
Abstract
Objective:
Spontaneous cerebrospinal fluid (CSF) rhinorrhea is commonly misdiagnosed due to overlapping symptomatology with other sinonasal diseases, thus leading to delay in diagnosis and increased risk of meningitis. The objective of this study was to examine the risk factors for the initial misdiagnosis of spontaneous CSF rhinorrhea.
Methods:
A single-institutional retrospective chart review of patients with spontaneous CSF rhinorrhea was performed. Patient characteristics, initial diagnosing provider specialty, and accuracy of radiology reports were compared between subjects initially diagnosed correctly versus those that were not.
Results:
Fifty-seven patients with spontaneous CSF rhinorrhea were included with 61% being initially misdiagnosed with rhinitis, sinusitis, or migraines. Being initially seen by a non-otolaryngology provider was significantly associated with being misdiagnosed (misdiagnosis rate 83%, P < .001, Cramer’s V = 0.49). Otolaryngologists had a misdiagnosis rate of 36%. Only 32% of radiology reports correctly identified the skull base defect prior to a positive beta-2 transferrin. However, once the diagnosis of a CSF leak was established, subsequent reads by radiologists were more likely to identify the skull base defect (P < .001). Multivariable logistic regression revealed that initial visit to a non-otolaryngology provider increased the odds of misdiagnosis after adjusting for relevant confounders (P = .035).
Conclusions:
Spontaneous CSF rhinorrhea is commonly initially misdiagnosed by both non-otolaryngology and otolaryngology providers. Moreover, the skull base defect on radiographic imaging is frequently missed by radiologists when the official diagnosis is not established. Further education for all providers on the proper differential diagnosis of sinonasal symptomatology is warranted to expedite the diagnosis of spontaneous CSF rhinorrhea.
Keywords
Introduction
Cerebrospinal fluid (CSF) rhinorrhea can be challenging to diagnose. This is attributed to multiple factors, including symptomatology overlapping with other sinonasal diseases combined with potential subtle findings on radiographic imaging. Recognizing this condition may be especially difficult in the setting of spontaneous CSF rhinorrhea, where the skull base defect is often small and a common identifiable risk factor, such as a history of trauma, is absent. 1 A recent study investigating 22-item sinonasal outcome test (SNOT-22) scores in spontaneous CSF rhinorrhea revealed that 48% of spontaneous CSF rhinorrhea patients were initially misdiagnosed with chronic rhinosinusitis (CRS). 2 However, unlike CRS, misdiagnosing spontaneous CSF rhinorrhea can have potentially fatal consequences, such as meningitis. 1 Thus, timely diagnosis is critical to prevent morbidity and mortality.1,3,4 While previous studies have investigated the misdiagnosis rate of spontaneous CSF rhinorrhea,2,5 none have evaluated the specific risk factors contributing to a missed diagnosis nor the accuracy of radiographic assessment. Therefore, the objective of this study was to examine the specific risk factors resulting in the initial misdiagnosis of spontaneous CSF rhinorrhea with a goal of improving clinical accuracy amongst providers.
Materials and Methods
Study Design and Patients
A single-institutional study was performed at the University of Texas Health San Antonio. This study was reviewed by the institutional review board and determined to be exempt. A retrospective chart review (2014-2024) was conducted for patients diagnosed with spontaneous CSF rhinorrhea. Inclusion criteria included: (1) adult patients (≥ 18 years old) and (2) confirmed diagnosis of spontaneous CSF rhinorrhea with a beta-2-transferrin. Patients with CSF rhinorrhea due to iatrogenic, traumatic, neoplastic, or congenital (non-spontaneous) etiologies were excluded. Patient demographics, medical and surgical history, symptomatology, initial diagnosing provider specialty, accuracy of initial diagnosis, accuracy of radiographic reports, and location of the skull base defect were collected for all patients.
