
Abstract
Objectives:
Characterize the presentation of chronic airway obstruction for patients presenting with massive thyroid goiters.
Methods:
Demographic data acquisition was undertaken on 5 patients who presented with a compressive goiter and had pre-operative severe airway obstruction secondary to supraglottic and laryngeal edema. Each patient had a resolution of severe airway obstruction post-thyroidectomy.
Results:
In all, 5 patients were diagnosed with severe airway obstruction due to chronic obstruction by a thyroid goiter. Several airway management interventions were pursued during definitive surgery (conventional or videolaryngoscopic intubation and a hybrid endoscopic approach incorporating the Seldinger technique). Successful thyroidectomy led to rapid resolution of laryngeal edema.
Conclusion:
Venolaryngeal obstruction syndrome is proposed as a term to describe the laryngeal findings in compressive goiters. The pathophysiological sequence resulting in chronic airway obstruction may have similar mechanisms to expanding neck hematomas after thyroid surgery.
Introduction
Patients who present with massive thyroid goiters can develop watery supraglottic edema related to the chronic compression of venous and lymphatic outflow within the central visceral compartment of the neck. We postulate that this process represents a reasonable anatomic surrogate for a rapidly expanding neck hematoma, which is the most dreaded complication after thyroidectomy. 1 In the current investigation, we present specific case examples of the supraglottic edema that occurs as a consequence of laryngeal lymphatic and venous outflow obstruction stemming from compressive goiter. The term “venolaryngeal obstruction syndrome” (VLOS) is proposed to describe this predictable sequence of events that likely occurs as a chronic condition associated with compressive goiter.
Materials and Methods
A quality assurance database of endocrine surgery was interrogated after permission was sought and obtained from the Augusta University Institutional Review Board (Protocol number 611354-20). Patients were identified with massive goiters and who also manifested varying degrees of chronic airway obstruction.
A case series of 5 patients with similar presentations (between 2004 and 2020 by a single surgeon) were detected. Each of the 5 patients presented with massive goiters and an endoscopic laryngeal examination that demonstrated distorted laryngeal anatomy with watery supraglottic edema. There were 3 women and 2 men. Cross-sectional imaging revealed retropharyngeal goiter in all 5 patients; 2 patients had extensive goiter involving both the retropharyngeal and substernal spaces. Brief case histories are provided below.
Case 1
D.C. was a 68-year-old obese female with a massive multinodular goiter with substernal extension. Examination in the office revealed partially obscured vocal folds from ball-valving supraglottic edema (Figure 1a) but with full mobility. Her BMI was 31. A pre-operative neck CT revealed her goiter’s substernal and retropharyngeal extension (Figure 1b). An intubation was accomplished with the video-assisted laryngoscope. An uncomplicated total substernal thyroidectomy was performed (Figure 1c), and she had an uneventful recovery with prompt resolution of her supraglottic edema (Figure 1d). Video documentation of her larynx’s pre-operative and post-operative appearance may be found online (Video 1).
