
Abstract
Objective:
For early glottic carcinoma, the 2 main treatment modalities are radiotherapy (RT) and transoral CO2 laser microsurgery (TLM). The aim of this study was to investigate treatment preferences and considerations in patients with early glottic carcinoma (T1-T2) who were given a choice between TLM and RT.
Subjects and Methods:
Patients with early glottic cancer (suspected or confirmed extended T1 or limited T2) were counseled by an ENT-surgeon. A subset of 32 patients was also counseled by a radiotherapist. Treatment choice and considerations were recorded and analyzed.
Results:
Of 175 patients, 168 patients (96%) chose TLM, and 7 patients (4%) chose RT. The most common reason for choosing TLM was shorter treatment and more treatment options in case of recurrence. Subanalysis showed that additional counseling by the radiotherapist did not seem to affect our patients’ preferences for TLM in this group.
Conclusions:
The majority of patients in our study prefer TLM to RT when given a choice. Reasons given indicate that optimizing future treatment options and practical considerations seemed more important to our patients than primary functional outcome. Further research is needed to study patient-related and physician-related factors to gain more insight into this complicated process of shared decision making.
Introduction
The main treatment modalities in early glottic carcinoma (Tis-T2) are radiotherapy (RT) and transoral CO2 laser microsurgery (TLM). There is as of yet no formal proof that one treatment is more efficient than the other, and the respective use of these 2 modalities varies. 1 Recently published National Institute for Health and Care Excellence (NICE, United Kingdom) guidelines advise TLM for all T1a tumors, whereas TLM or RT is suggested for T1b to T2 lesions. This guideline aims to reduce variation in practice and improve survival. 2 According to the Dutch guideline for the treatment of laryngeal carcinoma, TLM is the treatment of choice for superficial T1a midcord lesions. For the more extended T1 and T2 lesions, radiotherapy is still the advocated treatment. 3 However, in other countries, more extended glottic tumors are treated with TLM.4-13
Both treatment modalities offer advantages and disadvantages. Advantages of TLM are shorter hospitalization, decreased morbidity, and lower cost. Also, using TLM as a primary treatment strategy leaves more treatment options open in patients with recurrent disease.14,15 Patients who have been primarily treated with radiotherapy cannot be re-irradiated, and achieving a radical laser resection is more difficult in an irradiated larynx. Therefore, these patients have a potentially higher risk of undergoing a laryngectomy, and several studies show larynxpreservation to be lower in patients initially treated with RT.16-18 A possible advantage of RT is that voice outcome, although similar for the 2 treatment modalities for limited T1 lesions, is thought to be better after RT in more extended T1 and T2 carcinomas, although definitive proof of this is lacking.
In light of the aforementioned, treatment strategy not only depends on the individual surgeon and patient preference but also varies between institutions and countries. Although much has been written about the relative merits of the 2 treatments, to our knowledge, there is no study available on how patients make clinical decisions with related considerations. The objective of this study was to investigate treatment preferences and considerations in patients with suspected or confirmed early glottic carcinoma (T1-T2) who were given the option between TLM and RT.
Patients and methods
The current study was carried out as a part of a larger multicenter study on functional outcome after treatment for early glottic carcinoma (extended T1 and limited T2) requiring a transmuscular resection (ELS type III) or a bilateral superficial resection of the anterior commissure (bilateral ELS type II). In the Netherlands, the guideline advocates radiotherapy for these lesions mainly because functional outcomes are believed to be better after RT. The multicenter study of which this study is a part was designed to investigate this assumption.
For this study, we prospectively enrolled patients in 2 tertiary university institutions in the Netherlands (Leiden University Medical Center [LUMC] and Erasmus MC Cancer Institute [EMC]) who were identified with untreated early glottic carcinoma or with a clinically suspected lesion possibly fitting the study criteria described previously. Prior to endoscopy under general anesthesia, all patients underwent stroboscopy and were offered the option of either TLM or radiotherapy should their lesion prove to require the stated resections during endoscopy (ELS bilateral type II or unilateral type III). Patients were counseled about the advantages and disadvantages of both treatment options by a head and neck surgeon/laryngologist (henceforth ENT-surgeon) who are the primary physicians regarding the treatment of this tumor in both participating hospital organizations. A random subset of the patients was counseled by both an ENT-surgeon and a radiotherapist in that order and only occurred when the radiotherapist was available in the outpatient ENT-clinic. After having had both modalities extensively explained to them in a face-to-face conversation of about 15 minutes by their treating physician(s), patients were also specifically informed that RT is the standard therapy according to the Dutch guideline for this type and extension of the tumor. Patients were given the same written information on both treatments (see the following), which was written by both an ENT-surgeon and a radiotherapist. Patients were given 1 week to make a choice between the 2 treatments. For the larger study, patients were given several elaborate questionnaires on paper, with 2 questions on the last page of the questionnaire: “Which treatment do you prefer? Can you specify why you chose this treatment? (you are allowed to describe more than one consideration).” From the patients’ own words, it was obvious what patients implied with their arguments. Subsequently, the arguments were arranged according to their content into categories that closely resembled the written text of the patients. There were no problems with categorizing these arguments. If more considerations were mentioned by 1 patient, this combination was kept as a whole and recorded as 1 reason (e.g., “more secondary treatment options and shorter treatment duration”).
