Abstract
The British and Irish Porphyria Network guidelines describe best practice in the clinical assessment, investigation and management of acute porphyria attacks and their complications, including severe attacks with neuropathy. Acute attacks of porphyria may occur in acute intermittent porphyria (AIP), variegate porphyria (VP) and hereditary coproporphyria (HCP). Aminolaevulinic acid dehydratase deficiency porphyria (ADP) is a very rare autosomal recessive porphyria; only six cases substantiated by mutation analysis have yet been described in the literature.
Urinary porphobilinogen (PBG) is always raised in an acute attack due to AIP, VP or HCP and this analysis is essential to confirm the diagnosis. A positive result in a qualitative or semi-quantitative screening test must be followed by PBG quantitation at the earliest opportunity. However in a severely ill patient, treatment should not be delayed.
Removal of precipitating factors, effective analgesia and control of symptoms with safe medication, attention to nutrition and fluid balance are essential. The indications for use of intravenous haem arginate are set out, together with advice on its administration. A small proportion of acute porphyria patients develop recurrent attacks and management options that may be considered include gonadotrophin-releasing hormone analogues, ‘prophylactic’ regular haem arginate infusion or ultimately, liver transplantation.
Scope of the guidelines
The guidelines provide a practical assessment and management tool for patients with acute porphyria attacks. Patients hospitalized with acute porphyria attacks are at risk of acute deterioration and the guidelines emphasize additional measures required when attacks are complicated by progressive neuropathy. Treatment options for patients with recurrent attacks are described.
Introduction
The porphyrias are a group of rare, mostly inherited disorders that are each caused by specific enzyme deficiencies, or in one porphyria, gain of function in the haem biosynthetic pathway. 1 Clinical features depend on the extent and type of pathway intermediates (aminolaevulinic acid [ALA], porphobilinogen [PBG] and porphyrins) that accumulate and biochemically characterize each disorder. The principal manifestations are acute neurovisceral attacks or photosensitive skin disease or both.1–3
Acute attacks of porphyria may occur in acute intermittent porphyria (AIP), variegate porphyria (VP) and hereditary coproporphyria (HCP), due to mutations in the hydroxymethylbilane synthase (HMBS), protoporphyrinogen oxidase (PPOX) and coproporphyrinogen oxidase (CPOX) genes, respectively. These three acute porphyrias are autosomal dominant disorders with low clinical penetrance. Patients with VP and HCP may also experience photosensitive skin lesions, not necessarily in association with acute attacks.
ALA dehydratase (ALAD) porphyria is an exceptionally rare autosomal recessive porphyria that may present in childhood or adulthood with prominent neuropathic features, sometimes with acute attacks. Only six cases (substantiated by mutation analysis) have been reported to date.4–6
Accurate and complete biochemical characterization of a new case of acute porphyria is essential for optimal management. Biochemical diagnosis requires specialist analytical techniques, expertise in interpretation and rigorous internal and external quality assurance.7–9 In addition, new probands should be counselled and offered genetic testing to identify the family-specific mutation as this enables at risk family members to be offered predictive testing. 10
Acute attacks
Clinical assessment
Recognition of an acute porphyia attack can be difficult as individual symptoms and signs are non-specific, particularly in the early stages. 11 Acute attacks are most common in young adults, and extremely rare before puberty. Women are more often affected than men. Patients are typically well between attacks. 12
Clinical features during an attack
Abdominal pain – severe, poorly localized. Pain can also affect back, legs and other sites; Nausea, vomiting, constipation; Dark urine – colour darkens to orange or red on exposure to light; Hypertension, tachycardia, and rarely, arrhythmias; Agitation, insomnia, confusion, psychosis with hallucinations and unusual behaviour; Convulsions – frequently associated with hyponatraemia; Peripheral motor neuropathy – may progress to flaccid paralysis, respiratory insufficiency, difficulty swallowing, urinary retention or incontinence; Hyponatraemia; Bullous skin lesions may be present during an acute of VP (about 50% of patients) or HCP (less than 20% of patients). Skin lesions do not occur in AIP (unless end stage kidney failure develops).