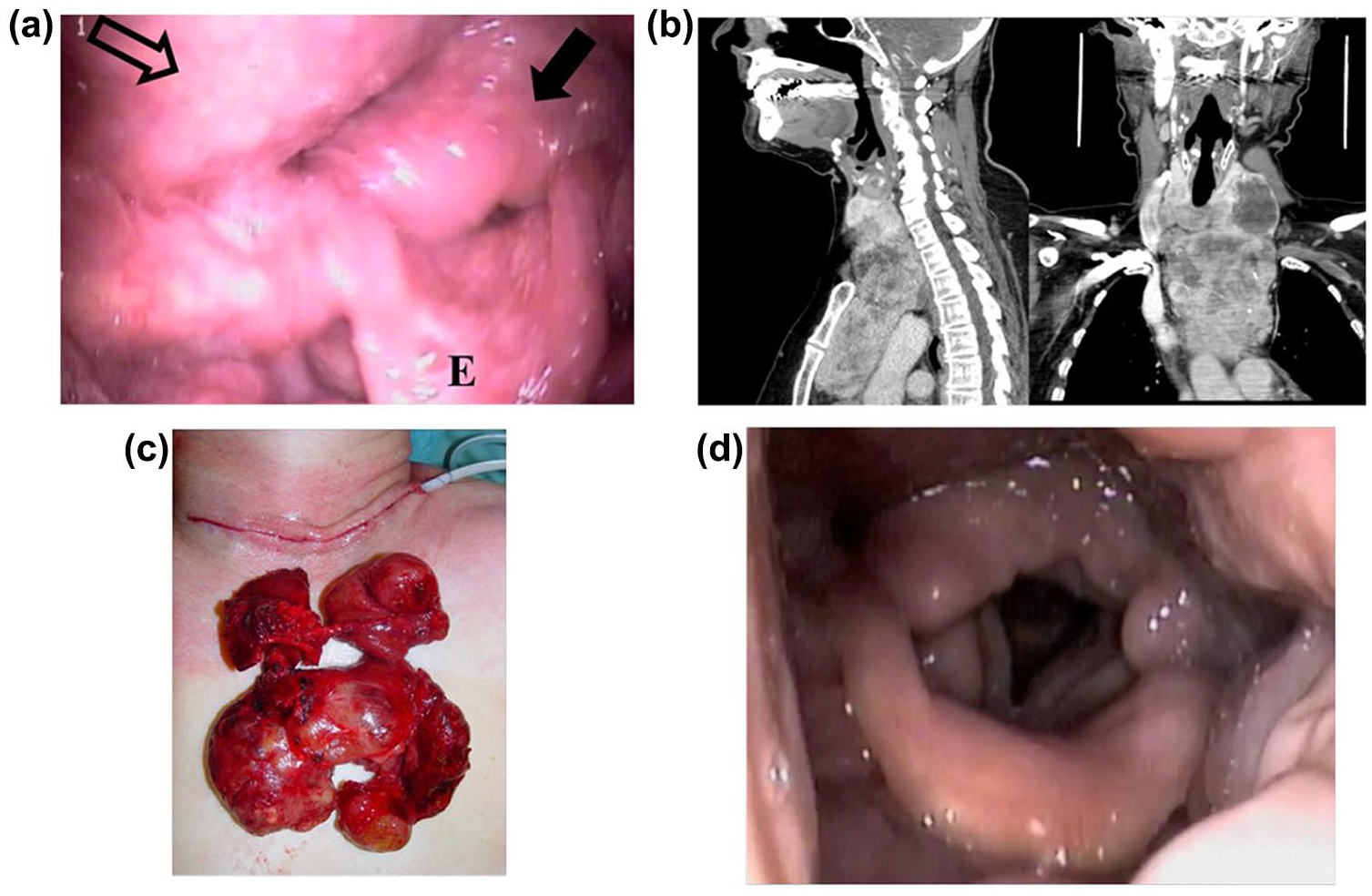
Pre-operative larynx (a) of patient with massive retropharyngeal goiter causing airway obstruction. E = epiglottis; solid arrow = supraglottic edema; open arrow = retropharyngeal compression. CT (b) confirms extent of goiter; (c) removed specimen. Post-operative examination (d) confirmed resolution of edema.
Case 2
L.M. was a 52-year-old male with a massive bilateral multinodular goiter with retropharyngeal extension who was scheduled for a total thyroidectomy at an outside hospital. Surgery was aborted because of the inability to intubate the patient despite the use of a video-assisted laryngoscope device. He was a super-morbidly obese individual (BMI 43), and he had 9-centimeter bilateral thyroid lobes and a 6-cm isthmus nodule. Endoscopic laryngeal examination revealed severely redundant tissue in the hypopharynx with supraglottic edema obscuring the anatomy (Figure 2a) and making it difficult to navigate this redundancy. CT scan revealed a massive bilateral goiter with retropharyngeal extension on the left (Figure 2b). His intubation required a multidisciplinary approach with exposure of the larynx utilizing a video-assisted laryngoscope, and with a Seldinger technique utilizing a flexible bronchoscope by the laryngology team in which the endotracheal tube was threaded through the larynx over the bronchoscope (see Video 2 online). This approach has been described previously.2,3 The surgery was accomplished uneventfully with the removal of the entire thyroid (Figure 2c). The post-operative course was unremarkable with rapid resolution of the airway edema (Figure 2d).
