
Abstract
Introduction
Nasal septal perforation is often seen clinically, 1 but the repair operation is technically difficult to perform and the outcomes are typically not successful. In recent years with the continuous improvement of endoscopic techniques, the surgical success rate has increased significantly. However, success rates remain low in cases of large and/or complicated defects. 2 Since June 2018, our department has used biologic grafts for repairing nasal septal perforations, achieving satisfactory results and greatly reducing the technical difficulty of the operation.
Patients and Methods
Materials and Methods
The Ethics Committee of General Hospital of Xinjiang Military Region has reviewed the proposed use of human subjects in the aforementioned projects. The research plan and other materials submitted comply with the principles of medical ethics and the requirements of Helsinki Declaration. It is recognized that the rights and the welfare of the subjects are adequately protected; the potential risks are outweighed by potential benefits (Ethical Approval No. GHXJMR-EC099). Furthermore, the written consent was informed, and patients provided informed written consent to have data from their medical records used in our research.
Patients and Etiology
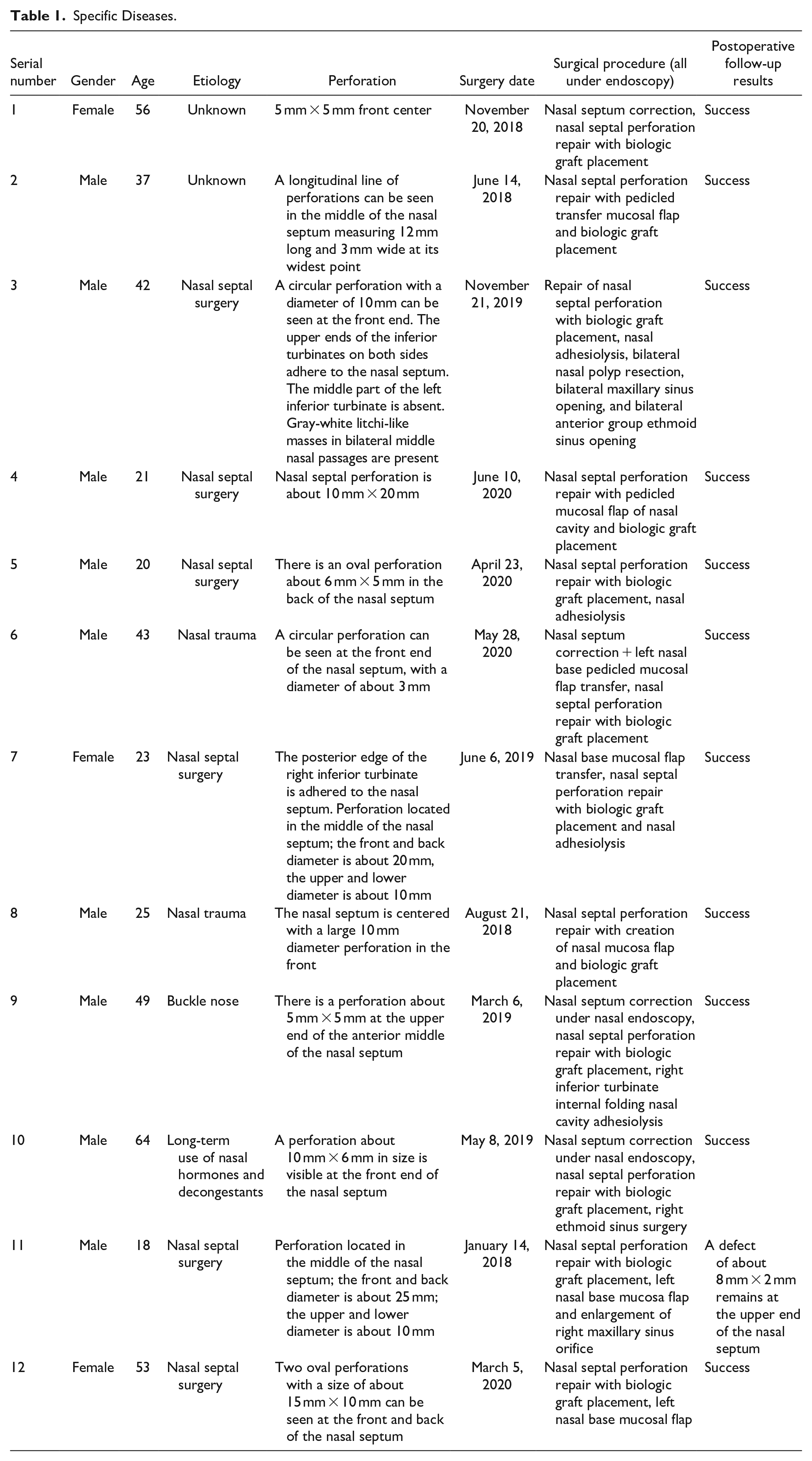
From 2018 to 2020, 12 cases of nasal septal perforation were treated with a biologic graft. The patient cohort included 9 males and 3 females whose age ranged from 18 to 64 years. The patients’ average age was 38 years, and the disease had been present for anywhere between 2 months and 8 years. Two cases were of unknown etiology, 1 case was caused by nose picking, 6 cases were caused by nasal cavity surgery, 2 cases were caused by trauma, and 1 case was caused by long-term use of nasal hormones and decongestants. All patients had differing degrees of dryness of the nasal cavity, crusting, headache, nasal congestion, nose bleeding or blood in the mucus, and whistle sounds when breathing. 3 Perforation location in the nasal septum varied and the size varied from 5 mm to 20 mm. There were 4 cases with nasal septal deviation, 4 cases with nasal adhesions, 2 cases with sinusitis, and 1 case with nasal neoplasms (specific diseases are shown in Table 1). The preoperative endoscopy and computed tomography scan of 1 patient are shown in Figure 1. Written informed consent was obtained from all patients.
