
Abstract
Objectives
Inferior meatal antrostomy (IMA) is regarded as a safe method, with minimal complications, for managing various lesions in the maxillary sinus. However, in patients with persisting IMA window, resection of the inferior turbinate may result in direct airflow into the antrum, irritating the antral mucosa.
Methods:
Case report and review of literature.
Results/Case:
The present report describes a 29-year-old man who previously underwent unilateral IMA for the excision of a dentigerous cyst. The patient did not report any facial pain following the excision of the cyst. One year later, this patient underwent partial resection of the inferior turbinate for the resolution of nasal stuffiness by another surgeon. Soon after surgery, the patient developed severe facial and ocular pain on the side of the IMA, with the pain being especially aggravated upon inhalation. Endoscopy and computed tomography (CT) revealed a persisting IMA window. The patient’s severe discomfort was thought to result from direct airflow into the maxillary sinus, as the resected turbinate may have altered normal nasal airflow. A unilateral inferior meatal augmentation procedure (IMAP) with an autologous ear cartilage implant was performed, resulting in complete relief of pain and discomfort.
Conclusions:
Although IMA alone is a relatively safe surgical procedure, care should be taken when performing inferior turbinoplasty in patients with persistent IMA opening.
Introduction
Lesions in the maxillary sinuses, especially those located in the anteroinferior portion of the maxillary antrum, can be surgically accessed by an inferior meatal antrostomy (IMA). 1 In IMA, a surgical corridor is created through a window in the inferior meatus of the lateral nasal wall, enabling surgical access to the antrum through the nasal cavity (NC). 1 IMA window often undergoes spontaneous closure by surrounding mucosa and fibrous tissues, or it is intentionally opened for postoperative surveillance purposes. 2 Regardless of the IMA closure, almost no patient experiences any discomfort, thus IMA is considered a very safe surgical approach with minimal complications. 1
It is a well-known fact that an excessively resected inferior turbinate, especially the head portion, may cause the development of an empty nose syndrome (ENS). 3 Although few prior publications have reported a recirculation phenomenon following an IMA with excessive inferior turbinate resection,4,5 none have reported a case of a persisting IMA window in association with ENS or facial pain.
The present report describes a patient with a persisting IMA window who presented with severe unilateral facial and ocular pain following inferior turbinate resection. The patient was successfully treated with an inferior meatal augmentation procedure (IMAP), which was designed to divert the nasal airflow heading directly into the maxillary sinus.
Case Report
A 29-year-old man presented with severe right-sided facial and ocular pain accompanied by headache. The patient reported his pain as sudden, sharp, throbbing pain, which were shooting in his right cheek, temporal, and ocular region. The pain was especially triggered upon nasal inhalation, suggesting a neuropathic pain rather than a dull, constant pain. In addition, the patient reported ENS symptoms, such as bilateral nasal dryness, crusting, and a decrease in nasal airflow sensation.
The patient’s medical history included the excision of a dentigerous cyst from the right maxilla via a combination of sublabial and IMA approaches 7 years earlier. Five years after cyst removal, the patient complained of bilateral nasal obstruction, for which he underwent septoplasty with bilateral partial resection of the inferior turbinate (inferior turbinoplasty). All previous surgeries had been performed by another surgeon. The patient reported that his discomfort developed about 1 month after the turbinate surgery.
Examination of the NC showed that the nasal septum was relatively straight, although a resected inferior turbinate with scarred mucosa was observed bilaterally (Figure 1A). A 30° endoscope showed a persisting IMA opening in the anterior portion of the right lateral wall of the inferior meatus (Figure 1B). The IMA window was approximately 0.8 cm in diameter, directly connecting the right maxillary sinus and NC. Upon initial nasal endoscopy, no discharges were drained out from both MMA and IMA windows, ruling out a possibility of recirculation syndrome. Computed tomography (CT) showed a partially reduced inferior turbinate bilaterally, with an IMA window in the right inferior meatus (Figure 1C).