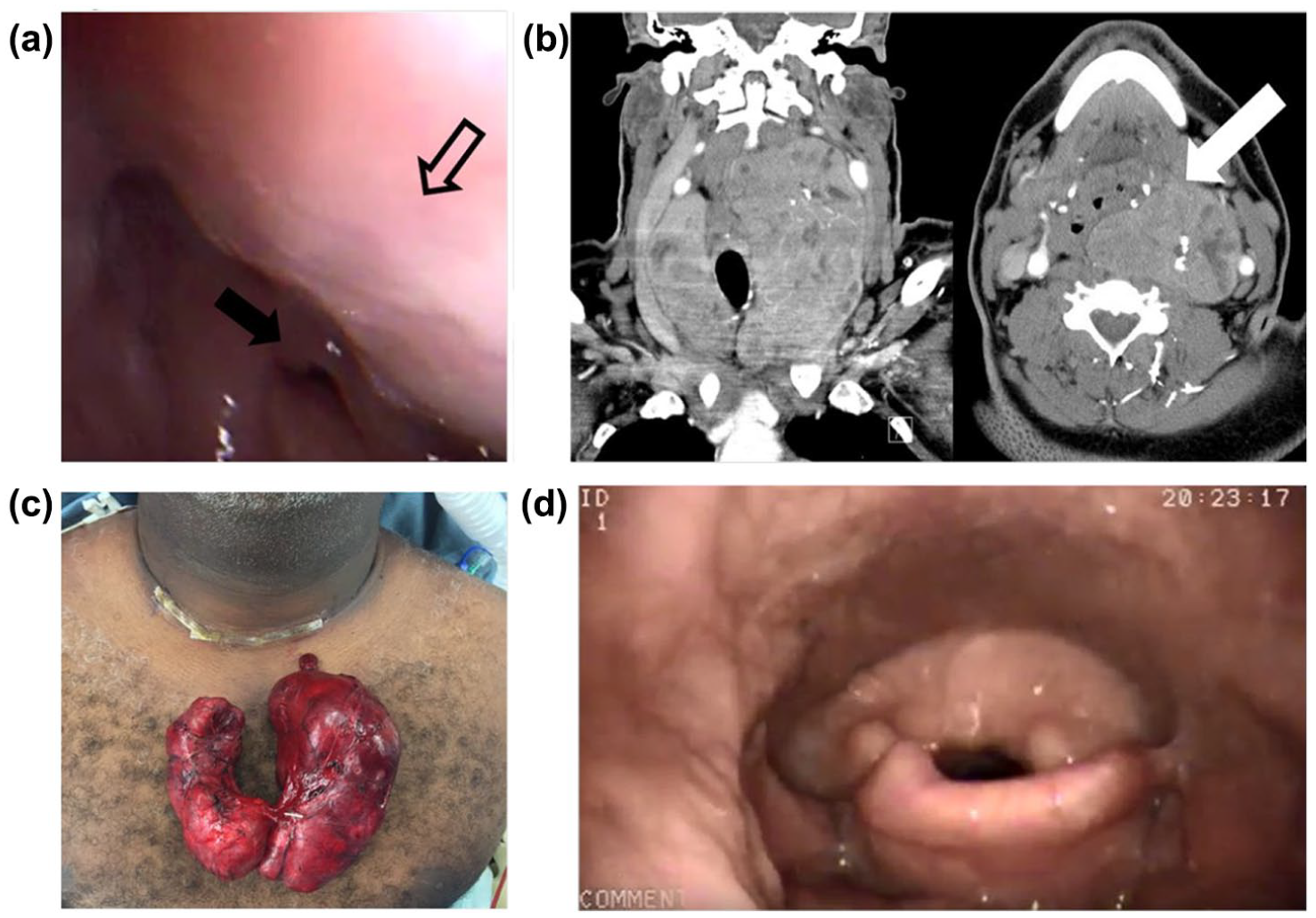
Retropharyngeal encroachment by goiter (open arrow) obscures the airway (a), and causes supraglottic edema (solid arrow). CT (b) confirms retropharyngeal extension (solid arrow). Removed specimen (c) and improved post-operative laryngeal appearance (d) are demonstrated.
