; Ccr: creatinine clearance; ACEI: angiotensin-converting enzyme inhibitors; ARB: angiotensin receptor blockers; UAE: urinary albumin excretion.
All data are presented as means ± SD.
P < 0.05 vs. control, bP < 0.05 vs. T2DM patients without DR.
Serum and vitreous irisin concentrations in PDR patients and controls
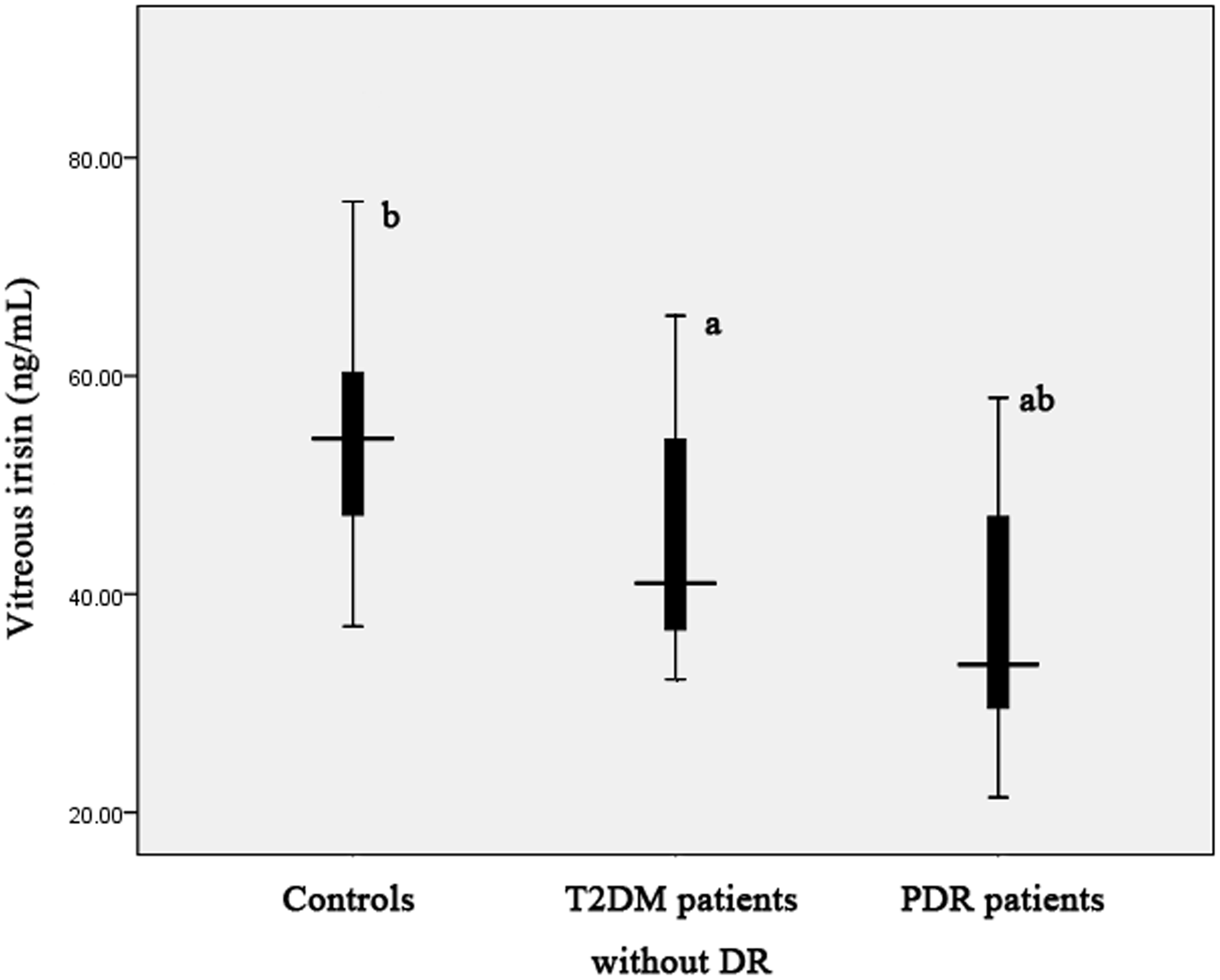
As shown in Figures 2 and 3, PDR patients showed significantly decreased concentrations of serum and vitreous irisin concentrations compared with the control group and T2DM patients without DR. Decreased serum and vitreous irisin concentrations were detected in T2DM patients without DR than those in the controls.
