
Abstract
Objectives:
Allergic fungal rhinosinusitis (AFRS) often results in expansion of disease beyond the paranasal sinuses, which may put important structures, such as the anterior ethmoid artery (AEA) or lateral lamella of the cribiform, at risk of injury during endoscopic sinus surgery (ESS). This study aims to compare the AEA to skull base (AEA-SB) length in patients with AFRS versus chronic rhinosinusitis with nasal polyps (CRSwNP), as well as additional anatomic variants.
Methods:
A single institutional retrospective chart review of patients undergoing ESS for AFRS and CRSwNP was performed. AEA-SB length were compared between the 2 groups. Other anatomic variants, including Keros measurement and presence of supraorbital ethmoid air cells (SOEC), concha bullosa (CB), sphenoethmoidal, and infraorbital ethmoid cells were measured and compared between the 2 groups.
Results:
Twenty-one patients were included in each cohort. The AFRS group was younger in age (P = .015) and had a significantly longer AEA-SB length (P = .014) compared to the CRSwNP group. No significant differences were observed between the 2 groups regarding Keros measurement, presence of concha bullosa, infraorbital ethmoid, sphenoethmoidal, or SOEC. No association was seen between AEA-SB length and Keros class in either group.
Conclusions:
AFRS harbors anatomical differences when compared to CRSwNP, with the former associated with a longer AEA-SB length. This key difference should be considered in preoperative planning to prevent injury to the AEA in patients undergoing ESS for AFRS.
Keywords
Introduction
Allergic fungal rhinosinusitis (AFRS) commonly presents with symptoms similar to undifferentiated chronic rhinosinusitis with nasal polyps (CRSwNP). Yet, AFRS can cause characteristic chronic expansion and demineralization of the paranasal sinuses and skull base. In severe cases, it has resulted in complications such as vision change, spread of intracranial infection, and craniofacial deformity. Combined with the need for meticulous surgery, these anatomic changes pose important considerations for the endoscopic sinus surgeon.1 -4 The complications of endoscopic sinus surgery (ESS) have been well documented. However, literature is lacking on AFRS specific complications and associated preoperative planning and avoidance.2,4
Traditional operative management of AFRS is thorough endoscopic sinus surgery with potential operative complications, including orbital hematoma, skull base injury and resultant cerebrospinal fluid leak.5 -7 Use of preoperative imaging to define variations in anatomic landmarks, including the Keros measurement and a defined “low” skull base, is shown to correlate with AFRS surgical complications.7,8 The risk of transecting the anterior ethmoid artery (AEA) when lying in mesentery is a known risk of sinus surgery. 6
The objective of this study was to compare the AEA to skull base (AEA-SB) length in patients with AFRS versus non-AFRS CRSwNP, with the goal of improving preoperative planning and preventing inadvertent injury to the AEA. Additionally, this study sought to determine if there were differences in the presence of anatomic variants.