Specific Diseases.
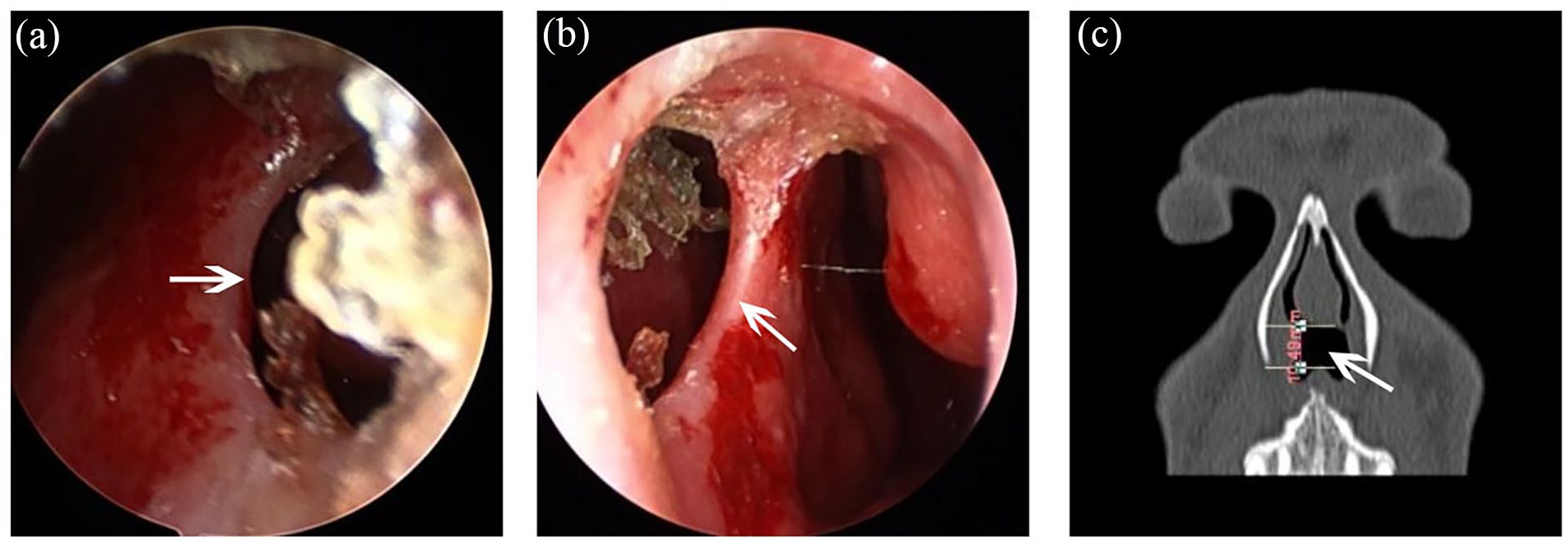
Preoperative endoscopy and coronary CT scans of nasal septum before the surgery. (a, b) The nasal septum is centered with a large 10 mm diameter perforation in the front by preoperative endoscopy. (c) A large 10 mm diameter perforation in the front of nasal septum by the coronary CT scans before the surgery. White arrow, a large 10 mm diameter perforation; CT, computed tomography.
Surgical Technique
The nasal septum was dissected via endoscopic approach. 4 A 4 cm × 7 cm biologic graft (Biodesign® Tissue Graft) was folded to form a double layer, was placed over the perforation with at least a 5 mm overlap, and was affixed into place using suture. In 5 patients, residual nasal septal cartilage was inserted into the graft, which was affixed with suture approximately 5 mm from the edge of the perforation. Three patients with perforations greater than 15 mm underwent the transfer of the left nasal base mucosal flap to repair the left perforation.