Precipitating factors
Drugs – typically newly prescribed medication, including antibiotics, oral contraception, anticonvulsants. Many commonly prescribed drugs are UNSAFE in acute porphyria. For information about SAFE prescribing in acute porphyria contact the Welsh Medicines Information Centre (see below); Alcohol; Reduction in calorie intake, e.g. fasting, dieting, gastrointestinal upset; Fluctuating sex hormone concentrations, especially increased progesterone. Attacks in women are more frequent in the luteal phase of the menstrual cycle. Pregnancy may trigger an attack but is usually well tolerated; Stress; Infection; Smoking; Illicit drugs.
Inheritance of AIP, VP and HCP is autosomal dominant, so a history may reveal an affected relative. However most carriers of the gene defect are likely to remain asymptomatic (penetrance is incomplete).
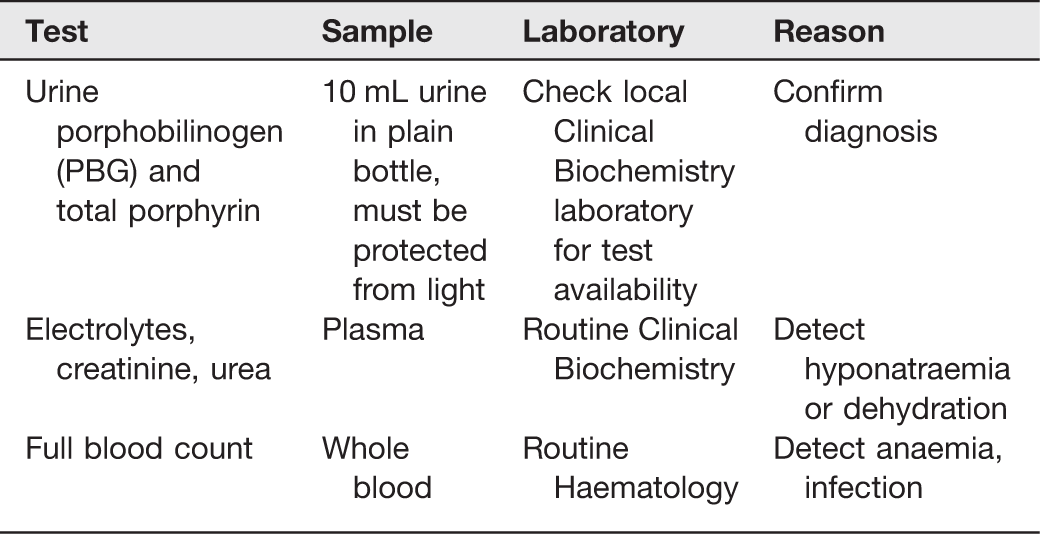
Initial investigations
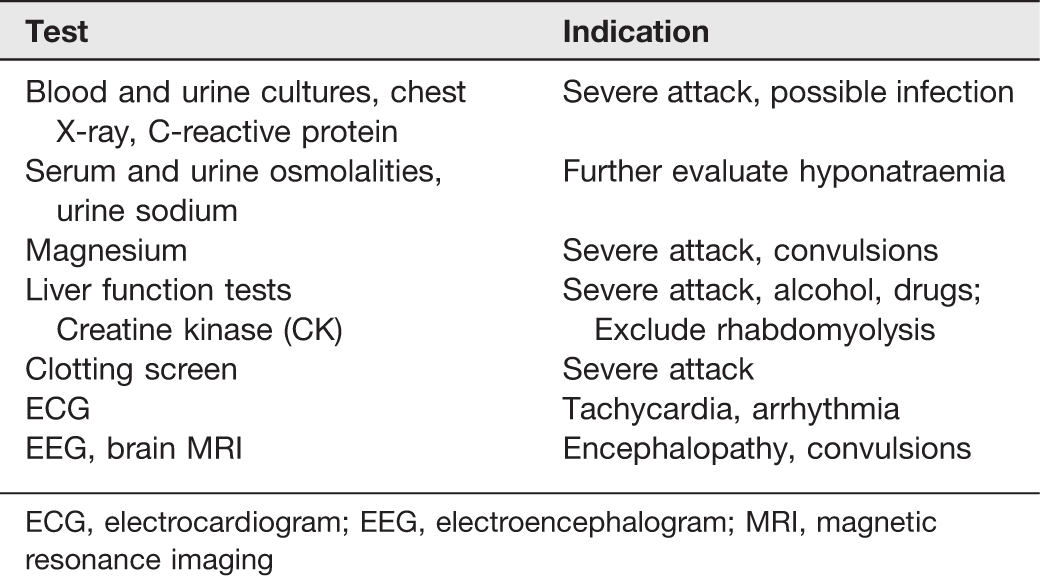
ECG, electrocardiogram; EEG, electroencephalogram; MRI, magnetic resonance imaging
Urine PBG
PBG analysis, preferably by a quantitative test, is essential and should be available within 24 h. A positive result in a qualitative or semi-quantitative screening test must be followed by PBG quantitation at the earliest opportunity (ideally using the same sample).11,13 However in a severely ill patient, treatment should not be delayed.