Materials and Methods
Study Design
A single institution, retrospective review of patients that received sinus surgery was approved by the University of Texas Health San Antonio Institutional Review Board (#HSC20180202H). Data was collected for patients over 18 years of age that underwent ESS from January 2021 to January 2023 at a single hospital. Basic demographic information (age, gender), indication for surgery, adverse events, and intraoperative findings were collected by chart review of the electronic medical record. All patients had thin-cut computed tomography (CT) imaging available for review. Patients without radiographic imaging and prior endoscopic sinus surgery were excluded from the study. Images in the bone windows were reviewed by 2 otolaryngologists in the coronal, sagittal, and axial planes, and results were averaged (d.e., m.k.). AFRS was determined as present or absent, and laterality was included if present. Measurements were only included if disease was present on that side. Criteria for AFRS diagnosis were based on the International Consensus Statement on Allergy and Rhinology, and included presence of characteristic fungal imaging findings, fungal elements or eosinophilic mucin noted on pathology, and type I hypersensitivity based on prior testing or history. 9 The control group consisted of patients undergoing ESS for non-AFRS CRSwNP. Patients with CRSwNP met diagnostic criteria as defined by the International Consensus Statement on Allergy and Rhinology, with pathologic presence of polyps. 9 Control group patients were selected as a number matched group to the AFRS group (21) and were only included if no prior surgeries and if disease was present bilaterally. Measurements from the beak of the anterior ethmoid artery (AEA) to the outer cortex of the skull base (AEA-SB) were measured on each side, this was taken from the sharpest point of the AEA’s exit from the orbit, and if the beak was abutting the skull base, measurement was noted as zero (Figure 1). The Keros measurement was measured as previously described by Keros et al 8 Additionally, the presence of concha bullosa (CB), infraorbital ethmoid cell, sphenoethmoidal air cell, and supraorbital ethmoidal air cell (SOEC) was determined as present or absent, and laterality was included if present, as previously suggested with high reliability. 10 For sinonasal variant presence, measuring authors (d.e., m.k) had to be in agreement. In the event of a disagreement, the senior author reviewed the in-question imaging and consensus was agreed upon by the 3 authors.
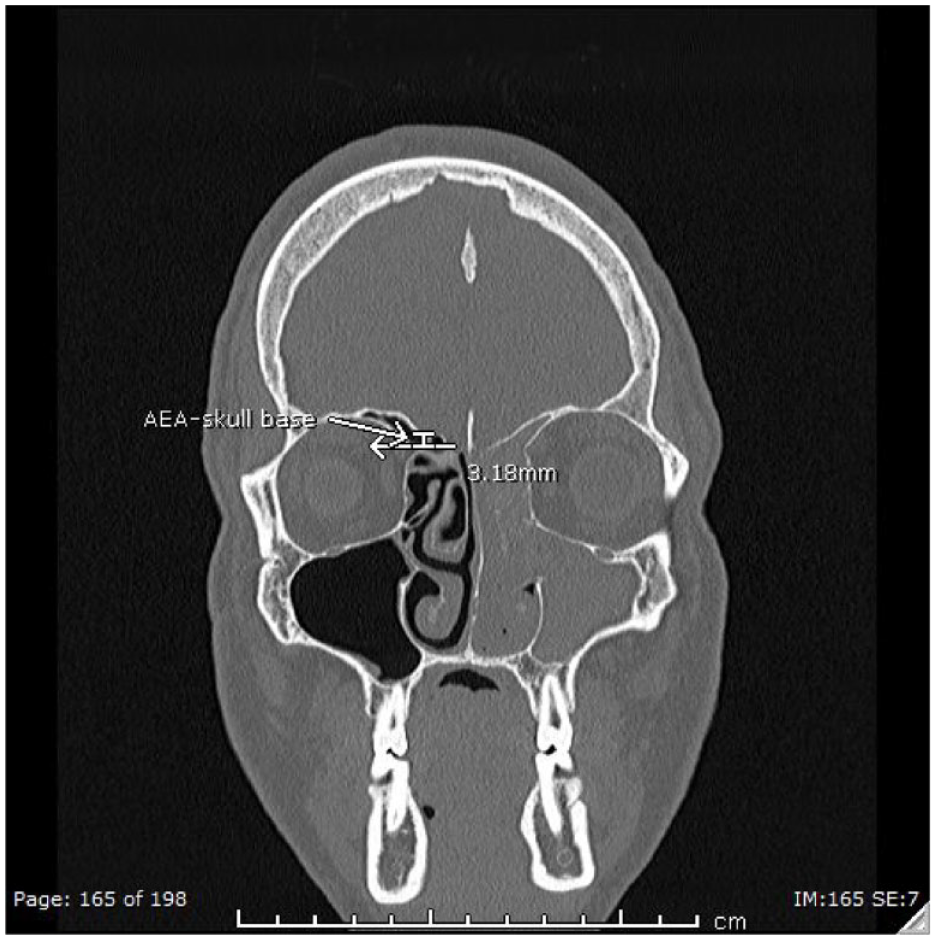
Anterior Ethmoid Artery to Skull Base Length (AEA-SB) on computerized tomography (CT). Illustration of AEA-SB measurement depicted by white line.