Postoperative Treatment
After the operation, the nasal cavity was left open and the nasal cavities on both sides were splinted and then moisturized with silica gel. 5 Antibiotics were routinely used for 2 days after the operation. The 3 patients with perforations greater than 15 mm were given vasodilators and drugs (sodium aescinate) to improve microcirculation. Silicone sheets were removed after 1 month. All patients routinely used an epidermal growth factor nasal spray (GeneTime, recombinant human epidermal growth factor derivative for external use, liquid) for the first postoperative month. Two to 3 months after the operation, patients were allowed to block the front nostril with a small cotton ball.
A Post Hoc Power Analysis
First, we encoded the description information on gender, age, etiology, perforation, and surgical procedure (all under endoscopy) (1, 2, 3, 4, 5 . . .), and the data are quantified (shown in Supplemental Table 2). Second, descriptive analysis and normality test were carried out on the data (shown in Supplemental Table 3). In view of the results of Shapiro-Wilk test and Kolmogorov-Smirnov test (P < .01), we can carry out the analysis of variance (shown in Supplemental Table 4). According to the results of variance analysis on etiology and perforation items (P < .05), it preliminarily confirmed that post hoc multiple comparative analysis can be available. Because the analysis of variance is significant, we can make a preliminary quantitative analysis of the difference with quantitative analysis of effect (shown in Supplemental Table 5). Based on the aforementioned data of etiology and perforation, we should focus on the analysis results of etiology and perforation in the subsequent postevent analysis.
Next, the results of Bonferroni variance analysis showed that there is no significant difference between gender in the variable etiology without multiple comparisons after the event. Meanwhile, the variable perforation has significant differences between gender (P = .044**), and post hoc multiple comparisons are indispensable (shown in Table 2). Finally, the results of post hoc multiple comparisons showed that: (1) for variable age and surgical procedure, the order of the mean value is: 1.0 > 2.0. There is no significant difference in the overall mean. (2) For the variable etiology, the order of the mean value is: 2.0 > 1.0. There is no significant difference in the overall mean. (3) For the variable perforation, the order of the mean value is: 1.0 > 2.0. There is a significant difference between 1.0 and 2.0. (shown in Table 3).
Bonferroni Variance Analysis.
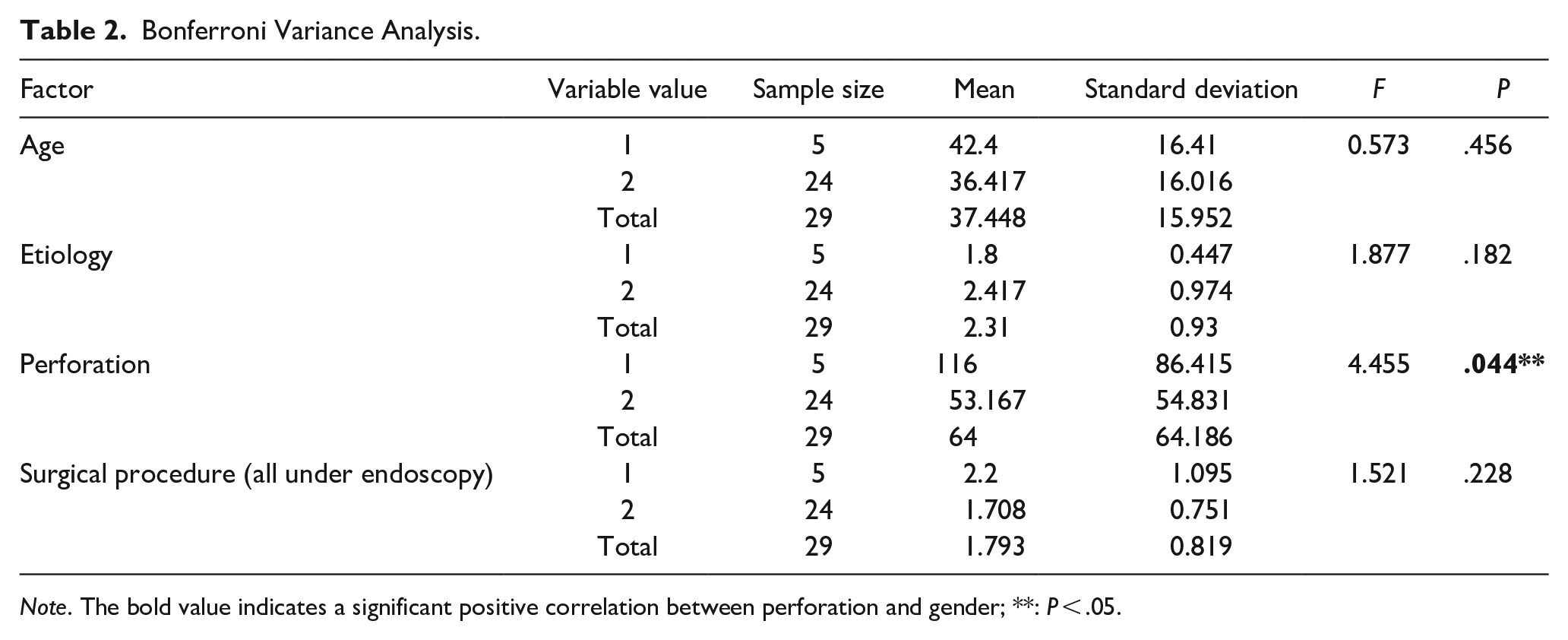
Note. The bold value indicates a significant positive correlation between perforation and gender; **: P < .05.