Statistical Methods
Continuous variables were reported as means and standard deviations while categorical variables were reported as counts with percentages. Differences in continuous variables between patients that were initially misdiagnosed versus those that were correctly diagnosed were compared using the t-test. Chi-square test, Fishers exact test, and McNemar’s test were used for differences in categorical variables. Cramer’s V was reported for effect size where relevant. Multiple logistic regression was performed to evaluate the association between the initial misdiagnosis of spontaneous CSF rhinorrhea and the initial diagnosing provider specialty while controlling for potential confounders, including pertinent demographic characteristics, medical history, surgical history, and symptomatology. Odds ratios and 95% confidence intervals were reported. Alpha was set to .05 to determine statistical significance. All statistical analyses were performed using Stata 18.0 (Stata LLC, College Station, TX).
Results
Fifty-seven patients with spontaneous CSF rhinorrhea were included with 61% initially misdiagnosed with rhinitis (46%), sinusitis (51%), or migraines (3%; Table 1). Being initially seen by a non-otolaryngology provider was significantly associated with being misdiagnosed (P < .001; Cramer’s V = 0.49; Table 2). Non-otolaryngology providers in this study included emergency department (n = 3), neurosurgery (n = 3), and primary care (n = 24) providers with a misdiagnosis rate of 100%, 0%, and 92%, respectively. Only 32% of radiology reports correctly identified the skull base defect prior to a positive beta-2 transferrin. However, once the diagnosis of a CSF leak was established, radiologists