Case 3
Patient K.M. was a 65-year-old morbidly obese male smoker (BMI 38) with severe oxygen-dependent COPD and obstructive sleep apnea who presented with a massive bilateral Hashimoto’s goiter. He described increasing shortness of breath, hoarseness, and dysphagia, and a positive Pemberton’s sign was elicited. Laryngeal examination revealed diffuse supraglottic edema. The vocal folds could be seen and were mobile. Tracheal compression was seen on the CT scan, revealing circumferential laryngeal compression (Figure 3a). Because the vocal folds could be visualized, a conventional intubation was undertaken. While he had rapid resolution of his supraglottic edema, he was noted to have temporary bilateral recurrent laryngeal nerve dysfunction postoperatively. Despite gradual evidence of improving laryngeal function over several weeks of observation, a temporary surgical airway was eventually obtained with a Montgomery cannula 6 weeks after his thyroidectomy. He had complete recovery of vocal function 4 months after the original surgery, and his cannula was removed.
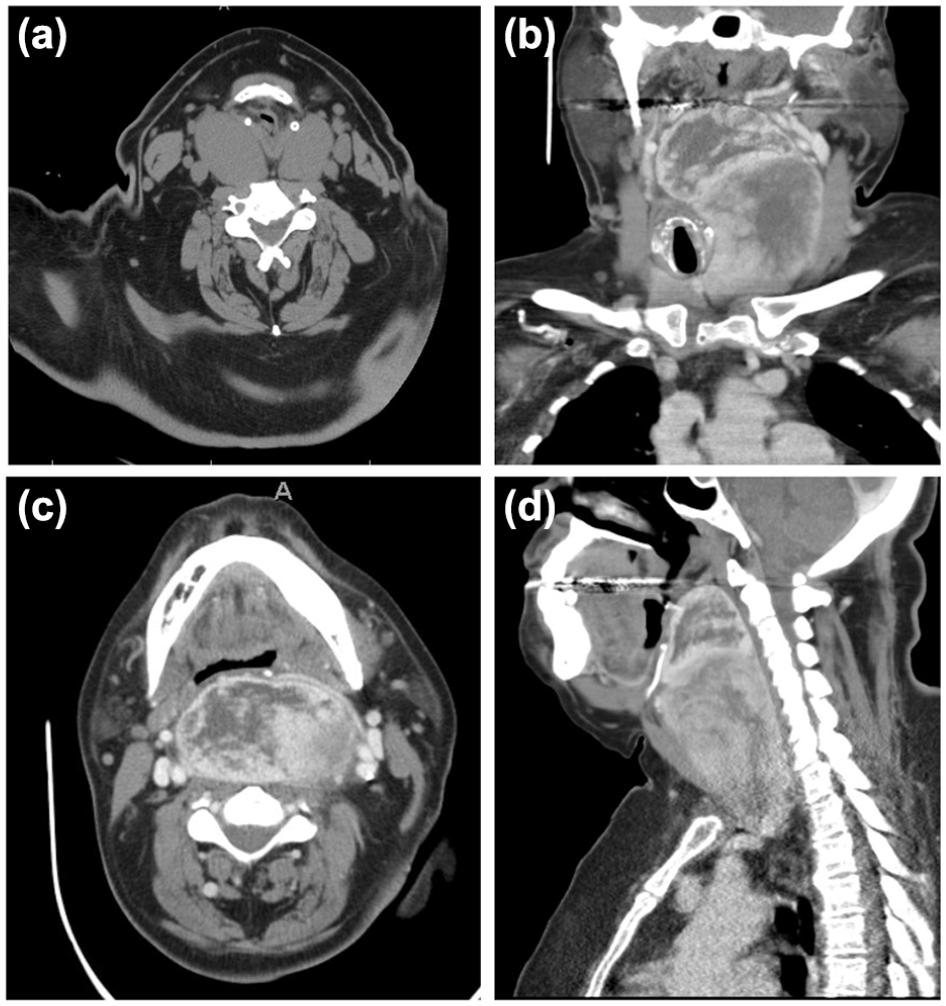
Patient KM had a large Hashimoto’s goiter which caused severe retropharyngeal compression (a) as seen on cross-sectional imaging. Patient BR with extensive retropharyngeal goiter causing chronic airway obstruction in coronal (b), axial (c), and sagittal reformatting (d).
Case 4
Patient B.R. was a 65-year-old female morbidly obese (BMI 37) who presented with a neck mass, dysphonia, and intermittent dysphagia. Examination revealed a massively enlarged left retropharyngeal thyroid goiter. Endoscopic examination demonstrated supraglottic edema with obstruction preventing a view of the vocal folds. Hypopharyngeal narrowing from goitrous compression was apparent. A CT scan (Figure 3b-d) demonstrated the posterior retropharyngeal encroachment, which caused venous and lymphatic outflow obstruction sufficient to result in airway obstruction. She was taken to surgery, intubated with a video-assisted laryngoscope, and a retropharyngeal thyroidectomy was accomplished without incident. Post-operative laryngoscopic examination revealed rapid resolution of her laryngeal swelling.
Case 5