A Post Hoc Multiple Comparisons.
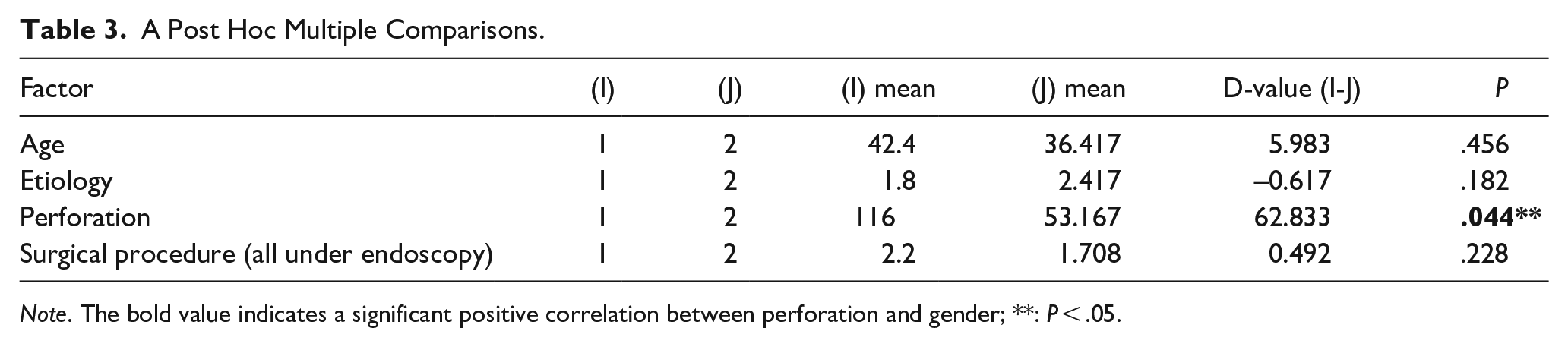
Note. The bold value indicates a significant positive correlation between perforation and gender; **: P < .05.
Results
Follow-up ranged from 2 to 8 months after the operation. One patient was not completely healed and presented with a remaining defect of about 2 mm × 8 mm in the upper part of the nasal septum. This patient had a perforation of more than 20 mm at surgery, presented with an insufficient blood supply at the margins, and received a mucosal flap that did not adequately cover one side of the defect during the procedure. The remaining 11 patients healed completely. Postoperative endoscopies are shown in Figure 2.
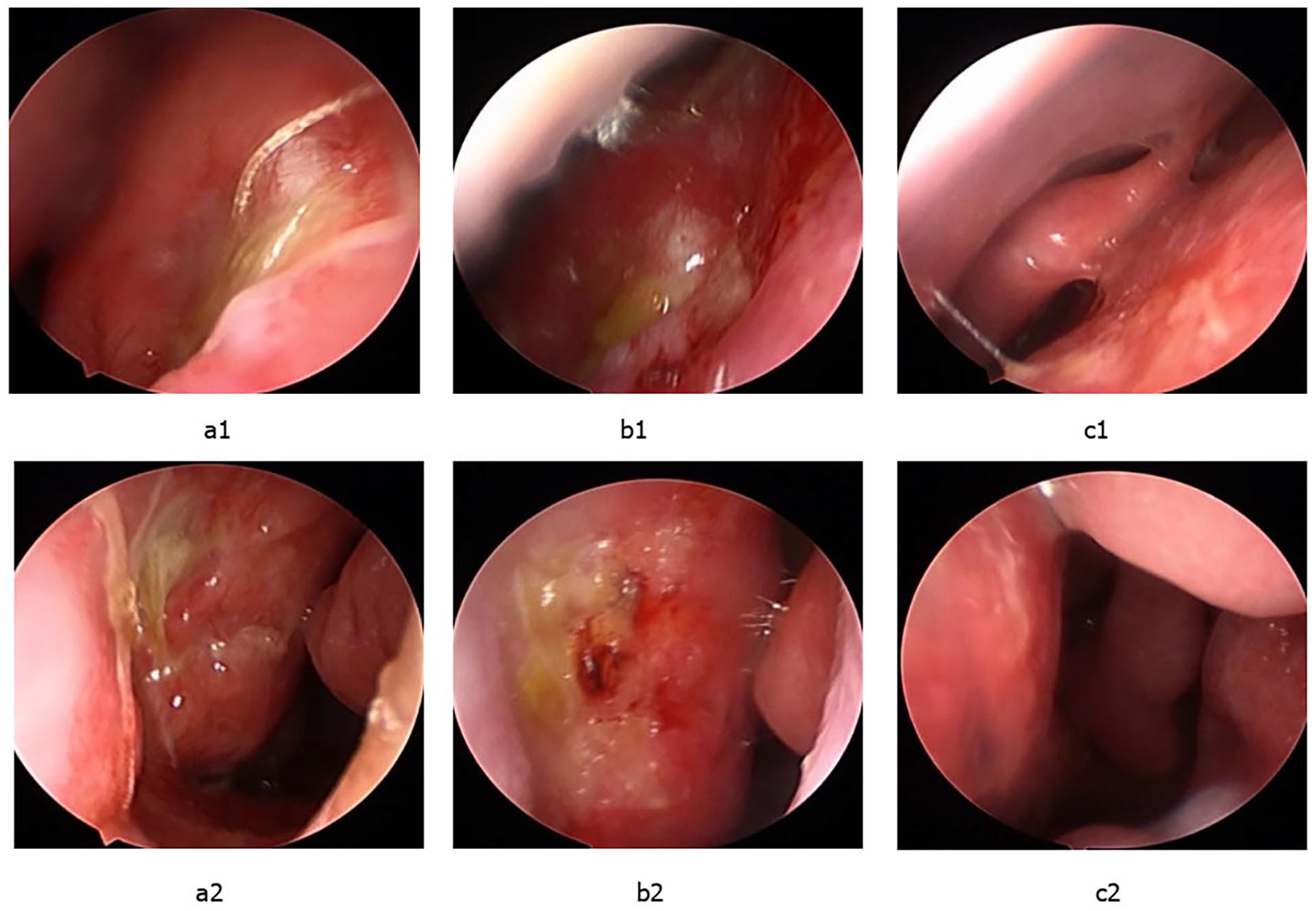
Postoperative endoscopies. (a1, a2) One month after operation, the repaired part of nasal septum perforation was largely epithelialized, but the absorbable thread was still fixed in place. (b1, b2) Two months after operation, the repaired part of nasal septum perforation was completely epithelialized, and most of the absorbable thread was absorbed. (c1, c2) Three months after operation, the mucosa of nasal septum was intact and healed well.
Discussion
Nasal septal perforation refers to the formation of permanent perforations of different sizes and shapes in any part of the nasal septum, such that the 2 sides become connected. The condition is not a clinically uncommon disease. 6 There are several etiologies for nasal septal perforation including iatrogenic causes, poor lifestyle habits, occupational factors, and trauma. 7 At present, iatrogenic septal perforation, especially after septum surgery, is the most common etiology.8,9 Six of the 12 cases in this article were caused by nasal surgery, 2 cases were due to nasal trauma, 1 was a bad lifestyle habit, and 1 was a history of long-term use of nasal hormones and decongestants, which are all the etiologies consistent with other reports.