This study was approved by the local medical ethics committees. Informed consent was obtained from each patient before participation.
Statistical Method
Data were analyzed using SPSS version 23.0 (IBM Corp, Armonk, New York, USA). The Fisher’s exact test of association was used to test the difference in treatment choice after counseling by only the ENT-surgeon or after counseling by both an ENT-surgeon and a radiotherapist.
Patient information
The following text is the literal translation of the part of the written study information, considering the advantages and disadvantages of both treatment modalities, given to the patients:
Benefits of laser surgery are that treatment takes place in one day instead of 5 weeks every working day for radiotherapy. You are admitted in the morning and in the evening of the same day you will go home in the majority of cases. Furthermore, you will have fewer complaints of sticky saliva and dry mouth than after irradiation. Finally, in the rare advent that cancer recurs, there are usually more secondary treatment options, which may result in a higher probability of preserving your larynx. Advantages of radiation therapy are that you do not undergo surgery and that you probably have a better voice outcome than after laser surgery. If you add higher value to voice outcome, radiotherapy would be a good choice. If you prefer a shorter hospital stay and a theoretically higher chance of larynxpreservation, laser surgery would be a good option.
Results
In total, 175 patients were identified as potentially fitting the study criteria and were offered a treatment choice (RT or TLM) between December 2009 and March 2015 in the 2 institutions. Table 1 shows the distribution of the definite T-stages after endoscopy. Of the 175 included patients, 37 were eventually staged as Tis, 69 as T1a, 27 as T1b, 39 as T2, and 3 as T3 (Table 1). Because patients were counseled before the staging endoscopy, not all patients met the final inclusion criteria (extended T1 and limited T2 tumor requiring a bilateral type II or unilateral type III resection) and were therefore not treated by their preferred treatment but according to Dutch guidelines. 3
Distribution of Tumor Stage After Endoscopy.
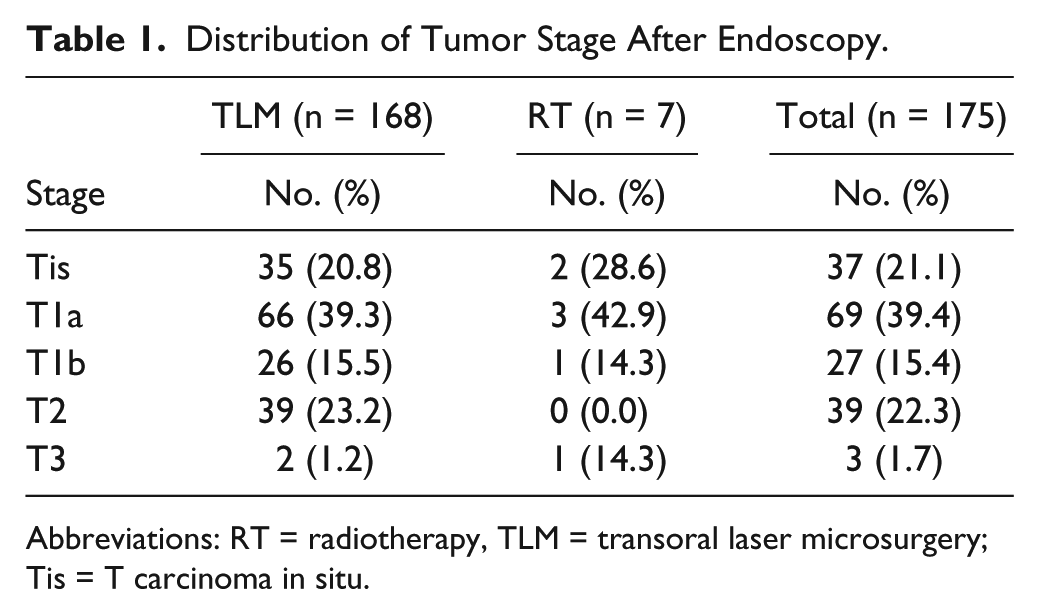
Abbreviations: RT = radiotherapy, TLM = transoral laser microsurgery; Tis = T carcinoma in situ.