were more likely to identify the skull base defect (P < .001). No difference was observed in terms of patient demographic characteristics, presenting signs/symptoms, duration of symptoms, medical/surgical history, and location of skull base defect between subjects that were initially misdiagnosed and those that were not. Overall, non-otolaryngology providers initially misdiagnosed spontaneous CSF rhinorrhea about 83% of the time while otolaryngology providers had an initial misdiagnosis rate of 36%. Of the 9 patients that were initially misdiagnosed by an otolaryngologist, 6 of the patients had a body mass index ≥30 and were female. Additionally, medical history (sinusitis, rhinitis, obstructive sleep apnea, and meningitis) and having a nondiagnostic radiology report prior to a beta-2 transferrin were not associated with the ability of otolaryngologists to correctly diagnose spontaneous CSF rhinorrhea. However, patients that were initially misdiagnosed by an otolaryngologist were more likely to have undergone a previous sinonasal surgery (P = .037; Cramer’s V = 0.49). Multiple logistic regression revealed that being seen by a non-otolaryngology provider increased the odds of initial misdiagnosis after adjusting for relevant confounders (P = .035; Figure 1).
Sample Characteristics of Study Participants.
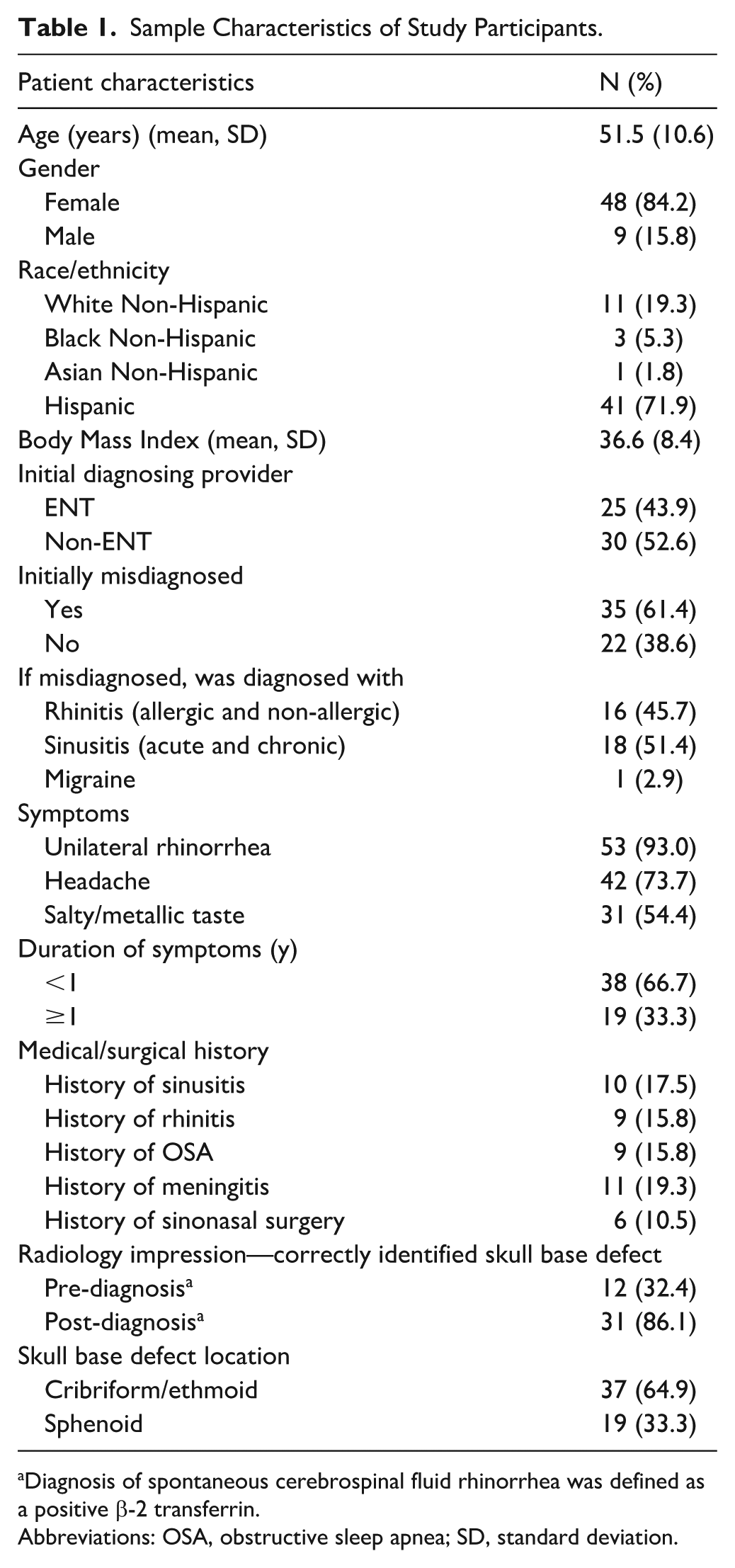
Diagnosis of spontaneous cerebrospinal fluid rhinorrhea was defined as a positive β-2 transferrin.
Abbreviations: OSA, obstructive sleep apnea; SD, standard deviation.
Bivariate Analysis of Initial Misdiagnosis of Spontaneous CSF Rhinorrhea by Demographics, Medical and Surgical History, Imaging, and Pathology Characteristics.