Statistical Methods
Continuous variables were reported as means and standard deviations while categorical variables were reported as counts with percentages. Differences in continuous variables between the AFRS group and CRSwNP group were compared using the 2-sample t-test. Chi-square test and Fishers exact test were used for differences in categorical variables. Alpha was set to .05 to determine statistical significance. All statistical analyses were performed using Stata (Stata LLC, College Station, TX).
Results
A total of 42 patients (AFRS: 21, CRSwNP: 21) were included in this study. The group had a mean age of 42.2 years (SD = 14.5). Majority of study participants were male (61.9%), and did not have concha bullosa (76.2%), infraorbital ethmoid cells (85.7%), or sphenoethmoidal cells (57.1%) present on imaging. However, 76.2% of subjects had a SOEC present on imaging. The average AEA-SB length was 2.15 mm (SD 1.65), while the average Keros measurement was 5.31 mm (SD 1.11).
On bivariate analysis, the AFRS group was significantly younger (mean age: 36.9, SD 12.8) compared to the CRSwNP group (Mage = 47.5, SD = 14.4; P = .015). Additionally, the AFRS group had a significantly longer AEA-SB length (AFRS = 2.76 mm [SD = 1.60] compared to CRSwNP = 1.53 mm [SD = 1.50]; P = .014) compared to the CRSwNP