
Abstract
Alkaline phosphatase is an enzyme present in all tissues of the human body. Several isoforms of this enzyme have been described with different catalytic nature, stability and antigenic structure. Rises in the activity of alkaline phosphatase are recognised in various states including bone diseases, liver disease, pregnancy, hyperthyroidism and malignant processes. The Regan isoenzyme, a rare variant of placental alkaline phosphatase, has been identified circulating in association with various tumours. The reported case describes a rising Regan isoform of alkaline phosphatase concentrations that led to a new diagnosis of occult renal cell carcinoma and persistently elevated activity postoperatively signposting persistent or recurrent disease.
Keywords
Case report
A 71-year-old woman was referred from primary care with a history of persistently elevated alkaline phosphatase (AP) for 11 months prior to referral, with normal results for serum bilirubin, transaminases and γ-glutamyl transpeptidase. Laboratory records had shown previous AP results to be within reference limits. Medical and surgical history included chronic obstructive pulmonary disease (COPD), primary hypothyroidism, dyslipidaemia, obesity, hysterectomy and a history of recurrent drop-attacks likely secondary to partial complex seizures which responded well to carbamazepine treatment. The list of daily medications included thyroxine, atorvastatin, carbamazepine, vitamin D, folic acid, paracetamol, as well as regular inhalers (tiotropium, salbutamol and a combined budesonide/formoterol preparation). There was a family history of colon cancer.
The myeloma screen was negative. Plasma carbamazepine concentration was stable and within the therapeutic interval since 2009. Hypovitaminosis D (25 hydroxyvitamin D concentration = 21 nmol/L) was corrected with oral cholecalciferol supplementation, but a few months later despite being vitamin D replete (62 nmol/L), AP concentrations remained elevated and continued to rise further. Serum C-terminal collagen cross-links were 0.31 µg/L (reference interval: 0.10–0.50) with parathyroid hormone within the reference interval, indicating no biochemical evidence of a disturbance in bone turnover. Isoenzyme analysis, performed using