At present, an important method for the treatment of nasal septal perforation is surgical repair to restore the physiological function and normal shape of the nasal cavity as much as possible. 6 However, surgical repair is often difficult, and the success rate is low. 10 In addition, there are many different surgical techniques and no clear classification methods. Published articles confuse the surgical repair technique with repair materials, and so it may be useful and appropriate to classify the surgical methods.
Choice of Surgical Approach
Many peer-reviewed publications confuse the repair method of nasal septum perforation with repair materials,11,12 and there is no clear classification method. The author believes that it is more appropriate to classify the surgical methods as follows based on various theories.
(1) Tension reduction with suture, also known as the displacement suture method 13 ; (2) plastic repair method 13 ; (3) external sticking method, with or without free tissue flaps or pedicled mucosal flaps; (4) sandwich method, with or without free tissue flaps or pedicled mucosal flaps; and (5) combined use of the aforementioned surgical combinations, such as the nasal cavity pedicled mucosal flap combined with a nasal cavity free tissue flap or an autologous distant free tissue flap, foreign body materials, or artificial or biologic materials. In this article, 4 cases used biologic materials directly (Biodesign® Tissue Graft), 5 cases used a combined technique with free nasal septal cartilage, and another 3 cases used a combined technique with nasal base pedicled mucosal flap transfer repair, all of which achieved good results.