All patients were asked to give their preference before the staging endoscopy; 168 patients (96.0%) chose TLM, and 7 patients (4.0%) chose RT. In total, 118 patients (67.4%) complied with our request and described their considerations relevant to their choice (Figure 1).
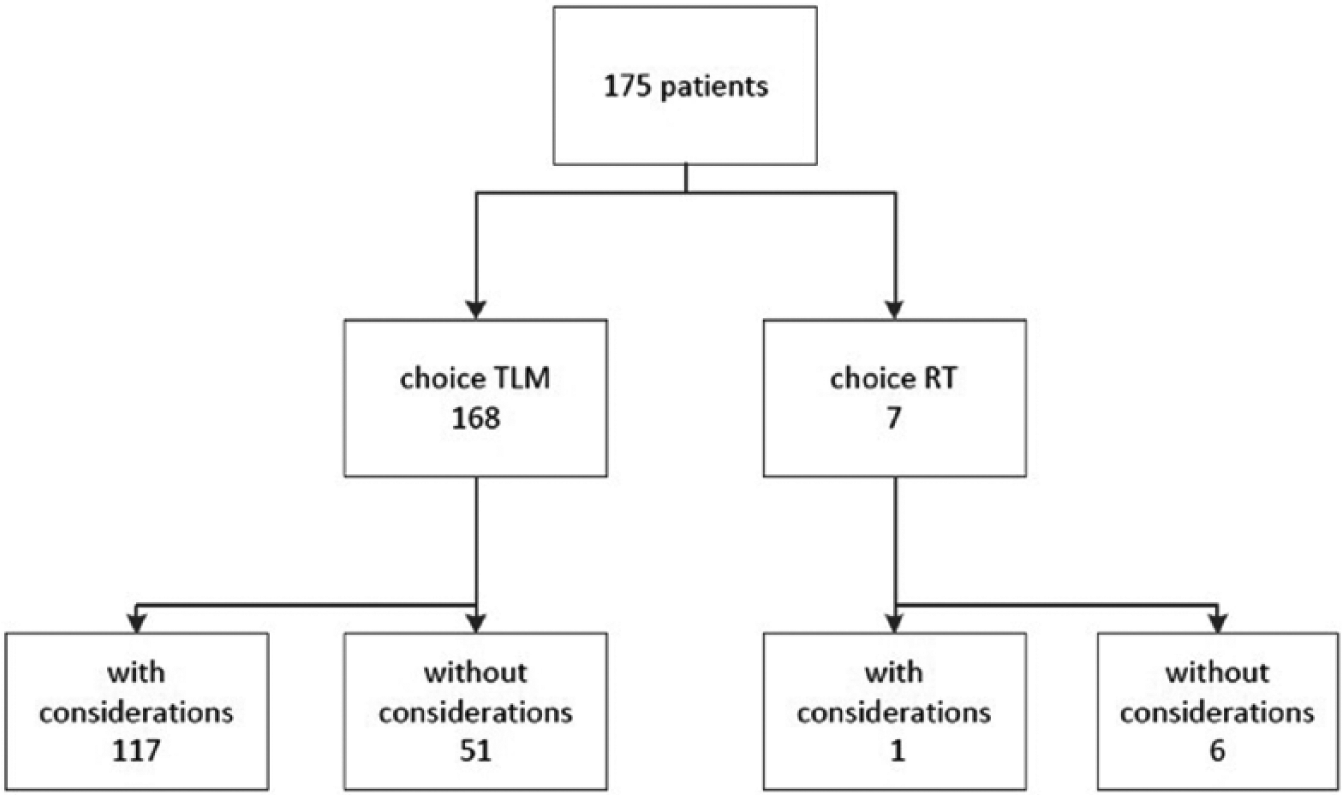
Flowdiagram of the study patients choosing their treatment of choice.
Table 2 shows the categorized argumentation of all patients. The most important reasons for choosing TLM were that TLM has a shorter treatment duration (21.4%), that more secondary treatment options were available in the case of recurrence (13.7%), and a combination of these 2 reasons (11.3%). Only 1 patient, who chose radiotherapy, gave written considerations. This patient chose radiotherapy because of the better voice outcome (14.3%). Arguments under the heading “other” were more confidence in TLM and fear of radiotherapy.