Serum irisin concentrations in PDR patients, T2DM patients without DR, and the controls. PDR patients demonstrated significantly decreased serum irisin concentrations compared with the controls and T2DM patients without DR. In addition, reduced serum irisin concentrations were found in T2DM patients without DR than those in the controls. (a) Significant versus the controls. (b) Significant versus T2DM patients without DR. The central box represents the values from the lower to the upper quartile (25 to 75%). The middle line represents the median. The horizontal line extends from the minimum to the maximum value. Vitreous irisin concentrations in PDR patients, T2DM patients without DR, and the controls. Decreased concentrations of vitreous irisin were observed in PDR patients compared with the control group and T2DM patients without DR. Furthermore, T2DM patients without DR had significantly lower vitreous irisin concentrations compared with the controls. (a) Significant versus the controls. (b) Significant versus T2DM patients without DR. The central box represents the values from the lower to the upper quartile (25 to 75%). The middle line represents the median. The horizontal line extends from the minimum to the maximum value.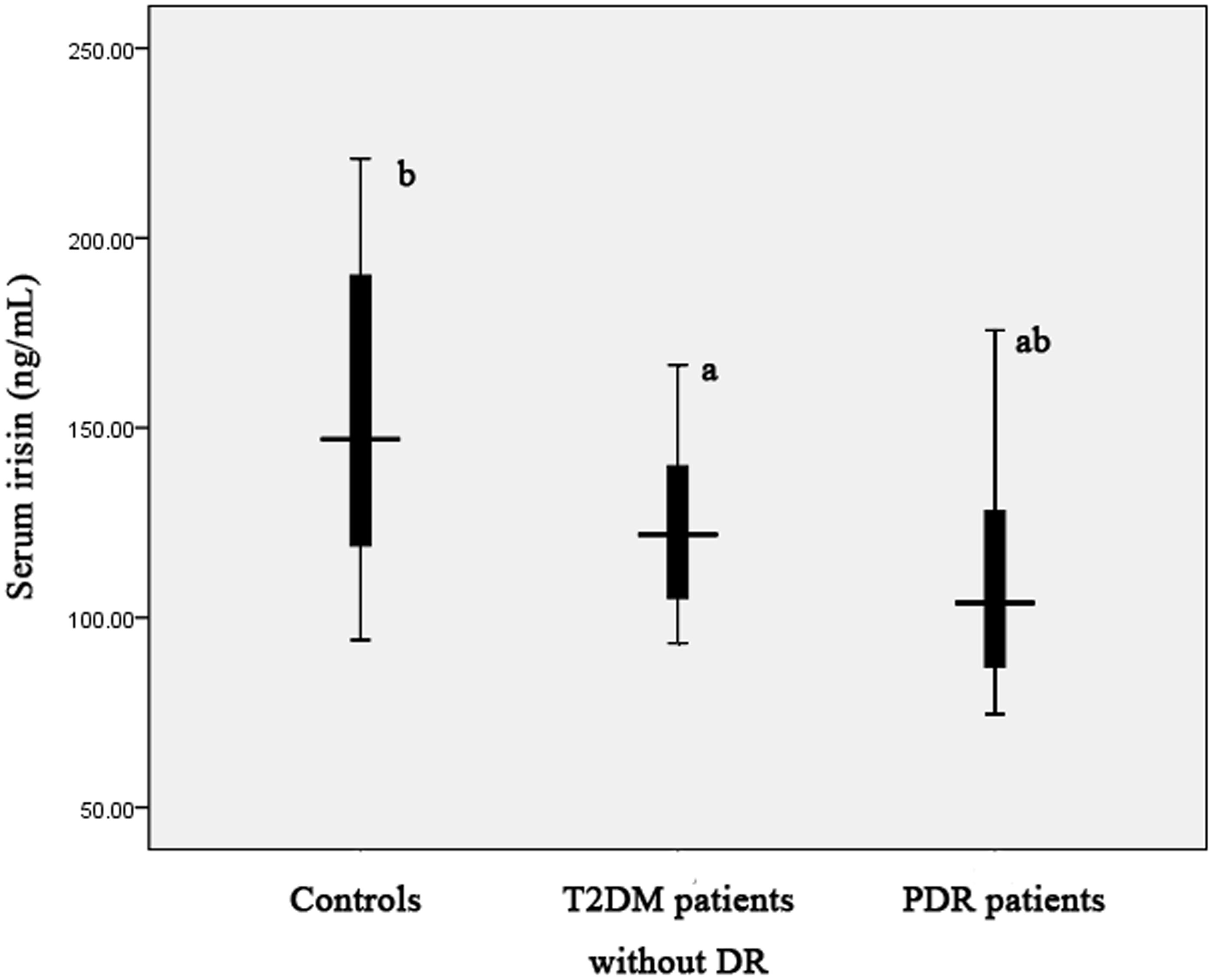
Discussion
The present results indicated that T2DM patients with macroalbuminuria had significantly lower concentrations of serum irisin compared with T2DM patients with normoalbuminuria and microalbuminuria. PDR patients showed significantly decreased concentrations of serum and vitreous irisin compared with the control group and T2DM patients without DR. To the best of our knowledge, this study is the first to demonstrate that irisin concentrations are associated with the presence of DR, as well as DN which is assessed using albuminuria.