the Sebia Hydragel ISO-PAL electrophoresis kit (Sebia, Evry Cedex, France) revealed that the major proportion of elevated AP was due to the highly antibody-complexed Regan isoenzyme with only some liver, a trace of biliary and bone isoforms detected (Figure 1). Additionally, the low electrophoretic mobility Regan isoenzyme band remained present following heating the specimen at 65℃. This unusual and unexpected finding prompted further tests, as the Regan isoenzyme, which shares similar characteristics with the placental AP, can be associated with occult malignancies.
Alkaline phosphatase isoenzyme analysis. Key: electrophoretic tracks from the left: Track 1: RIAP heat stability 82% at 56℃; Track 2: RIAP after precipitation of globulins with PEG; Track 3: RIAP after heat treatment at 65℃; Track 4: liver and bone AP isoenzymes; Track 5: Bone quality control sample; Track 6: liver quality control sample; Track 7: intestinal quality control sample; Track 8: quality control sample after neuraminidase treatment; Track 9: quality control sample without neuraminidase – confirming increased intestinal isoenzyme; Track 10: other patient heat stability 16% (large increase in bone isoform).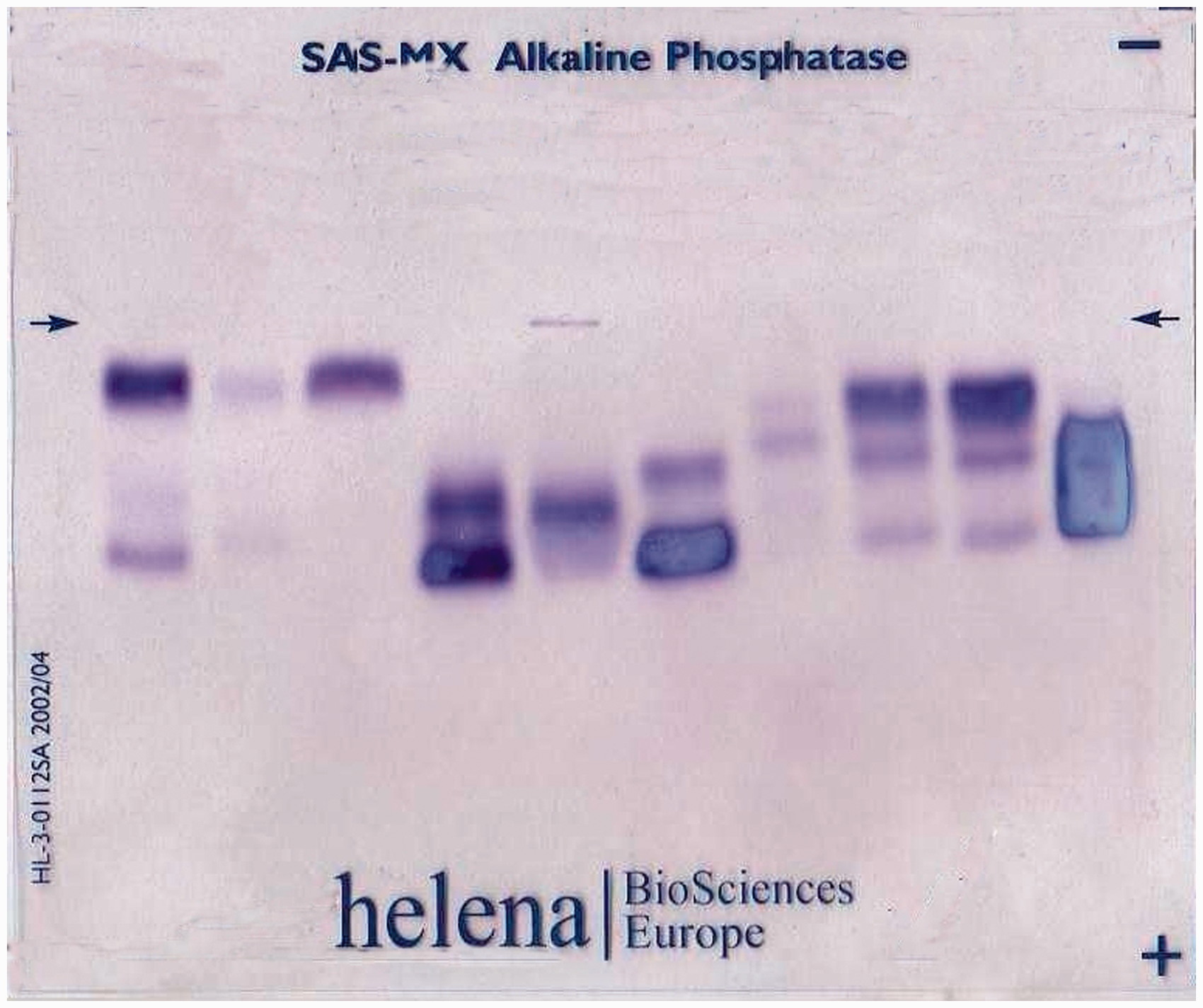
Upon detailed questioning of the patient there were no symptoms other than long-standing cough on a background of past extensive smoking history with mild residual COPD. Additionally, no suggestive signs could be elicited on thorough physical examination. A subsequent chest X-ray was reported as normal. With a high index of clinical suspicion for malignancy, the patient was referred for further investigation. Carcinoembryonic antigen (CEA), CA19-9, CA125, α-fetoprotein (AFP), β-human chorionic gonadotropin (β-HCG) were normal and so was the remainder of patient’s laboratory investigations (full blood count, CRP, erythrocyte sedimentation rate (ESR), urea and electrolytes, bone profile, myeloma screen). Whole-body computed tomography (CT), including dedicated renal protocol revealed a dense 1.5 cm irregularly enhancing lesion in the right kidney with the radiological characteristics of Bosniak 3/4 renal cell cancer (RCC). There was no evidence of any distant metastases.
Changing liver function test results over time.