Semi-quantitative PBG analysis by the Trace® kit has sufficient sensitivity and specificity for initial testing and offers a suitable option for ‘out of hours’, urgent analysis.12,14
Urine PBG concentration is always raised in an acute attack of porphyria due to AIP, VP or HCP. Some patients with acute porphyria (especially AIP) have persistently elevated urine PBG concentrations. Interpretation of results in such patients is complex as it requires comparison with a recent baseline quantitative PBG:creatinine ratio in conjunction with clinical assessment. 15 PBG is not increased in ADP 4 and urine ALA should also be measured in children if acute porphyria is suspected.16,17
Urine PBG excretion may return to normal relatively quickly as symptoms resolve in VP and HCP. Where there is a delay in sample collection in these circumstances, PBG measurement alone is not sufficient to exclude acute porphyria and analysis of urine porphyrin is required. If increased, faecal and plasma porphyrin analysis is essential.
Management of an acute attack
Specific treatment is indicated only in patients with clinical features of an acute attack and increased excretion of porphobilinogen in the urine. In mild attacks (mild pain, no vomiting, no paralysis, no hyponatraemia), a high carbohydrate diet and supportive measures may be used for up to 48 h. However if neurological complications occur in the absence of other indicators of severity, treatment with haem arginate should be started immediately
Patients with severe attacks should be admitted to hospital for evaluation, control of symptoms and prompt treatment of complications. Symptoms usually improve within a few days of starting haem arginate, and most patients make a complete recovery in 1–2 weeks. Patients with neurological complications (convulsions, progressive neuropathy, respiratory insufficiency, encephalopathy), severe hyponatraemia (plasma sodium less than 120 mmol/L) or cardiac arrhythmias must be cared for in a High Dependency or Intensive Care Unit (see Section 2).
Remove precipitating factors
Review medication and check for safety in acute porphyria. New medication is a common trigger. Look for, and treat, infection.
Consider other causes of symptoms
For instance, abdominal pain in a patient with porphyria may be due to appendicitis, cholecystitis or a complication of pregnancy. Surgical or other appropriate opinions should be sought if other diagnoses are thought possible.
Human haemin
Intravenous haem arginate (Normosang®) is licensed for specific treatment of acute porphyria attacks and is available in Europe and many other countries worldwide. It is a concentrated human haemin solution, stabilized as a complex with arginine. In the USA, a lyophilized haemin preparation (Panhematin®) is used. Both act to reduce production of porphyrins and their precursors, ALA and porphobilinogen, by repressing hepatic ALA synthase activity. 18 Many clinical studies suggest that acute attacks respond favourably to haem arginate,12,18,19 though the only placebo controlled double blind trial (involving 12 patients) gave a statistically insignificant result. 20 Early treatment with haem arginate is associated with significantly improved outcome.19,21
Indications for haem arginate in acute porphyria include severe or prolonged pain, persistent vomiting, hyponatraemia, convulsions, psychosis or neuropathy. See Appendix A for details of administration. Haem arginate has been administered in pregnancy and appears to be safe.22,23
Haem arginate is irritant to veins,
24
and repetitive peripheral use may lead to loss of the superficial venous system. It is therefore very important to infuse through a large vein, and to alternate arms for daily infusions. Administration advice must be followed carefully, particularly after the infusion:
After the haem arginate has run through, immediately rinse vein with 250 mL 0.9% NaCl (initially 3–4 boluses of 10 mL, then infuse remainder); Remove venous cannula.