Patient E.G. was a 61-year-old super-morbidly obese woman with a toxic multinodular goiter. She was a debilitated woman on home oxygen for more than 10 years with obstructive sleep apnea, diabetes, congestive heart failure, coronary artery disease, and respiratory acidosis who presented with a BMI of 44.4. She also endorsed symptoms of dysphagia and odynophagia from a massive multinodular goiter with substernal and retropharyngeal extension and the largest nodule exceeding 7 cm. Her examination revealed severe supraglottic edema obscuring her vocal folds. Her hyperthyroidism was managed with methimazole and beta-blockers, and she was rendered euthyroid prior to surgery. Her procedure required intubation with a video-assisted laryngoscope, which was achieved without incident. After an uneventful total thyroidectomy, repeat flexible laryngoscopy in the hospital demonstrated marked improvement in her supraglottic lymphedema and normal vocal fold mobility.
Discussion
This paper describes 5 patients with similar presentations of significant laryngeal and supraglottic edema secondary to venous and lymphatic outflow obstruction by massive goiters. All 5 patients had complete resolution of their airway symptoms following total thyroidectomy.
This clinical condition resembles venous outflow obstructions elsewhere in the body, including superior vena cava syndrome. 4 SVC syndrome results in internal jugular and upper extremity venous congestion, including the laryngeal compartment. We propose a new term, VLOS, to encompass a more specific constellation of findings found within the laryngeal area. We suggest this development of laryngeal edema exists in the context of chronically expanding thyroid goiters and rapidly expanding neck hematomas. In these cases, the small caliber superior and inferior laryngeal veins are compressed by either tumor mass effect or blood, leading to venous congestion in the central visceral space. Whether the process is acute or chronic, each scenario will lead to eventual airway compromise if the venous flow of the laryngeal veins is not re-established. The key difference in severity and acuity of presentation may relate to a patient’s ability to adapt slowly over time and compensate in the case of massive goiters.