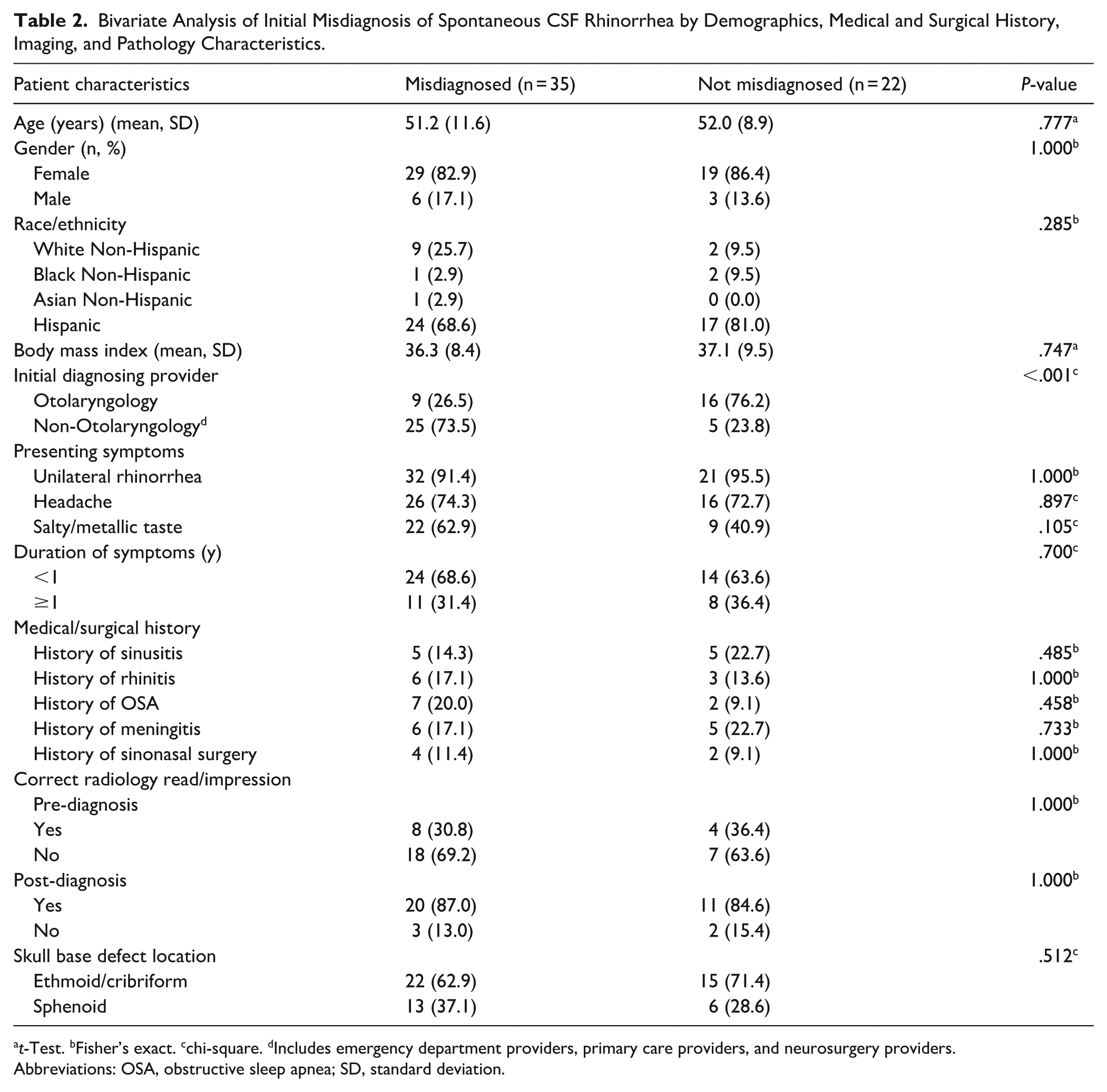
t-Test. bFisher’s exact. cchi-square. dIncludes emergency department providers, primary care providers, and neurosurgery providers.
Abbreviations: OSA, obstructive sleep apnea; SD, standard deviation.
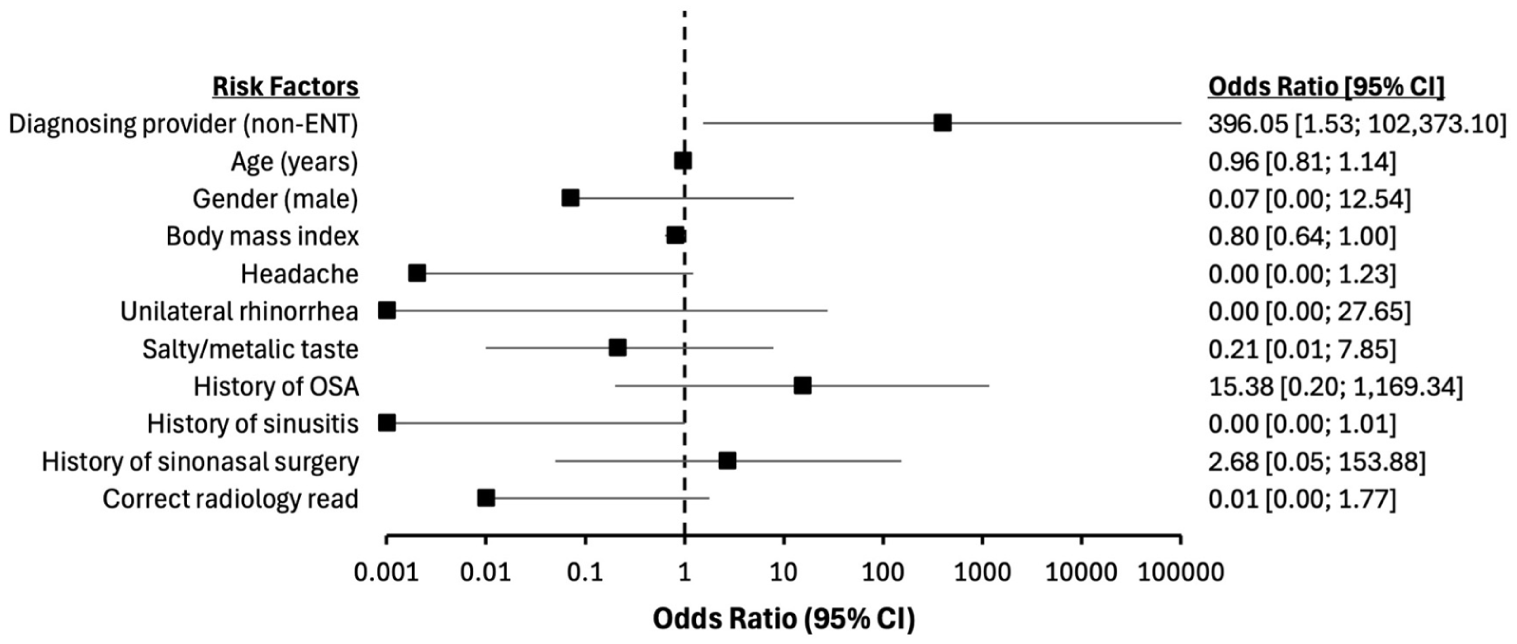
Forest plot displaying results of multiple logistic regression evaluating the relationship between the misdiagnosis of spontaneous CSF rhinorrhea and the initial diagnosing provider specialty while controlling for relevant confounders, including demographics, medical history, and symptomatology. Being a non-otolaryngology provider was used as the main risk factor of interest while being an otolaryngology provider was used as the reference. All odds ratios are adjusted for all other covariates in the model.
Discussion
According to the “International Consensus Statement: Spontaneous Cerebrospinal Fluid Rhinorrhea,” spontaneous CSF rhinorrhea should be suspected in female, obese patients with unilateral watery rhinorrhea that is triggered by changes in posture. 3 Additionally, idiopathic intracranial hypertension (IIH) has been associated with spontaneous CSF rhinorrhea, therefore asking about symptoms suggestive of IIH, including headache, visual changes, and pulsatile tinnitus, are important. 3 However, even in the presence of the classic symptoms set forth by the International Consensus Statement on spontaneous CSF rhinorrhea, providers may still fail to recognize CSF rhinorrhea and instead give an erroneous diagnosis of sinusitis or rhinitis, especially if knowledge of this pathology is limited.