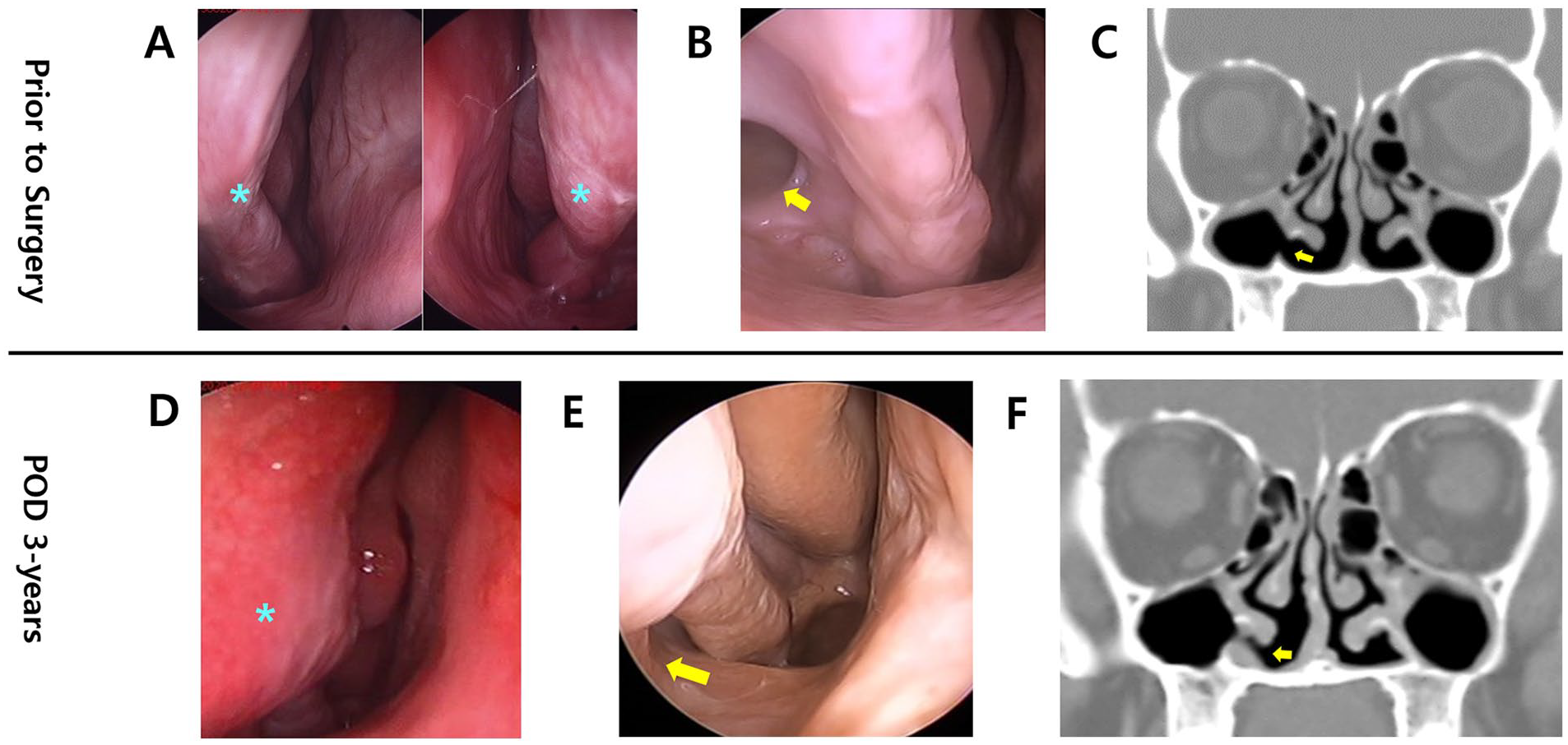
Endoscopic and CT findings in the 29-year-old male patient: Pre-operative endoscopic (A, B) and CT (C) images of a 29-year-old male patient with severe right-sided trigeminal neuralgia and ENS symptoms. Endoscopic images showed a bilaterally resected inferior turbinate (A, asterisks) with a right-sided IMA opening in the inferior meatus (B, arrow). Endoscopic (D,E) and CT (F) CT images 3 years after the operation. Endoscopic images showed that the augmented inferior meatus (D, asterisk) partially obliterated the previous IMA opening (E, arrow), whereas 3 year CT imaging showed a well-maintained autologous cartilage implant in the right inferior meatus (F, arrow).
Findings in this patient suggested that his right-sided ocular and facial pain was triggered by direct influx of air into the antrum through the IMA window in the inferior meatus, facilitated by the previous turbinoplasty. Based on findings in many ENS patients who had undergone inferior meatal augmentation with cartilage implant,6,7 IMAP was performed, as IMAP may reduce pain by diverting the nasal airflow directed toward the inferior meatus.