group. No significant differences were observed between the 2 groups regarding gender, Keros class, presence of concha bullosa, sphenoethmoidal cells, infraorbital ethmoid cells, or SOEC. See Table 1 for characteristics of study participants and Table 2 for analyses by disease type.
Sample Characteristics of Study Participants.
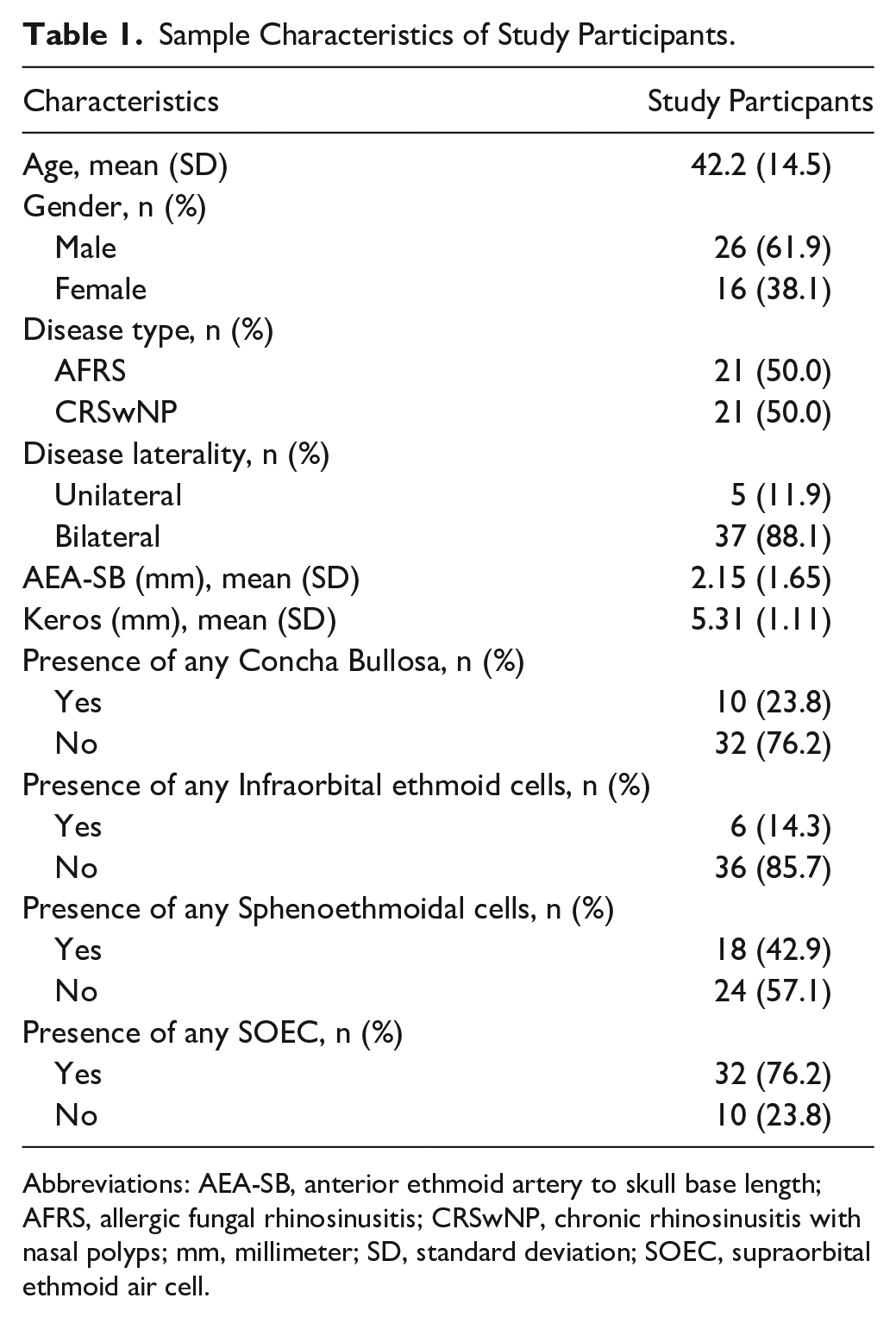
Abbreviations: AEA-SB, anterior ethmoid artery to skull base length; AFRS, allergic fungal rhinosinusitis; CRSwNP, chronic rhinosinusitis with nasal polyps; mm, millimeter; SD, standard deviation; SOEC, supraorbital ethmoid air cell.
Bivariate Analysis of Patient Characteristics by Disease Type.
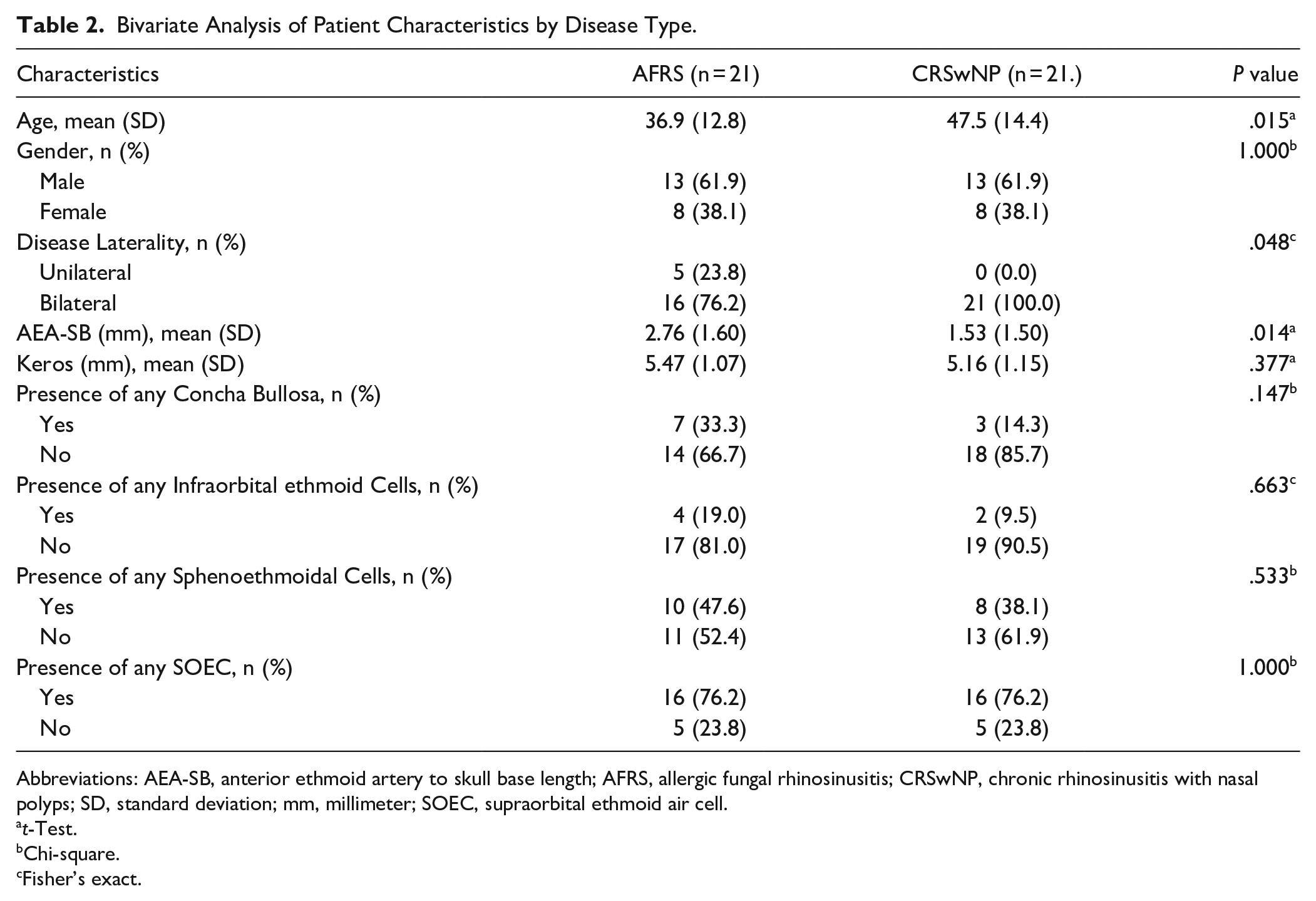
Abbreviations: AEA-SB, anterior ethmoid artery to skull base length; AFRS, allergic fungal rhinosinusitis; CRSwNP, chronic rhinosinusitis with nasal polyps; SD, standard deviation; mm, millimeter; SOEC, supraorbital ethmoid air cell.
t-Test.
Chi-square.
Fisher’s exact.
Discussion
This study was performed to analyze the association of AFRS in anatomic variants of the sinuses, and to aid in preoperative planning to prevent surgical complications during ESS. The clinical presentation of AFRS has been well described, as well as the radiographic diagnosis, but literature is lacking on the relative changes in sinonasal anatomy associated with the diagnosis of AFRS. 5 This study is the first to demonstrate an increased distance from the skull base to the anterior ethmoid artery in patients with AFRS. Additionally, this study is the first to show no significant difference in the presence of common sinonasal variants specifically in AFRS and CRSwNP.
Current consensus on AFRS diagnosis includes a clinical suspicion of diagnosis, with supporting features such as evidence of type I hypersensitivity, Charcot-Leiden crystals, eosinophilic mucin, bony erosion, and/or evidence of heterogenous opacification on CT imaging. 11 Management is supported with a combination of medical management and endoscopic surgical removal of disease. 12 AFRS has a higher rate of recurrence and need for additional surgery than traditional CRSwNP, and as in CRS, post-surgical medical management is first line in targeting recurrence.12 -14 Of note, the role of biologics as adjunct management has expanded rapidly in recent years and provides potential medical options for recurrence and primary management. 14 As discussed, local bony erosion is more common in AFRS than CRSwNP alone, and these changes further complicate surgical management.15,16 These bony changes are of high importance in surgical planning to avoid surgical complications.