Interestingly, only 1 out of 5 patients required advanced intubation techniques after failed intubation at an outside facility. Given the extensive supraglottic edema, more advanced techniques should always be considered in this patient population with the appropriate equipment readily available. If surgeons are performing cases of large thyroid goiters with associated VLOS, we believe it is safer to do so at a high-volume center where the anesthesia team is comfortable with advanced airway management. Furthermore, the presented findings further illustrate the importance of the pre-operative laryngeal examination. Critical information is garnered, including the movement of the true vocal cords, and the presence of VLOS or other airway anomalies in patients with compressive goiters. Examination in these cases allowed informed airway planning leading to safe and successful endotracheal intubation in all cases.
Each patient in this case series had a BMI over 30, which may be a key risk factor for developing VLOS in the context of massive thyroid goiters. Obesity is a well-known contributor to both venous congestion and lymphatic stasis. Although all patients presenting for thyroid surgery should have documentation vocal cord movement prior to surgery, patients with massive goiters and obesity should be closely evaluated in the perioperative period to facilitate safe airway management.
The case examples analyzed offer photo-documentary evidence of the supraglottic edema that causes airway compromise in patients with compressive goiter. Indirect support for the presumption of this mechanism derives from the consistently rapid resolution of edema following removal of the goiter. A similar mechanism may be responsible for the airway obstruction in neck hematoma, although demonstration of this cascade of events is difficult to capture endoscopically because of the rapid clinical deterioration that is usually present. The mechanics and consequences of acute and chronic airway obstruction for hematomas and goiters may be similar: pressure in the laryngeal compartment exceeds the venous and lymphatic pressures, reducing outflow from the larynx, leading to supraglottic laryngeal edema. In the cases of chronic obstruction by goiters, release of the pressure by total thyroidectomy results in complete resolution of edema. This understanding reinforces the principle that in the patient with acute VLOS from expanding neck hematoma, the most important initial maneuver in addressing the airway obstruction is to decompress the thyroid compartment rapidly decompress the thyroid compartment. 5 Jean Francois Henry and his team have previously speculated about the mechanism of airway obstruction in rapidly expanding hematomas, stating that “impairment in venous and lymphatic drainage with resultant laryngopharyngeal edema may place the patient’s airway at significant risk.” 6 We have previously urged that thyroid surgeons abandon the closure of strap muscles that are still commonly performed after thyroidectomy. 7 Strap muscle closure allows the thyroid compartment pressures to rise in the face of post-operative bleeding; leaving the strap muscles open essentially eliminates the potential for acute VLOS.
The limitations of this study and ability to draw conclusions are restricted by it being a case series. The proposed anatomic basis for airway obstruction in patients with expanding neck hematoma or compressive goiter cannot easily be tested with conventional scientific methods. Other reasonable factors to evaluate are age, peripheral vascular or cardiovascular disease history, and smoking history. We plan to evaluate this in future research efforts by examining a large cohort of patients with retrosternal goiters, but multi-institutional studies may be needed to reach reliable conclusions due to the relatively low incidence of VLOS.
In summary, we present 5 patients with massive thyroid goiters presented with significant airway obstruction. Total thyroidectomy resulted in the complete resolution of symptoms for all 5 patients. Airway obstruction in the context of chronically enlarged thyroid goiters may appropriately be labeled VLOS, reflecting the pathophysiological basis for this condition.
Footnotes
Acknowledgements
There are no further acknowledgments.
Author’s Note
Evan C. Compton is also now affiliated to Section of Otolaryngology-Head and Neck Surgery, University of Calgary, Calgary, Alberta, Canada
Data Availability Statement
The data that supports this paper is available upon request from the authors.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethics Approval Statement
A prospectively maintained quality assurance database of endocrine surgery was interrogated after permission was sought and obtained from the Augusta University Institutional Review Board (Protocol number 611354-20).
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.