The pedicled tissue flap in the published literature should belong to the external sticking method category. 2 As for the compound tissue flap reported in the literature, many authors regard the combined operation as a compound tissue flap, which is a wrong concept.14,15 The concept of a composite tissue flap refers to a living tissue unit that contains a variety of tissue structures and has its own blood supply. From the perspective of blood supply, composite tissue flaps can be divided into 2 categories: a simple composite tissue flap supported by a single vascular pedicle and a composite tissue flap supported by multiple vascular pedicles. What most authors describe in the literature should therefore be the combined use of various mucosal flaps and free tissue flaps or materials. 16
Selection of Repair Materials
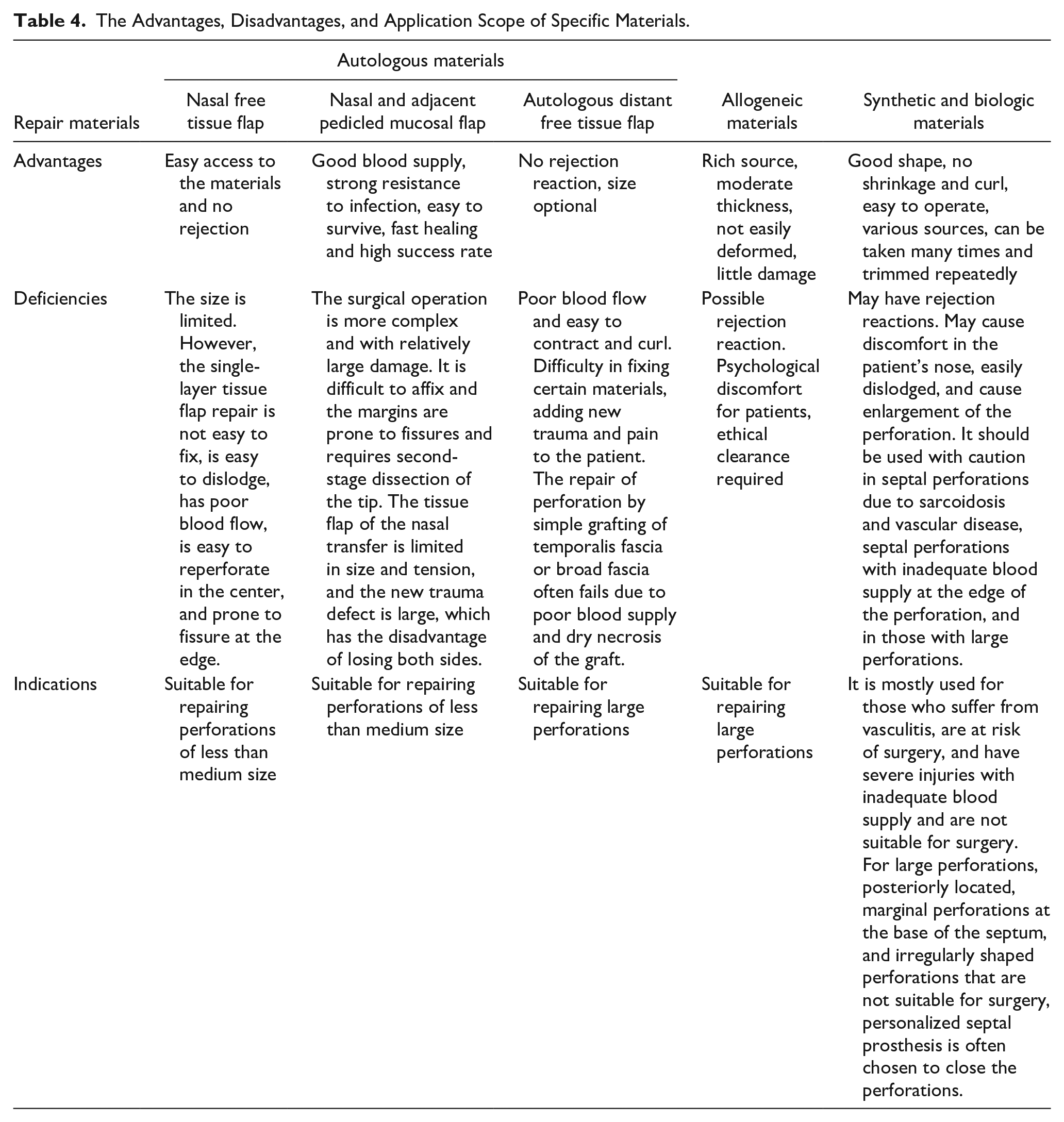
Repair materials used in nasal septal perforation repair can be classified into autologous materials17,18 (including nasal cavity free tissue flaps, nasal cavity and nearby pedicled mucosal flaps, or autologous distant free tissue flaps), allogeneic materials, and artificial/biologic materials. The specific material classification is shown in Figure 3. The advantages, disadvantages, and application scope of specific materials are shown in Table 4. Among them, a biologic graft 19 is derived from autologous or heterogeneous skin, small intestinal submucosal tissue, or other collagen matrix material. It is decellularized and manufactured to reduce immunogenicity using various treatment methods. The decellularized matrix material retains the 3-dimensional framework of the extracellular matrix, which can support the growth and proliferation of cells, and further promote the adhesion, growth, and proliferation of different cell types in the injured area to repair and reconstruct the defective tissue. The 3-dimensional support structure and the biologic growth factors contained in the extracellular matrix can promote tissue repair, and the released biological signals can promote nerve cell differentiation and vascular regeneration. 20
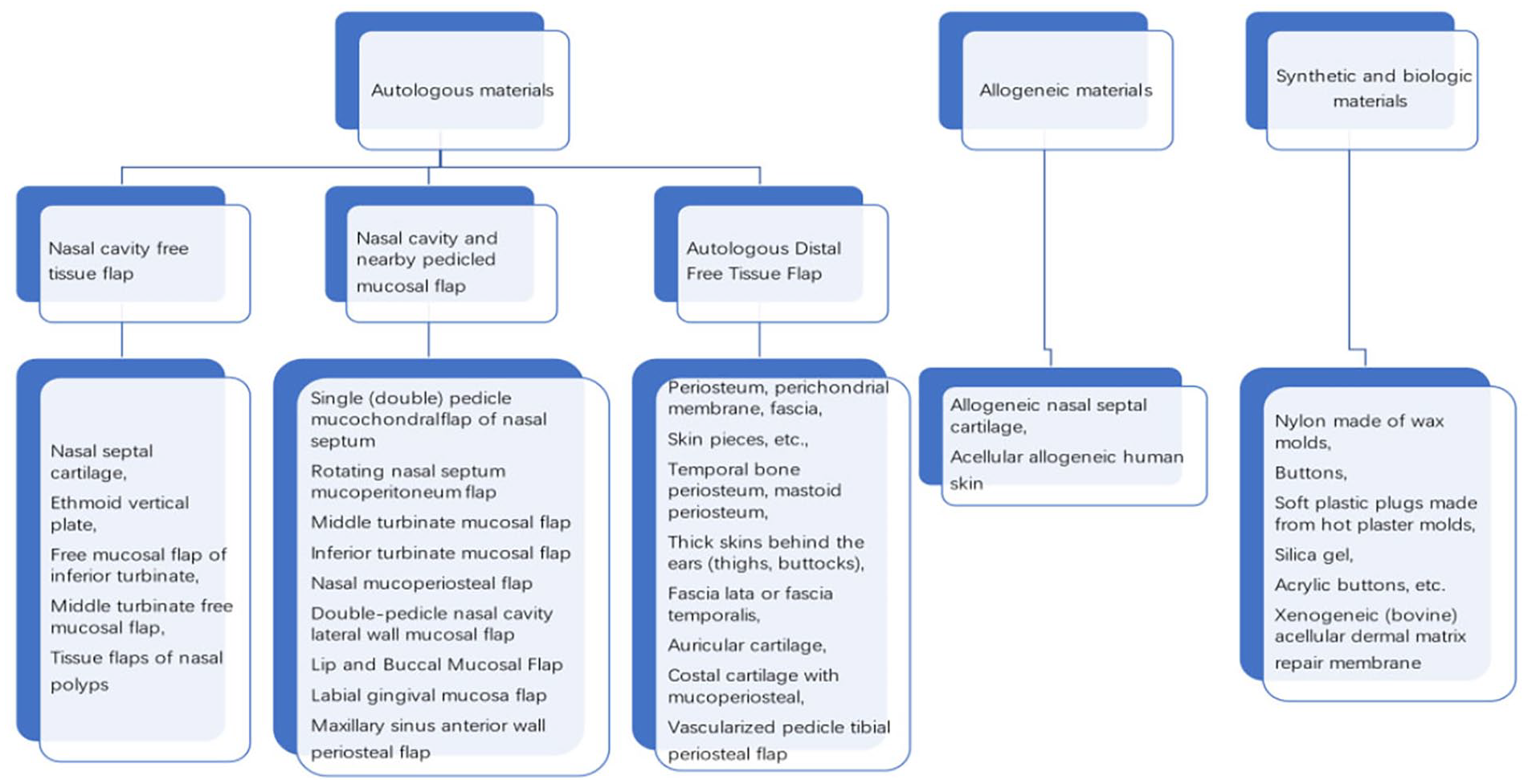