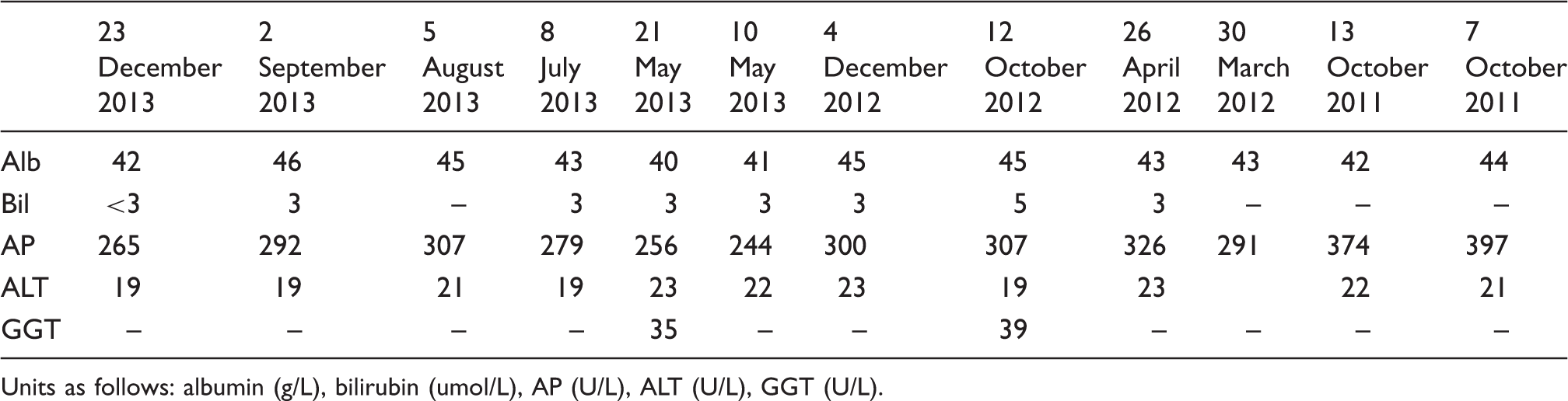
Units as follows: albumin (g/L), bilirubin (umol/L), AP (U/L), ALT (U/L), GGT (U/L).
Discussion
Tumour-related synthesis of embryonic gene products has important implications in the field of differentiation and laboratory diagnosis of cancer. Carcino-placental (‘Regan’) isoenzyme, a variant of oncofetal AP, is an example. It belongs to the placental-type alkaline phosphatase (PLAP) group – one of three major genetic groups of AP isoenzymes with the remaining two being intestinal-type AP, and early-pregnancy AP containing liver-, kidney- and bone-subtypes. 1 In healthy adults AP from the tissue non-specific locus constitutes around 95% of the total AP in the serum with equal contributions from bone and liver. Exploitation of the different properties of these isoenzymes such as structural variation, variable electrophoretic mobility or heat stability, underpins the ability to identify these to aid clinical practice.
Rises in the activity of this enzyme are recognised in various physiological and pathological states including pregnancy, first three months of life, puberty, postmenopause, blood group B or 0, smoking, drugs (i.e. oral contraceptives, phenytoin, ranitidine, erythromycin, carbamazepine, verapamil, allopurinol), bone and liver diseases, hyperthyroidism and malignant processes. 2
Elevated AP is well recognised as a marker of increased osteoblastic activity due to bone metastases in many forms of cancer. However, in addition it can be produced directly from the malignant cells.
It is well established that some malignant neoplasms produce substances which cannot be otherwise synthesised in significant quantities by their tissue of origin. 3 Paraneoplastic activity causing increased concentrations of AP is correlated to poorer prognosis. There have been reports that not only common but also specific AP isoenzymes appear in the serum samples of people diagnosed with cancer. 1 Malignant tissue transformations are in some cases associated with appearance of fetal-type proteins such as RIAP. 4 In an unselected population of 239 patients with malignant tumours, 25% were identified as having increased RIAP activity within the serum using immunological methods of identification. 5
The Regan isoenzyme of AP, a heat-stable and
At present our understanding of the role of Regan isoenzyme in relation to various tumours remains limited. However, further studies on placental AP – abundantly expressed by multiple neoplasms, and possessing identical enzymatic, physical and immunological characteristics to the Regan isoenzyme – may provide a better understanding of RIAP and its potential application to diagnosis and monitoring of numerous malignancies. 8
Medline and Scopus databases were searched for all English-language articles reporting an association between RIAP and all types of cancers. We identified one study from 1971 on a group of RCC patients which reported the presence of the RIAP in one case. 15 However, the link between RIAP and RCC has not been otherwise reported. The present case report highlights the utility of characterising the AP isoenzyme in the situation of an isolated increase of this enzyme. Furthermore, the association may inform further research on the biology of RCC.
Footnotes
Acknowledgements
The authors thank Dr KB Page, Associate Specialist in Chemical Pathology at Sheffield Teaching Hospitals NHS Foundation Trust for performing AP isoenzyme analysis and providing the images.
Declaration of conflicting interests
Not applicable.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Ethical approval
No ethical approval was required. Written consent was obtained from the patient.
Guarantor
JB.
Contributorship
JB wrote and edited the manuscript, and contributed to the discussions. SP, FJ and RQ contributed to the discussions, reviewed and edited the manuscript.