Although there is no published evidence, these problems may be reduced by diluting haem arginate in albumin rather than in saline. The use of 20% albumin provides a 1:1 molar ratio of albumin to haem and should ensure binding of all haem molecules, since each molecule of albumin has a single high affinity haem binding site.
25
Analgesia
Analgesia should be given as soon as possible. Seek support from a pain team where available. Patients with severe attacks require opiates to control their pain, and analgesic requirements are typically high. Morphine, diamorphine and fentanyl are safe, but pethidine should be avoided in this situation, as metabolites may be associated with seizures. Consider use of a Patient Controlled Analgesia (PCA) pump to deliver an intravenous opiate with a prophylactic antiemetic. Opiates should be replaced by less addictive analgesics as early as possible and should not be dispensed after discharge from hospital.
Other medication
All drugs given to the patient should be checked for their safety in acute porphyrias. The Welsh Medicines Information Service provides advice and a list of safe drugs:
website: www.wmic.wales.nhs.uk/porphyria_info.php
Tel: 0044 (0)29 2074 3877 or 2074 2251
Email: Nausea and vomiting can be treated with prochloperazine, promazine or ondansetron; Severe agitation and anxiety can be treated with chlorpromazine; Hypertension and tachycardia may be cautiously treated with atenolol, propranolol or labetalol (but monitor for hypotension and bradycardia); Convulsions can be terminated with intravenous diazepam, clonazepam or magnesium sulphate. Although safety of diazepam is controversial, benefit outweighs risk when used in this acute situation. However safer anxiolytics should be prescribed for ongoing use.
Carbohydrate administration
Carbohydrate loading was the standard treatment for an acute attack prior to the availability of haem arginate. Glucose has a repressive effect on ALA synthase through effects on peroxisome proliferator-activated receptor gamma coactivator 1-alpha. 26
Mild attacks (mild pain, no vomiting, no paralysis, no hyponatraemia) may be aborted by increasing oral carbohydrate intake with the use of glucose containing drinks and high-energy foods.
Intravenous glucose in water solutions, such as dextrose 5% or 10%, should be avoided as they may aggravate hyponatraemia. 27 Intravenous glucose has no role in the treatment of an acute attack once treatment with haem arginate has commenced.
As with any acutely ill hospitalized patient, all aspects of nutrition require assessment and appropriate intervention, with advice from the Nutrition Support Team
Fluid balance
Monitor fluid balance. Intravenous fluid replacement with 0.9% sodium chloride may be required to correct dehydration or electrolyte imbalance. Hyponatraemia commonly occurs (up to 40%) 1 and while it has been attributed in some reports to the syndrome of inappropriate antidiuresis, there may also be elements of renal and/or gastrointestinal sodium loss. 12 Therefore the cause should be carefully evaluated in each case, with particular attention paid to intravascular volume status. Chronic hyponatraemia (developing over more than 48 h) should be corrected slowly (less than 6 mmol/L in 24 h) to minimize the risk of central pontine myelinolysis.
Cardiovascular function
Pulse and blood pressure should be checked at least four hourly. An electrocardiogram monitor should be used to check for arrhythmias in patients with a tachycardia.
Respiratory function
Monitor respiratory rate, vital capacity, and blood gases in severe attacks. Evidence of respiratory insufficiency requires immediate transfer to an Intensive Care Unit so that respiratory support (intubation and positive pressure ventilation) can be provided if needed.
Neurological function
Monitor for signs of neuropathy, including muscle strength, bladder and bowel function.