Selection of different repair materials under different conditions. The repair materials can be classified into autologous materials (including nasal cavity free tissue flaps, nasal cavity and nearby pedicled mucosal flaps, or autologous distant free tissue flaps), allogeneic materials, and artificial/biologic materials.
The Advantages, Disadvantages, and Application Scope of Specific Materials.
We have used a biologic graft material for nasal septal perforation and have found that patient selection and surgical technique are important to achieving good outcomes. (1) Relatively young patients with fast basal metabolism should be selected, because these factors are conducive to rapid tissue reconstruction. (2) While the necrotic tissue and mucosa around the perforation should be excised as much as possible, the mucoperiosteal flaps of the bilateral nasal septum should be separated widely to ensure the fixation of the biologic graft between the mucous periosteum. If necessary, suture fixation can be used to strengthen the repair. (3) The tissue graft can be used to induce the growth of soft tissue in the internal nasal cavity, and successfully reconstruct a perfect autologous soft tissue which can be used to replace the autologous fascia and provide a collagen framework for tissue growth. 21 In addition, the growth factors contained in the tissue graft can help the newly deposited tissue to quickly vascularize and tolerate infection. (4) For patients with a perforation greater than 1 cm, the graft should be augmented with a mucosal flap, which significantly increases the chance of success. (5) For perforations with a nasal septum of more than 1 cm, the blood supply to the center of the repair becomes a problem, 22 causing reperforation as a result of central ischemia. A mucosal flap on 1 side can seal the perforation as much as possible but minimizing the gap to 5 mm or less is more likely to result in a successful outcome and lessen the chances of reperforation. (6) Patients with a perforation area of greater than 2 cm should be chosen carefully due to the increased risk of a recurrent perforation. (7) For patients with severe bilateral mucosal damage during nasal septum surgery, but no mucosal loss, the biologic graft can be directly inserted without flaps. 13 Doing so will result in good healing, greatly reduce the chance of postoperative perforation, and avoid the pain and expense of a reoperation.