As evidenced by the results of this study, presenting symptoms and the classic patient demographic for spontaneous CSF rhinorrhea (ie, females with higher body mass index) did not aid in correctly identifying CSF rhinorrhea. Instead, the provider’s specialty, which is a measure of exposure to and familiarity with CSF rhinorrhea pathology, was significantly associated with making the correct diagnosis. This study found that non-otolaryngology providers, especially primary care providers, more commonly initially misdiagnosed spontaneous CSF rhinorrhea, most likely due to the lower frequency of this sinonasal pathology. Additionally, radiologists failed to identify the presence of a skull base defect in 68% of cases. This error in radiographic accuracy further compounds the difficulty in correctly identifying a CSF leak by the ordering physician, especially those that are less familiar with interpreting sinonasal imaging themselves (ie, primary care physicians) and must rely on the radiologist’s expertise. However, even otolaryngology providers failed to correctly identify spontaneous CSF rhinorrhea about 36% of the time. Further investigation of those that were initially seen by an otolaryngologist revealed that patient demographics, comorbid sinonasal conditions, and the accuracy of radiology reads did not impact the misdiagnosis rate among otolaryngologists. However, patients that initially saw an otolaryngologist were more likely to have undergone a previous sinonasal surgery, which may have complicated the clinical picture and made diagnosis more challenging. A possibility exists that these patients may have had undergone incorrect sinonasal surgeries and procedures based on the wrong diagnosis. Notably, the limitations of a retrospective study prevent demonstrating the temporality of such incidence.