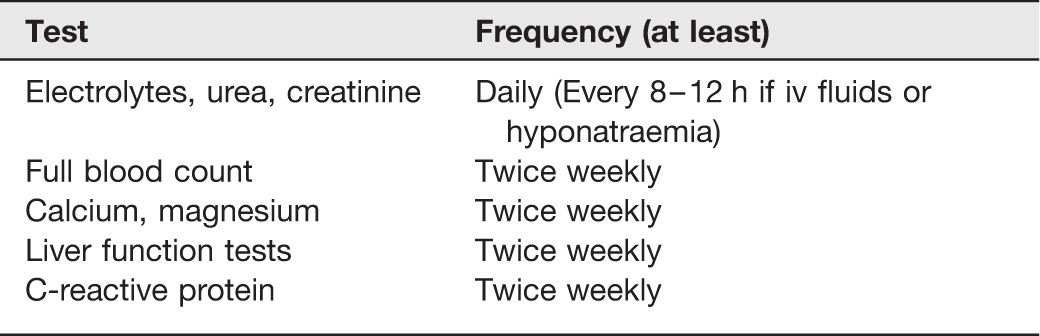
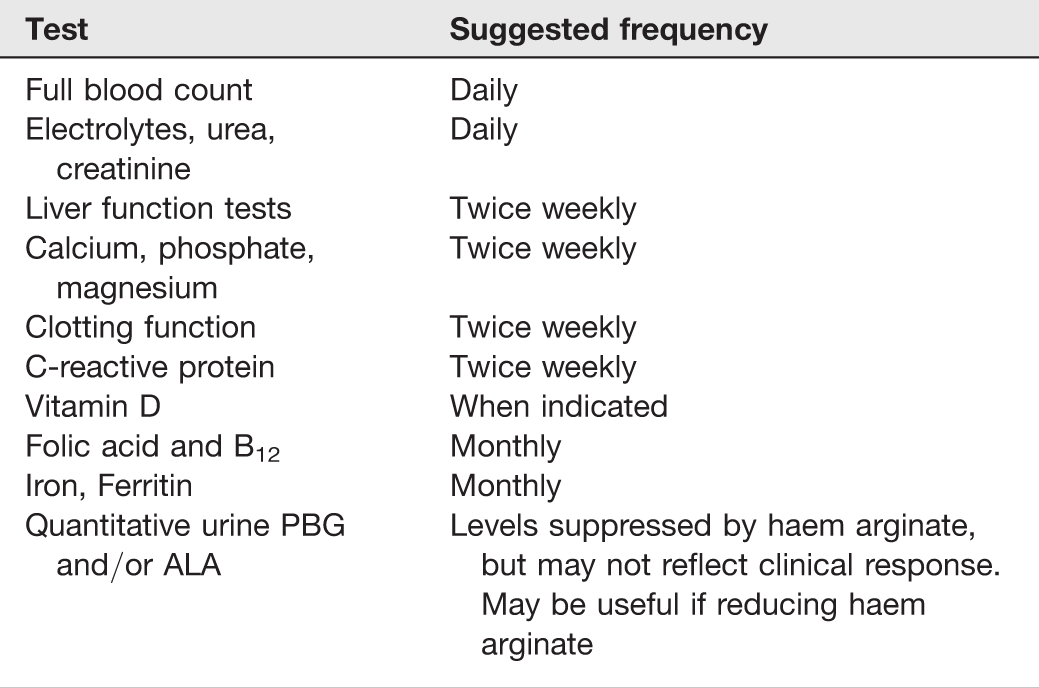
These tests are recommended to support ongoing clinical assessment for signs of deterioration.
Acute attacks complicated by progressive neuropathy
Severe attacks with neuropathy are almost always a consequence of delayed diagnosis and/or delayed treatment.11,21 Neuropathy usually develops in the context of pre-existing abdominal pain, and other clinical features of a severe acute attack. A symmetrical motor neuropathy with weakness beginning proximally in the upper limbs is typical. Focal neuropathy can also occur, and may involve cranial nerves. Neuropathy may progress rapidly to give complete paralysis, incontinence or urinary retention, swallowing difficulties and respiratory failure. Sensory neuropathy is less common but may manifest as distal, neuropathic pain and paraesthesiae or hypoaesthesia. 28 Progressive neuropathy is a medical emergency, and care of such patients must initially take place in a High Dependency or Intensive Care Unit, with access to specialist Metabolic and Neurology advice. Management should involve a multidisciplinary approach with monitoring of all organ systems and appropriate support. Infections are the main complication in critically ill patients and should be treated promptly and aggressively. Care can be transferred to general Neurology or Rehabilitation services after the acute attack has subsided, provided the patient does not require respiratory support.