Under general anesthesia, the patient’s left cavum concha cartilage was harvested. IMAP was performed using a method similar to the surgical treatment of ENS with autologous cartilage grafting.6,7 Briefly, an incision was made on the piriform aperture, followed by subperiosteal-mucosal tunneling into the inferolateral wall of the inferior meatus. The harvested ear cartilage was molded in the shape of an oval ball, and the graft was inserted into the lateral wall pocket of the inferior meatus, just in front of the antral window, without violating the integrity of the nasal mucosa surrounding this window (Figure 2A). Reinforcement of the lateral wall in the inferior meatus partially obliterated the IMA window (Figure 2B) in the anterior part (Figure 2C). The surgery was terminated without any perioperative complications.
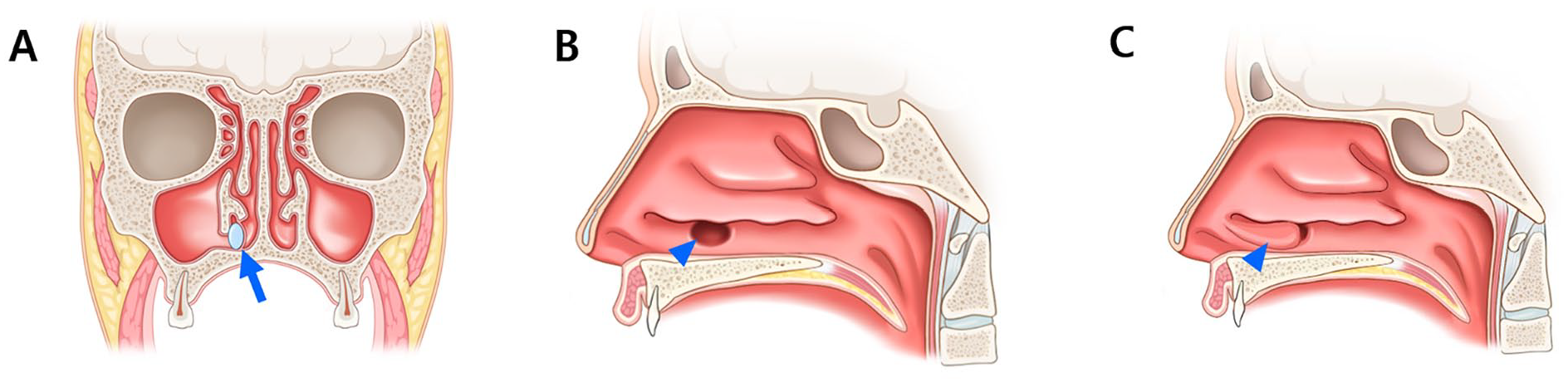
Illustration of the inferior turbinate reconstruction via submucosal autologous cartilage implant. Illustrations showing the procedures by which the submucosal autologous cartilage implant was used to reconstruct the resected inferior turbinate and to obliterate the IMA window made during the previous operation. The autologous cartilage implant was placed below the mucosal layer of the inferior meatus, medial to the IMA opening (A, asterisk). This allowed the IMA opening (B, arrowhead) to be partially obliterated (C, arrowhead).
The patient reported the complete resolution of facial pain a few weeks after surgery, with absence of pain continuing for at least 3 years. Additionally, the patient’s nasal dryness and nasal suffocation symptoms on the side of the operated NC were resolved. The ear cartilage donor site wound was fully healed, with minimal scarring. Endoscopy and CT examination at 3 years showed a well-maintained augmented lateral wall of the inferior meatus with ear cartilage grafting (Figure 1D), partially obscuring the IMA window on the operated side of the NC (Figure 1E and F).
Discussion
This report describes a patient with a persisting IMA window on the right nasal wall of the inferior meatus who developed severe right-sided facial and ocular pain soon after undergoing inferior turbinoplasty. The partially resected inferior turbinate resulted in widening of the inferior meatus, allowing the maxillary sinus antrum to be completely exposed to the NC through the IMA window, with this physical alteration resulting in severe discomfort. To divert the airflow directed toward the antrum, the anterolateral wall of the inferior meatus was augmented by autologous cartilage graft implantation. Following IMAP, the patient reported resolution of facial and ocular pain and nasal dryness, as well as an improved sense of nasal airflow. CT examination after 3 years showed an augmented anterolateral nasal wall in the inferior meatus, partially obliterating the previous IMA opening.