The AEA is an important structure to identify in ESS, and if damaged inadvertently, can lead to serious complications such as orbital hematoma or blindness. 6 The presence of the AEA hanging in a mesentery is often discussed by endoscopic sinus surgeons, and this anatomic variant has previously been published as an important finding to note. 6 Shorter distance between the skull base and AEA is believed to confer protection during sinus surgery, while greater distances result in higher probability of inadevertently damaging the artery. 7 It has been noted that SOEC presence and size were associated with increased distance of the AEA to the skull base. We found no differences in SOEC presence in our 2 groups, but incidence of SOEC was consistent with previously published rates. 17 Although, there has been little additional research exploring AEA-SB variations in CRSwNP, and specifically AFRS. Likewise, variations in skull base height have been well-described as a risk factor for complication in endoscopic sinus surgery. As demononstrated with prior studies, checklists are a crucial aspect of preoperative planning, and we believe the AEA-SB length should be an additional consideration in preoperative planning, especially with AFRS.8,18,19 Our findings are within expected ranges as previously published data regarding distance from the skull base to the AEA. 20
Previous studies have examined sinonasal variants in AFRS, notably the presence of infraorbital ethmoid, sphenoethmoidal, CB, and SOEC. 21 Sinonasal variants have been extensively studied, and their relevance lies in their association with higher rates of sinus mucosal disease, complication, and recurrence after surgery.22,23 These studies demonstrated differences in sinonasal variant presence, notably the presence of CB and infraorbital ethmoid cell was shown to be more likely in AFRS.3,21 We found no significant difference in presence of sinonasal variants (infraorbital ethmoid, sphenoethmoidal, CB, or SOEC) between our AFRS and CRSwNP groups. Our findings were consistent with previously published prevalence for anatomic variants. 24 We postulate that the difference in our results and those previously published is due to the utilized control group. In our study, we compared sides only if sinus disease was present, whereas previous studies utilized a non-CRS control or a disease-free self-control. We believe the utilization of a CRS control is more accurate, as these comparisons can more directly be attributed to AFRS, not CRS in general.
In this study, we illustrated that the AEA-SB length was longer in patients with AFRS when compared to a CRSwNP control. The increased distance of AEA-SB may be related to bony expansion commonly seen in patients with AFRS, and therefore may lead to increased risk during surgical management. Additionally, we illustrate that the presence of sinonasal variants (infraorbital ethmoid, sphenoethmoidal, CB, and SOEC) was similar in AFRS patients when compared to CRSwNP, whereas differences had previously been reported. This finding is significant due to the previously demonstrated association between sinonasal variants, recurrence, and complications. Additionally, our study’s utilization of 2 independent reviewers may provide additional accuracy of imaging findings.
Retrospective cohort studies of relatively rare pathologies have several inherent limitations. This study has risk of selection bias because inclusion criteria was based on chart review for disease presence. To minimize this bias, the authors used several sources to determine patients with disease, including electronic health record and surgeon records, and multiple reviewers of the imaging. Additionally, the relatively small size of the study may not hold true in larger cohorts. There were no AEA intra-operative injuries in our cohort, so larger studies may further delineate this complication. With larger studies, the SOEC pneumatization may be better elicited to further study subgroup variations as well. Further this population has geographic (and potential ethnic) characteristics that likely limit generalizability. We were additionally unable to compare ethnicity by limitations of our review, which may offer another potential confounder. This suggests further research to establish variations in sinus anatomy in patients with AFRS is needed. Lastly, additional imaging reviewers may further increase reliability and decrease bias in measurements.
Conclusion
AFRS has a longer AEA-SB length when compared with traditional CRSwNP. This key difference should be considered in the preoperative planning to prevent inadvertent injury to the AEA in patients undergoing ESS for AFRS.
Footnotes
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Philip Chen recieves consulting fees from Medtronic, speaking honoraria from GlaxoSmithKline and Optinose, and research funding from Aerin Medical.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.