Human haemin
Patients with neuropathy must be treated with haem arginate as soon as possible. Although haem arginate will not reverse an established neuropathy, it will prevent further neuronal damage. In a severely ill patient, courses of haem arginate longer than four days may be indicated, although there is no good evidence that this improves outcome. Longer courses should be considered in patients with advanced neurological damage with the aim of suppressing progression. The optimum dose, frequency and duration are uncertain, but treatment periods as long as three months have been undertaken occasionally. A daily infusion at 3 mg/kg is advisable initially, with gradual reduction of either the dose or frequency of infusions as the patient recovers. Relapse is likely on stopping long-term haem arginate, and patients may need a maintenance dose, for instance a weekly haem arginate infusion, until a clinically stable state is achieved.
Respiratory support
Artificial ventilation may be necessary for several months if respiratory failure has occurred.
Physiotherapy and occupational therapy
Recovery from neuropathy occurs slowly and may be incomplete. Intensive physiotherapy should be started as soon as possible to optimize recovery of function. Even advanced paralysis is potentially reversible though it may require months of rehabilitation. At a later date, occupational therapy is important to help the patient achieve independence and minimize long-term disability.
Neuropathic pain
Gabapentin and opiate patches may be useful to control neuropathic pain during recovery.
Safe medication
In the setting of an Intensive Care Unit with many staff from different disciplines involved in patient care, it is particularly important to check all medication for safety in acute porphyria. Prescription of an unsafe drug in a patient who is already seriously ill with an acute attack must be avoided. Clear reminders both above the patient's bed and attached to the drug chart, as well as a suitable wrist-band are useful.
Nutritional support
Good nutrition by enteral or parenteral routes is essential to prevent catabolism and reduce the risk of further attacks. Specialist Dietetic and Nutrition Support Team advice should be sought to devise and implement an individual nutritional plan. Formal nutritional assessment (including anthropometric data) and review of the plan should take place at least weekly. Regular biochemical and haematological monitoring is recommended to detect organ dysfunction, sepsis, electrolyte derangement, haematinic, vitamin D and other micronutrient deficiency (see table below for suggested frequency). Additional monitoring of electrolytes, micronutrients, glucose and triglycerides will be required if enteral or parenteral nutrition is required.
Psychiatric support
Many patients are young adults who have previously led healthy and fulfilling lives. Psychiatric problems including depression are common and should be managed appropriately. Note that fluoxetine is safe in acute porphyria, but tricyclic antidepressants are not safe. Patients may also benefit from referral to a Clinical Psychologist for counselling and support.
Monitoring in severe attacks with prolonged hospital admission
Management of recurrent acute attacks
A minority of patients have recurrent acute attacks of porphyria. In women, attacks may be related to the menstrual cycle, especially during the luteal phase.
General measures and avoidance of precipitating factors
Patients should be educated regarding precipitating factors. Regular meals, and avoidance of smoking, alcohol and drugs that can induce attacks, are all relevant. Symptomatic treatment of nausea and loss of appetite is important to help ensure an adequate diet. Patients should be given a letter or other document giving details of their condition and recommended treatment. They should be given information about appropriate support groups such as the British Porphyria Association (
Gonadotrophin-releasing hormone (GnRH) analogues
In women with recurrent premenstrual attacks of porphyria, GnRH analogues can be administered to prevent ovulation. A number of preparations are available (busrelin, goserelin, histrelin, leuprorelin or triptorelin) and published studies have reported use of differing regimens, sometimes in extremely low doses.29,30 As an example, Zoladex 3.6 (containing goserelin acetate 3.6 mg) a long acting analogue of GnRH, can be given as an implant by subcutaneous injection into the anterior abdominal wall every 28 days, with the first injection being given during the first few days of the menstrual cycle. NOTE Administration of GnRH analogues may induce a hormone surge that can trigger an acute attack. Side-effects include depression, hot flushes, reduced libido, osteoporosis and other menopausal symptoms. These can be reduced by use of a low dose oestrogen patch. Pretreatment assessment of skeletal health (including bone mineral density [BMD] determination) should be arranged with regular gynaecology review and annual BMD while treatment continues. Treatment with GnRH analogues should be reviewed after one year.