Maintaining some level of suspicion and always having CSF rhinorrhea on the differential diagnosis for patients with rhinorrhea are crucial to avoid delayed treatment and the associated morbidity and mortality associated with CSF rhinorrhea.3,6 Thus, education of both otolaryngology and non-otolaryngology providers on the signs and symptoms of CSF rhinorrhea and its differentiation from common sinonasal complaints is needed to efficiently treat this patient population. To aid in properly evaluating a patient with rhinorrhea, Figure 2 displays a possible diagnostic algorithm that can be used by both non-otolaryngologists and otolaryngologists.
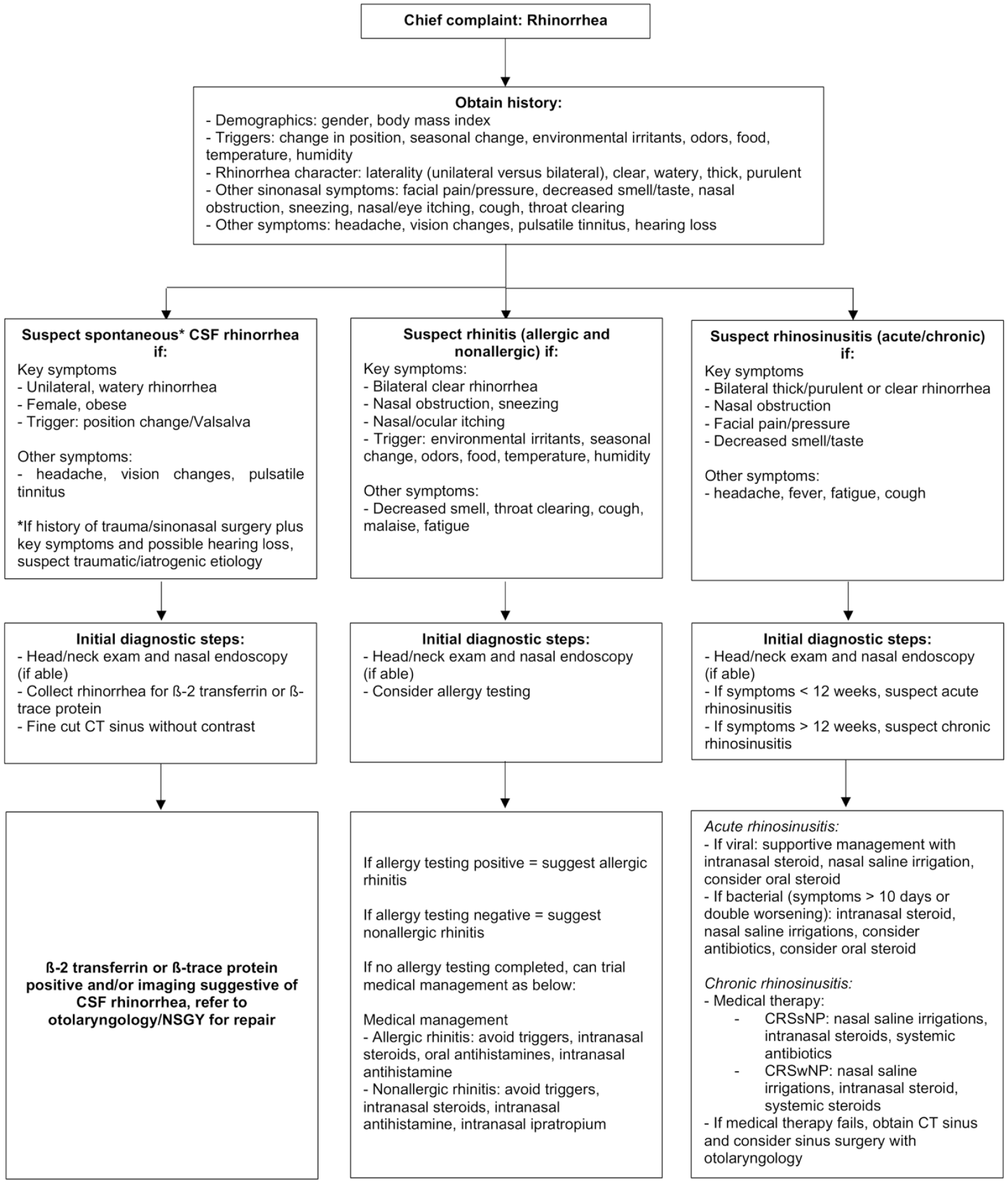
First, a detailed history is obtained, including collecting demographic information, laterality of the rhinorrhea, triggers, character of the discharge, and other associated symptoms. Second, based on the key symptoms gathered by history, suspicion for a certain sinonasal pathology can be determined. If history details a female with higher body mass index and complaining of unilateral, watery salty-tasting rhinorrhea that is triggered by changes in position and Valsalva along with possible headaches, vision changes, and pulsatile tinnitus, then spontaneous CSF rhinorrhea should be suspected. If a history of head trauma or sinonasal surgery is also present, then the provider should still suspect CSF rhinorrhea but one that is due to a traumatic or iatrogenic etiology. The next step would be to do a comprehensive head/neck exam along nasal endoscopy (if able) in addition to collecting the rhinorrhea for β-2 transferrin or β-trace protein. During physical exam, a provider can attempt to trigger the CSF leak by having the patient lean forward in a chair placing their head between their knees and Valsalva. Clear liquid discharge from 1 side of the nose can then be collected in a sterile specimen cup for β-2 transferrin or β-trace protein testing. Fine cut CT sinus should be obtained to locate the skull base defect. On the other hand, if a patient with rhinorrhea has the key symptoms of bilateral clear rhinorrhea that is associated with nasal obstruction, sneezing, nasal/ocular itching, and triggered by environmental irritants, seasonal changes, odors, food, temperature, or humidity, then rhinitis (allergic or nonallergic) should be suspected. Again, a comprehensive head and neck exam should be completed along with nasal endoscopy (if able). Allergy testing can then be considered or medical management can be trialed as described in the algorithm based on suspicion if the rhinitis is allergic or nonallergic in etiology. Finally, if a patient with rhinorrhea is also experiencing bilateral purulent or clear rhinorrhea associated with the cardinal symptoms of rhinosinusitis, then rhinosinusitis should be suspected. Workup and initial management are described in the algorithm.