Considerations of the patients.
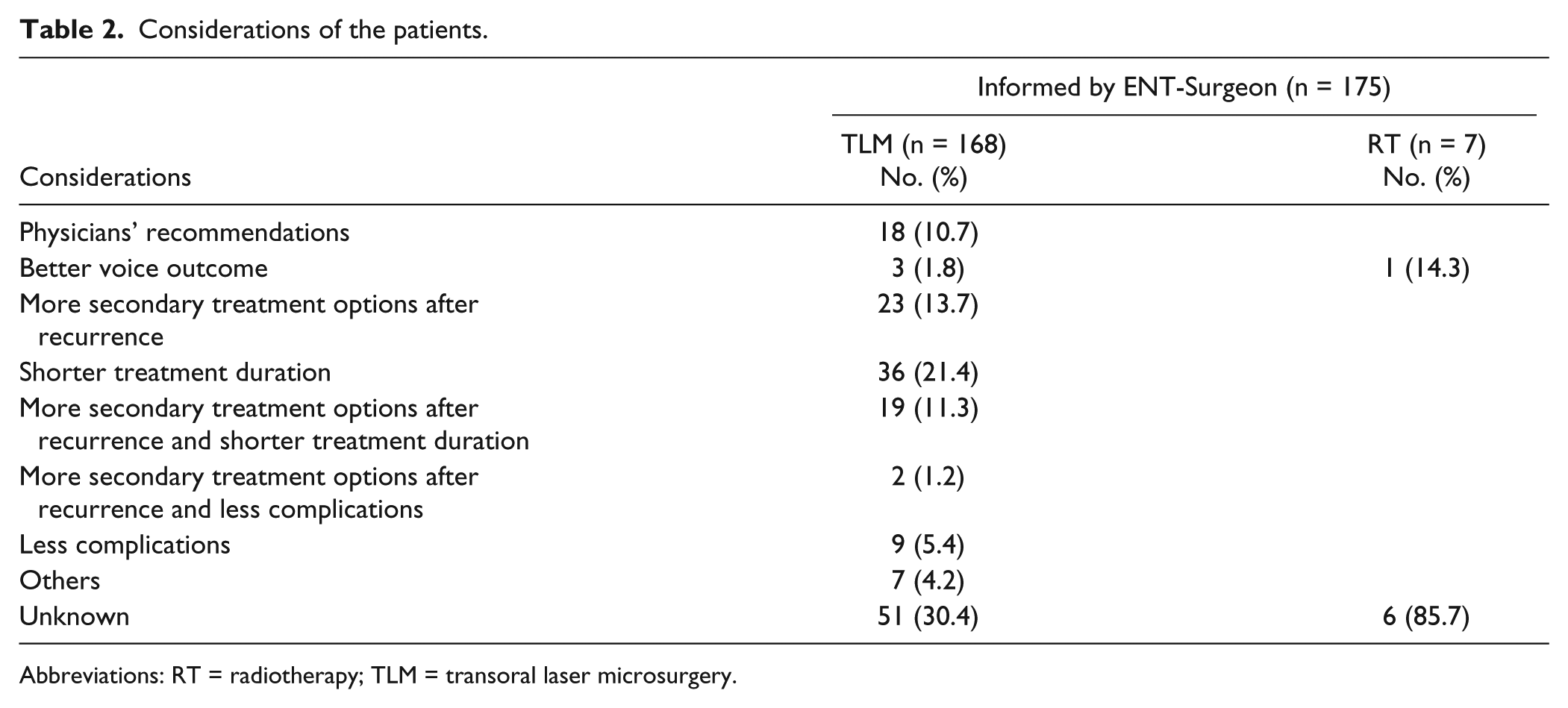
Abbreviations: RT = radiotherapy; TLM = transoral laser microsurgery.
A subanalysis of patients counseled by both an ENT-surgeon and a radiotherapist showed that all patients (n = 32) chose TLM (100%) (Figure 2). Patients counseled by only the ENT-surgeon showed that 95.1% (n = 143) chose TLM. No statistically significant differences in treatment choice exist between patients counseled by only the ENT-surgeon or by both an ENT-surgeon and a radiotherapist (P = .352).