Prophylactic haem arginate
Haem arginate is not licensed as a preventive treatment, but it has been useful in some patients in whom quality of life is severely impaired by frequent, recurrent attacks that are unresponsive to the above measures. Problems include complications related to venous access devices, iron overload associated with long-term use (which can be managed with venesection) and difficulty withdrawing treatment. The decision to commence regular haem arginate should be made only by specialist metabolic centres with experience in this therapy and facilities for follow-up and monitoring. Administration through a central line is preferable. This should be inserted and managed by clinical staff with experience in the field of vascular access. Prophylactic haem arginate should be given at the lowest possible frequency that is effective. In patients with premenstrual attacks, one infusion of haem arginate (or two infusions on consecutive days) at an appropriate point in the second half of the cycle may be sufficient. Home therapy supervised by one of the homecare nursing companies may be possible for some patients, and will minimize disruption to daily life. 31
Liver transplantation
Liver transplantation has been undertaken in 10 AIP patients in the UK and Ireland and is curative, resulting in biochemical and clinical remission.32,33 Indications include: intractable acute attacks not responsive to medical treatment, recurrent acute attacks severely affecting quality of life, repeated severe life-threatening acute attacks leading to prolonged ventilation, lack of venous access for haem arginate treatment. Morbidity and mortality after transplantation is dependent on the level of preoperative complications and organ damage (paralysis, contractures, technical difficulty due to large vein thromboses).
Further advice and expert services
From 1 April 2012 a National Acute Porphyria Service has been commissioned for patients living in England. The service is provided by three main centres in Cardiff, Cambridge and London (Kings College Hospital), with additional outreach centres in Salford and Leeds. The aim is to provide clinical advice and haem arginate where appropriate, for patients with one-off acute attacks or with recurrent attacks of porphyria. The service can be contacted 24 h a day and seven days a week by telephoning the University Hospital of Wales (Tel: 029 2074 7747).
The British and Irish Porphyria Network (BIPNET;
The EPNET website (
Footnotes
DECLARATIONS
The guidelines have been reviewed by the following stakeholders: John Chamberlayne (Chair) and committee members of the patients’ support group, the British Porphyria Association. Dr Peter Galloway and members of the Metabolic Diseases subgroup of the Association for Clinical Biochemistry Clinical Practice Section.