Limitations of this study include: (1) the observational study design and (2) single institution. First, a retrospective review may predispose the data to certain biases, such as selection and non-response bias. Availability of data was limited by documentation in the chart, thus identifying the initial diagnosing provider was sometimes difficult. Second, although this study was limited to a single institution, the population characteristics paralleled those expected for spontaneous CSF rhinorrhea patients, including predominately middle-aged females with higher body mass index. 3
Conclusion
Spontaneous CSF rhinorrhea is commonly misdiagnosed due to the overlap in symptomatology with other sinonasal diseases. Although non-otolaryngology providers are more likely to initially make a diagnostic error, otolaryngologists fail to recognize CSF rhinorrhea at least a third of the time. Additionally, radiologists often do not identify the skull base defect on radiographic imaging when the diagnosis is not established. Education is needed for all providers (both otolaryngology and non-otolaryngology) to improve the diagnostic accuracy of spontaneous CSF rhinorrhea.
Footnotes
Acknowledgements
None.
Ethical Considerations
This study received ethical approval from the University of Texas Health San Antonio IRB (approval STUDY00000932) on September 17, 2025. This is an IRB-approved retrospective exempt study, all patient information was de-identified and patient consent was not required. Patient data will not be shared with third parties.
Consent to Participate
The Institutional Review Board of the University of Texas Health San Antonio waived the need for ethics approval and patient consent for the collection, analysis, and publication of the retrospectively obtained and anonymized data for this non-interventional study.
Consent for Publication
Not applicable.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Philip Chen is a consultant for Medtronic, advisory board for Sanofi, Amgen, and GlaxoSmithKline, speaker’s bureau for GlaxoSmithKline and Optinose, and has research funding from Aerin Medical. None affect this research.
Data Availability Statement
The datasets generated during and/or analyzed during the current study are available from the corresponding author on reasonable request.