
Abstract

The case report in this issue by Akinosoglou et al. 1 describes increased serum amylase activity in a patient with a small oat cell tumour of the lung. Alpha amylase is a relatively small 45 kDa enzyme that breaks down glycogen and starch to maltose and dextrin. Amylase is a glycoside hydrolase which acts upon α-1,4-glycosidic bonds. It is located principally in the pancreas and salivary glands but is also found in other organs, including the gonads, fallopian tubes and intestinal tract. Total amylase activity in human plasma usually comprises pancreatic (P) and salivary (S) isoenzymes. 2
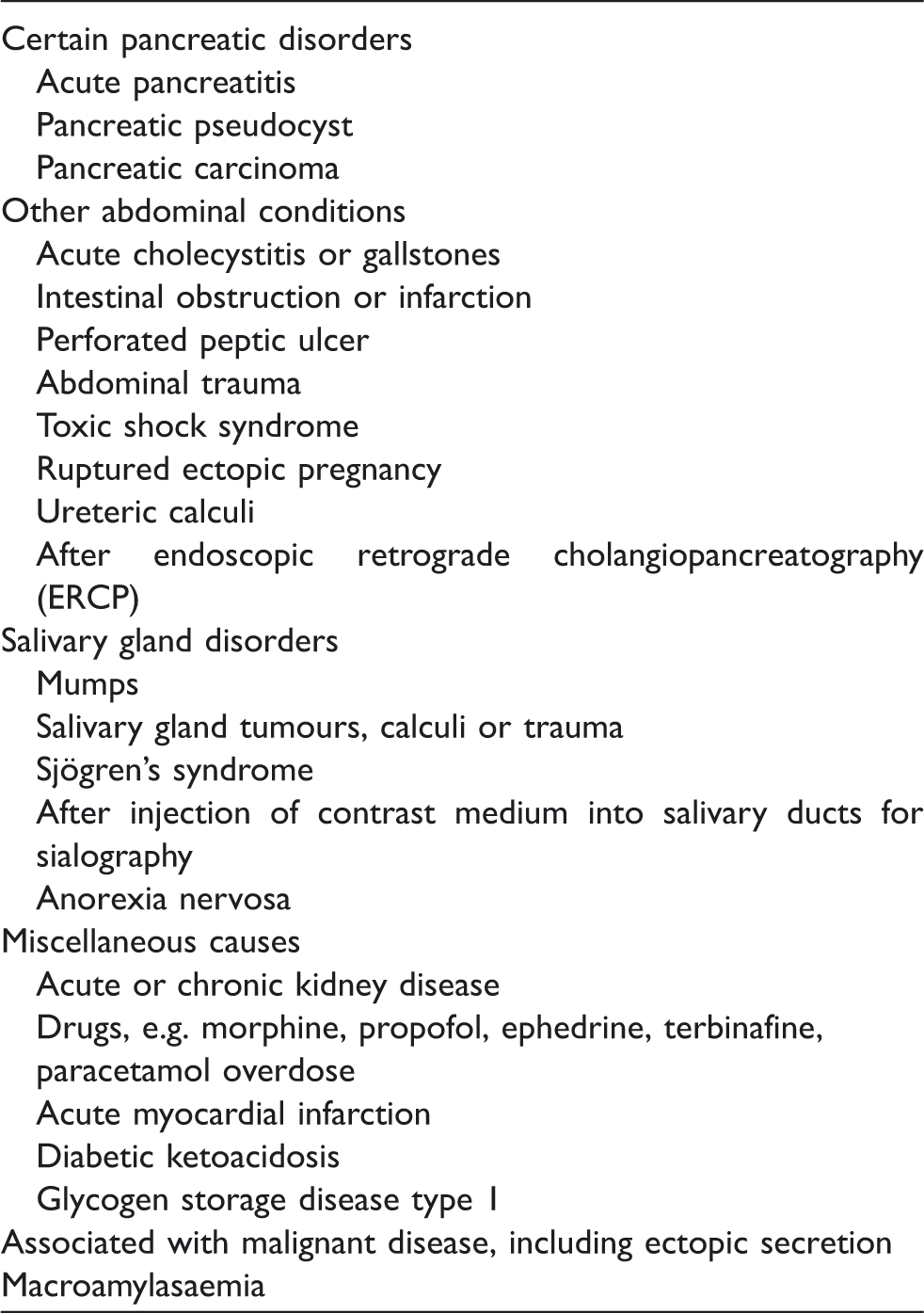
Some possible causes of hyperamylasaemia.
Alpha amylase is filtered by the renal glomeruli and excreted in the urine, hence its elevation in the plasma in certain renal disorders. In macroamylasaemia, amylase is bound to immunoglobulins and can be diagnosed by a low ratio of amylase clearance to creatinine clearance. Electrophoretic and chromatography techniques can also be used to determine macroamylasaemia. Macroamylasaemia is associated with certain autoimmune disorders including coeliac disease, ulcerative colitis and rheumatoid arthritis as well as lymphoma and human immunodeficiency virus (HIV) infection and after administration of hydroxyethyl starch.2,6
Hyperamylasaemia can also be associated with malignant disease. Serum amylase activity may be increased in some patients with multiple myeloma. A common feature of the myeloma cell lines associated with hyperamylasaemia was a translocation of chromosome 1, which harbours the gene for amylase.7–9 Shigemura et al. 10 reported that in multiple myeloma with hyperamylasaemia, a majority of cases were due to salivary-type hyperamylasaemia (sialyl salivary-type amylase). In patients with amylase-producing multiple myeloma, the onset of hyperamylasaemia was associated with a rapid disease progression associated with extensive bone destruction and increased mortality. It has been suggested that serum amylase activity may be a prognostic index of multiple myeloma disease progression. 11
Ovarian carcinomas12,13 are also associated with hyperamylasaemia as are some lung tumours. Amylase-producing tumours of the lung are rare and may comprise in total only 1–3% of all lung carcinomas and, in these cases, the salivary amylase isotype is generally found.14–18 As Akinosoglou et al. 1 point out, small cell lung carcinoma originates from Kulchitsky cells, which are of neural crest origin and able to secrete various polypeptide hormones and enzymes such as amylase. However, this hyperamylasaemia may also be due to an increase in the amylase content within the lung tissues; possibly the carcinoma provokes an inflammatory response resulting in release of amylase into the circulation.
There are also reports of hyperamylasaemia, usually the salivary amylase isotype, in some patients with phaeochromocytoma (paraganglioma). Here, the hyperamylasaemia may be transient and related to the hypertensive crisis evoked by the phaeochromocytoma. Rather than being a result of tumour ectopic secretion, the hyperamylasaemia may be due to tissue hypoxia secondary to high catecholamine concentrations that elicit vasoconstriction and decreased organ perfusion.19–21
In summary, there are many causes of hyperamylasaemia including as part of the paraneoplastic syndrome, as illustrated by Akinosoglou et al. 1
Footnotes
Declaration of conflicting interests
None declared.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Ethical approval
Not applicable.
Guarantor
MAC.