Appendix A
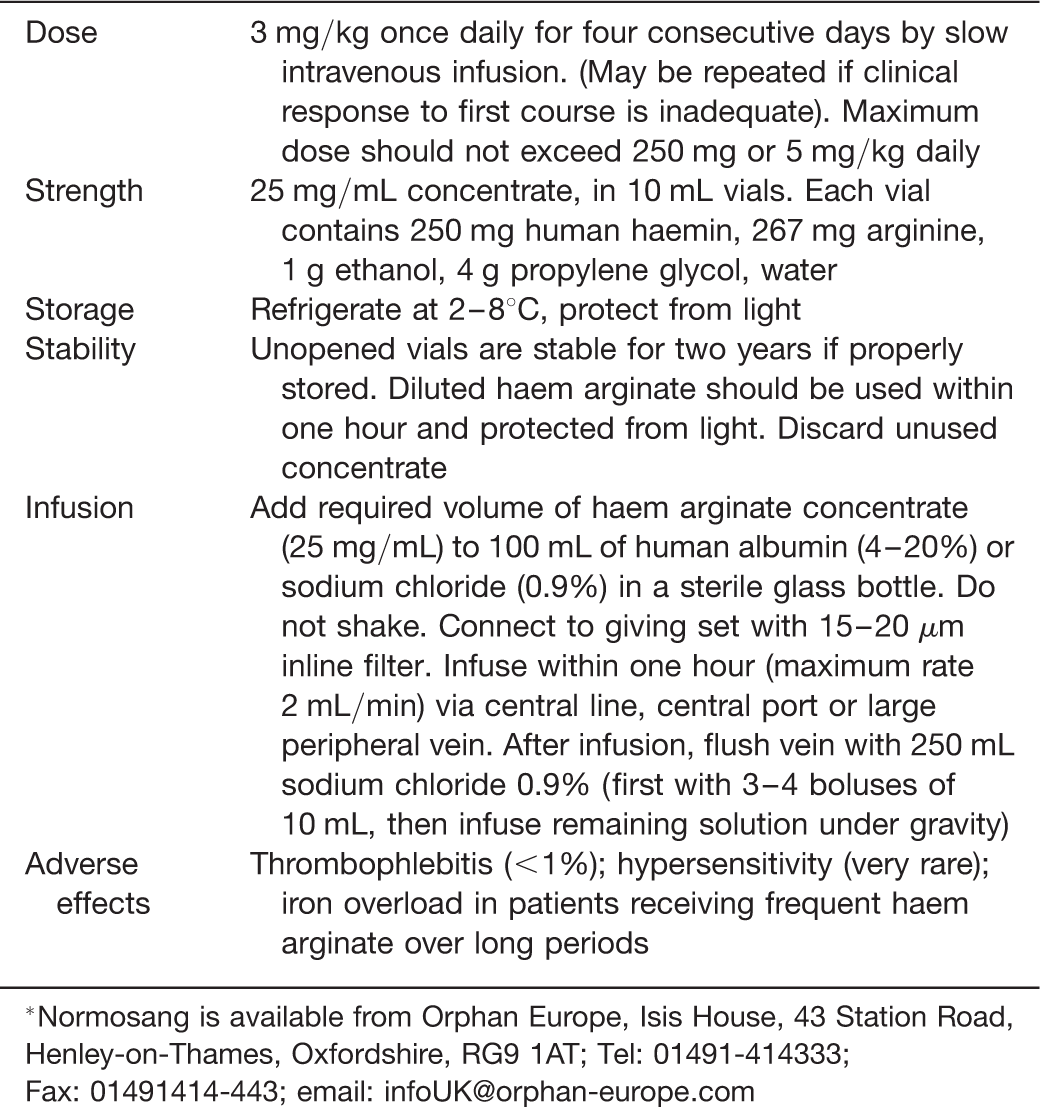
Haem arginate (Normosang*) *Normosang is available from Orphan Europe, Isis House, 43 Station Road, Henley-on-Thames, Oxfordshire, RG9 1AT; Tel: 01491-414333; Fax: 01491414-443; email:
Dose
3 mg/kg once daily for four consecutive days by slow intravenous infusion. (May be repeated if clinical response to first course is inadequate). Maximum dose should not exceed 250 mg or 5 mg/kg daily
Strength
25 mg/mL concentrate, in 10 mL vials. Each vial contains 250 mg human haemin, 267 mg arginine, 1 g ethanol, 4 g propylene glycol, water
Storage
Refrigerate at 2–8℃, protect from light
Stability
Unopened vials are stable for two years if properly stored. Diluted haem arginate should be used within one hour and protected from light. Discard unused concentrate
Infusion
Add required volume of haem arginate concentrate (25 mg/mL) to 100 mL of human albumin (4–20%) or sodium chloride (0.9%) in a sterile glass bottle. Do not shake. Connect to giving set with 15–20 μm inline filter. Infuse within one hour (maximum rate 2 mL/min) via central line, central port or large peripheral vein. After infusion, flush vein with 250 mL sodium chloride 0.9% (first with 3–4 boluses of 10 mL, then infuse remaining solution under gravity)
Adverse effects
Thrombophlebitis (<1%); hypersensitivity (very rare); iron overload in patients receiving frequent haem arginate over long periods