Irisin, a newly discovered myokine, is induced by exercise in mice and humans, and is elevated with increased energy expenditure in mice. 2 Irisin could be a therapeutic target for human metabolic diseases and other disorders which can be improved with exercise. Irisin is correlated with glucose metabolism and diabetes. Irisin treatment significantly increased insulin-like growth factor 1 which is correlated with insulin sensitivity in human myocytes. 8 In human adipocytes, irisin induced uncoupling protein 1 and consequently increased adipocyte energy expenditure, resulting in the inhibition of lipid accumulation. 8 Subjects with higher irisin concentrations at baseline showed a greater reduction of glucose and insulin concentrations and the homeostasis model assessment index after dietary intervention for eight weeks. 9 Circulating irisin concentrations were inversely correlated with fasting blood glucose (FBG). 10 FBG was a significant predictor of circulating irisin. 10 Serum irisin concentrations were significantly lower in patients with T2DM compared with the healthy controls.11–14 The current study also obtained similar results which showed that T2DM patients with different stages of albuminuria exhibited reduced serum irisin concentrations compared with the controls. Nevertheless, no investigation has been focused on the association of circulating irisin concentrations with type 1 diabetes. Furthermore, subjects with gestational diabetes mellitus presented significantly lower serum irisin concentrations than the control subjects.15,16
Recent studies have indicated the association of irisin with macrovascular disease. Serum irisin concentrations were significantly elevated in T2DM patients with macrovascular complications. 11 In addition, serum irisin concentrations were increased gradually with the increase of flow-mediated dilation (FMD) concentrations. Multivariate stepwise regression analysis demonstrated that serum irisin concentrations were independently associated with FMD which is correlated with endothelial dysfunction. 12
It is then hypothesized that there may also be an association of irisin with diabetic microvascular complications. Wen et al. reported that plasma irisin concentrations were significantly decreased in patients with chronic kidney disease (CKD) compared with normal subjects. 17 Serum irisin concentrations significantly decreased with increased CKD stages and lowest irisin concentrations were seen in patients with CKD stage 5. 18 Another study showed that circulating irisin concentrations were significantly decreased in T2DM patients with renal insufficiency which is established by glomerular filtration rate (GFR). 5 All these studies evaluated the renal dysfunction using GFR. Our investigation assessed the correlation of serum irisin concentrations with UAE and found that T2DM patients with macroalbuminuria exhibited significantly lower concentrations of serum irisin compared with those with normoalbuminuria and microalbuminuria. In addition, serum irisin concentrations were correlated with renal function characteristics, such as BUN, Cr and Ccr. This finding is consistent with those of other studies, which also suggested the association of serum irisin with BUN, Cr and GFR.5,17,18 Hence, irisin possibly plays a protective role in the mechanism of DN.
DR and DN are both microvascular complications of T2DM. The current results showed that the serum and vitreous concentrations of irisin significantly decreased in PDR patients compared with the controls and T2DM patients without DR. Our results indicated that irisin may be involved in the pathogenesis of DR. Inflammation plays an important role in the development of DR. 19 Polyzos et al. reported that serum irisin tended to be higher in patients with portal inflammation compared with those without portal inflammation, which suggests the possible role of irisin in inflammation regulation. 20 Therefore, irisin may indirectly contribute to the development of DR by regulating inflammation. Further studies must be performed to elucidate the exact mechanism of irisin in DR.
Simvastatin significantly increased irisin secretion and induced cellular reactive oxygen species concentrations in human skeletal muscle cells. In addition, the increased irisin secretion by simvastatin could be reversed by antioxidant treatment, partially implying that irisin is secreted because of increased mitochondrial oxidative stress. 21 This indicates that irisin may function as an antioxidant regulator. Oxidative stress plays a key role in the pathogenesis of DN and DR. It is then hypothesized that irisin may protect T2DM patients from DR by suppressing the oxidative stress pathway.
Vitreous irisin concentrations are lower than serum irisin concentrations. This indicates that vitreous irisin may be caused by bleeding from the vascular system of the eyes. Irisin in eyes may protect the eyes against DR development. Therefore, decreased vitreous irisin concentrations in DR patients may explain the presence and progression of DR.
This study has several potential limitations. First, the sample size was not large enough to formulate definitive conclusions. Further studies with a large sample size are therefore warranted. Second, our study is of cross-sectional design, and the causative relation must be confirmed by future longitudinal studies. Third, irisin is closely related to exercise. We did not determine the effects of exercise on serum irisin concentrations in the present study. This limitation will be assessed in our future research.
In conclusion, serum irisin concentrations are correlated with renal function and the presence of DN. Furthermore, serum and vitreous irisin concentrations are associated with the development of DR. Our findings may support the possibility of irisin as a therapeutic target for the treatment of diabetic microvascular complications.
Footnotes
Declaration of conflicting interests
None.
Funding
Specialized Research Fund for the Doctoral Program of Higher Education.
Ethical approval
The ethics committee of Metabolic Disease Hospital of Tianjin Medical University (2014MDHTMU0158) and Tianjin Eye Hospital (2014TEH0215).
Guarantor
WW.
Contributorship
WH and WW researched literature and conceived the study. RW, JL, and JZ were involved in protocol development, gaining ethical approval, patient recruitment and data analysis. WH wrote the first draft of the manuscript. All authors reviewed and edited the manuscript and approved the final version of the manuscript.