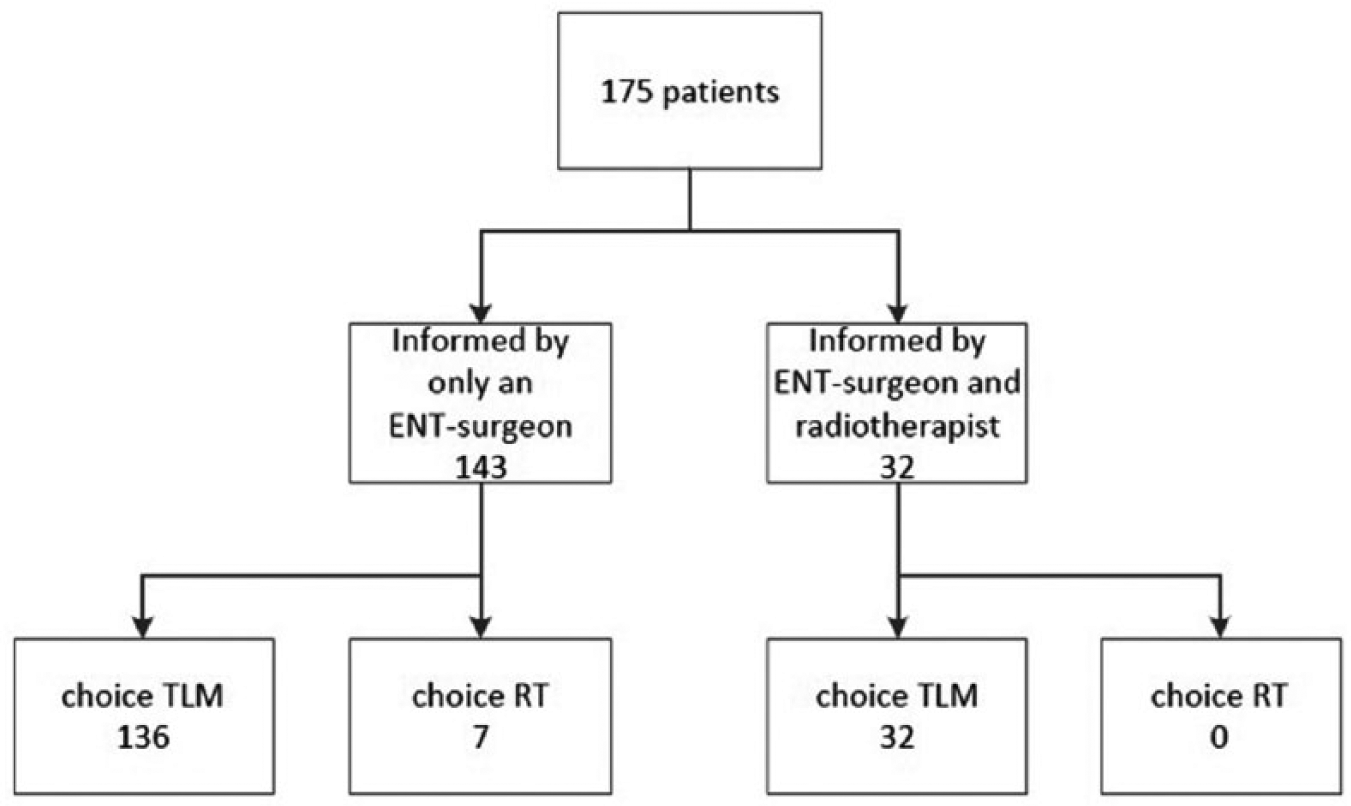
Flowdiagram of the study patients informed by only an ENT-surgeon or by both an ENT-surgeon and a radiotherapist.
Discussion
To our knowledge, this is the first study that describes treatment preferences in combination with a detailed evaluation of the considerations of patients with suspected or confirmed early glottic carcinoma (T1-T2) who were given the option between treatment with TLM or RT. In our study, 96.0% of the patients chose TLM, citing shorter treatment duration and more treatment options in case of recurrent disease as their main reasons, which was unexpected as the Dutch guidelines recommend RT for these lesions and patients were informed that their voice outcome would probably be better after RT. This indicates that optimizing future options and practical considerations were more important to our patients than primary functional outcome.