The biologic material used in this study, the Biodesign® Tissue Graft, has several advantages over other materials. The tissue graft can be used in the internal nasal cavity to induce the growth of soft tissue and remodel into a fully functional autologous soft tissue which can be used to replace the autologous fascia and provide a collagen framework for tissue growth. 23 In addition, the growth factors contained in the tissue graft can help the newly-deposited tissue to quickly vascularize and tolerate infection. 12 For patients with severe bilateral mucosal damage during nasal septum surgery but no mucosal loss, the biologic graft can be directly inserted without flaps. 24 The patient’s recovery status is good, which greatly reduces the chance of postoperative reperforation and helps reduce the patient’s pain and expense of reoperation.
In recent years, biologic grafts have been widely used clinically in neurosurgery, orthopedics, dermatology, urology, thoracic surgery, otolaryngology, and head and neck surgery. No obvious side effects of surgery have been found, but there are still risks that have not been assessed.25,26 The economic cost is relatively high: at present, the 2 cm × 3 cm patch is priced at more than 4000 yuan, and the 4 cm × 7 cm patch is more than 6000 yuan. The economic cost of patients has increased significantly. 27 There has been no continuous follow-up to determine long-term success, and no long-term evaluation of whether there are adverse effects on the body, such as the impact on tumors. All these factors need further exploration and study.
Using a biologic graft to repair nasal septal perforations is an easy operation, prevents the need to take autologous tissue from the patient, allows for a repair to be performed without creating septal flaps, and has good histocompatibility. 13 It is a safe and effective method that can be used clinically.
Limitations of Our Work
Due to limited cases that have been operated on, we did not statistically analyze data on application of biologic graft. Furthermore, continuous follow-up on long-term success and long-term evaluation of whether there are adverse effects on the body should be considered to focus on. Therefore, we will study further these aforementioned issues in our next work.
Supplemental Material
sj-docx-3-ear-10.1177_01455613241233748 – Supplemental material for Application of Biologic Graft in Nasal Septal Perforation Repair
Supplemental material, sj-docx-3-ear-10.1177_01455613241233748 for Application of Biologic Graft in Nasal Septal Perforation Repair by Jianjun Jing, Liang Li, Yongxiang Wu, Liang Zheng, Longfang Zhang, Haihong Li and Hui Wang in Ear, Nose & Throat Journal
Supplemental Material
sj-jpg-1-ear-10.1177_01455613241233748 – Supplemental material for Application of Biologic Graft in Nasal Septal Perforation Repair
Supplemental material, sj-jpg-1-ear-10.1177_01455613241233748 for Application of Biologic Graft in Nasal Septal Perforation Repair by Jianjun Jing, Liang Li, Yongxiang Wu, Liang Zheng, Longfang Zhang, Haihong Li and Hui Wang in Ear, Nose & Throat Journal
Supplemental Material
sj-jpg-2-ear-10.1177_01455613241233748 – Supplemental material for Application of Biologic Graft in Nasal Septal Perforation Repair
Supplemental material, sj-jpg-2-ear-10.1177_01455613241233748 for Application of Biologic Graft in Nasal Septal Perforation Repair by Jianjun Jing, Liang Li, Yongxiang Wu, Liang Zheng, Longfang Zhang, Haihong Li and Hui Wang in Ear, Nose & Throat Journal
Footnotes
Author Contributions
Concept and design: Jianjun Jing and Liang Li; data collection and analysis: Liang Zheng, Haihong Li, and Hui Wang; drafting of the article: Liang Li and Longfang Zhang; critical revision of the article for important intellectual content: Yongxiang Wu; study supervision: Jianjun Jing. All the authors approved the final article.
Data Availability
All data that support the findings of this study are included in this article and its supplementary information files. The datasets used or analyzed during the current study are available from the corresponding author on a reasonable request.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Youth Development Project of Military Medical Science and Technology (MMST, No. 14QNP023). They all authored or reviewed drafts of the article.
Ethical Approval
This study was approved by the Ethics Committee of General Hospital of Xinjiang Military Region (Reference number to the ethical application: GHXJMR-EC099), and the written approval was waived.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.