The patient did not experience facial pain or irritation following earlier dentigerous cyst removal via IMA and sublabial approaches. Rather, he complained of bilateral nasal obstruction symptoms a few years later. Although the CT image taken just prior to turbinate resection (Supplemental Figure 1) showed persisting IMA window, the patient did not report any facial pain. Interestingly, the patient reported severe neuropathic pain only in the side of a patent IMA opening following turbinate resection, although the turbinate resection was performed bilaterally. Thus, it can be concluded that the patient’s ipsilateral localizing pain might have been a combined result of inferior turbinate partial resection impacted on a side of a patent IMA opening, rather than ENS presenting as in the form of a facial pain.
To our knowledge, facial pain and discomfort have never been reported in patients with IMA windows triggered by inferior turbinate resection. Findings in the present patient suggest probable triggering of the antral mucosa or infraorbital nerve (ION) with direct airflow stimulation through the IMA window in the inferior meatus. Primary closure of the IMA opening with a nasal lateral wall mucosal advancement flap would have served as a treatment option. However, the concurrent presence of ENS symptoms led to the choice of IMAP, which resulted in diversion of the nasal airflow toward the antrum, resolution of severe facial pain, and relief of ENS symptoms.
Similarly, Yi and Jin 8 reported submucosal autologous costal cartilage grafting in the anterior inferior meatus, resulting in the successful management of pain in a patient with unilateral facial neuralgia following IMA. Their patient had previously undergone a Caldwell-Luc operation, which resulted in postoperative cheek cyst development, followed by cyst marsupialization through an IMA approach. However, their patient did not present with any ENS symptoms other than facial pain, and had no history of inferior turbinate resection, as CT imaging showed preserved inferior turbinate volume. The previous patient also exhibited severely contracted antral mucosa and destruction of the maxillary sinus bony skeleton with hanging of the ION in the antrum, explaining the direct triggering of ION through the IMA opening. Nevertheless, IMAP relieved facial pain in both our and their 8 patients, suggesting that altering the nasal airflow vector might have resulted in symptom relief in both patients.
IMAP using our surgical technique is effective in patients with ENS6,7 and primary atrophic rhinitis. 9 IMAP is also useful in restoring normal aerodynamics in the NC, thereby relieving ENS-associated symptoms.10 -12 Recent advances in computational fluid dynamic (CFD) modeling 13 have supported the impact of inferior turbinate resection, especially on the anterior part of nasal airflow, and the effects of inferior turbinate reconstruction in nasal aerodynamics. Results in the present patient showed that facial pain was completely resolved with IMAP, although the IMA window remained partially opened to the NC. 11
Although this patient’s severe facial and ocular pain on the side of IMA that had undergone resection of the inferior turbinate was successfully managed, the aerodynamics of altered nasal airflow in this patient could not be determined. Nonetheless, this previously unreported complication associated with IMA was successfully managed with IMAP. Findings in this patient emphasize the need for conservative inferior turbinoplasty in patients with persisting IMA windows.
Conclusion
The present report describes a patient with a persisting IMA window who developed severe facial and ocular pain following partial resection of the inferior turbinate. The pain completely resolved with IMAP using an autologous cartilage implant. In patients with persisting IMA window, inferior turbinoplasty should be conservatively performed.
Supplemental Material
sj-docx-1-aor-10.1177_00034894231180948 – Supplemental material for Facial Pain Triggered by Inferior Turbinate Partial Resection in a Patient with a Previous History of Inferior Meatal Antrostomy: A Case Report
Supplemental material, sj-docx-1-aor-10.1177_00034894231180948 for Facial Pain Triggered by Inferior Turbinate Partial Resection in a Patient with a Previous History of Inferior Meatal Antrostomy: A Case Report by Marn Joon Park and Yong Ju Jang in Annals of Otology, Rhinology & Laryngology
Supplemental Material
sj-tif-2-aor-10.1177_00034894231180948 – Supplemental material for Facial Pain Triggered by Inferior Turbinate Partial Resection in a Patient with a Previous History of Inferior Meatal Antrostomy: A Case Report
Supplemental material, sj-tif-2-aor-10.1177_00034894231180948 for Facial Pain Triggered by Inferior Turbinate Partial Resection in a Patient with a Previous History of Inferior Meatal Antrostomy: A Case Report by Marn Joon Park and Yong Ju Jang in Annals of Otology, Rhinology & Laryngology
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
This study was approved by the institutional review board (IRB) of Asan Medical Center, with an exemption of the informed consent (investigation approval no. 2022-0811).
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.