We found 3 similar studies in which patients with early glottic carcinoma were asked to choose their own treatment. In a study by McNeil et al, 19 all patients with Tis-T2 (n = 64, 100%) chose treatment with TLM. However, this study did not report on the considerations of the patients when choosing their treatment. 19 Zahoor et al 20 also reported on patients’ choice for early glottic carcinoma (T1-T2). They offered 99 patients a choice between TLM and RT, of which 59 patient (59.6%) chose TLM, and 35 patients (35.4%) chose RT. It is not clear from this study if patients with T2 tumors were more likely to choose RT. Also, this study did not report on the considerations of the patients when choosing their treatment. Contrary to our study, all their patient were counseled by a clinical oncologist and an ENT-surgeon. 20 Stoeckli et al 21 reported on patient preferences in early glottic (T1-T2) carcinoma treatment after multidisciplinary counseling, which contrary to our study, incorporated definite tumor stage in discussion with patients. In their study, the choice was fairly evenly distributed, with 65 patients choosing TLM and 75 patients choosing RT. The authors reported briefly on treatment preferences, but they were not studied in detail. There is no description of how the preferences were evaluated, how many patients preferred a specific therapy, and how many patients were treated according to their preference. They do report that patients with larger tumors and major concerns about their voice preferred RT, resulting in a predominance of T2 tumors and tumors with involvement of the anterior commissure in the radiotherapy group. Patients who opted TLM as primary treatment did this mainly because of shorter treatment duration. Also, they were less concerned about their voice. 21 Although the authors state that all effort was made to objectively counsel the patients, they acknowledge that it was possible that inadvertent bias was introduced in patients with larger tumors and tumors involving the anterior commissure, who primarily chose RT.
Literature shows that patients’ choice may vary according to what information they receive and by whom. To investigate a possible link between treatment choice and the discipline of the counseling physician in our study, a random subset of our study group (n = 32) was counseled by both an ENT-surgeon and a radiotherapist. In this subset, all patients chose TLM (100%). The minority of patients that chose RT (n = 7, 4%) were not counseled by a radiotherapist. Our results showed no statistically significant differences in treatment choice between patients counseled by only an ENT-surgeon or by both specialties. However, we cannot draw the conclusion that the specialty of counseling is not of influence on the final treatment decision. The reasons for this are further addressed in the limitations section of our study, described below. Contrary to this, a study by Makki et al 22 performed in Canada found that surgeons and radiotherapists diverged in treatment recommendations for early stage glottic cancer and that little consensus existed between them. For T1a tumors, radiotherapists preferred radiotherapy, and surgeons preferred TLM. For tumors staged T1b, the preferred treatment was radiotherapy among radiotherapists, but the preference of surgeons was split between radiotherapy and TLM. For T2 tumors, radiotherapy stood out as the treatment of choice for both specialties. 22 In our study, we did not examine physicians’ preferences as such, but as stated previously, additional counseling by the radiotherapist did not affect treatment choice. Notably, the size of the T2 tumors included was limited and may well have been smaller than in the studies by Stoeckli et al 21 and Makki et al 22 in which RT was found to have a more prominent role in larger lesions. From our results, one might speculate that both the ENT-surgeons as well as the radiotherapists in our participating hospitals might prefer TLM for limited lesions in early glottic cancer and that more consensus exists between the treating physicians in this study than in Makki et al’s 22 study. However, to determine this, a more in-depth study of physicians’ preferences in our hospitals would need to be performed.
In addition, our results showed that 18 patients (10.3%) made their choice between TLM and RT based directly on their physicians’ suggestion. This illustrates that not only patient preferences play a major part in clinical decision making but also the personal preferences of the specialist (ENT-surgeon or radiotherapist) counseling them. There are a number of studies investigating the role and features of physician counseling. Notably, a study by Gurmankin et al 23 evaluated the effect of physicians’ recommendations on hypothetical medical treatment decisions. Four hypothetical medical treatment scenarios were evaluated by 102 random subjects through a web-based questionnaire. It was made obvious to the subjects which treatment would lead to maximized health. However, subjects were significantly influenced by the physicians’ recommendations even when the recommendations went against the decision that maximized health. In another study, Scherr et al 24 assessed the influence of patient preferences and recommendations in treatment decisions for clinically localized prostate cancer. They concluded that patients’ treatment decisions were based largely on the physicians’ recommendation, which in turn were based on medical factors and not on patients’ personal views of the relative advantages and disadvantages of treatment alternatives. The study of Ubel et al 25 investigated treatment choice among physicians and concluded that when physicians make treatment recommendations for a patient, they think differently than when making decisions for themselves. Considering the aforementioned studies and our results, it is advisable that before giving their recommendations on treatment modalities, physicians examine and incorporate patients’ personal values and preferences. Also, physicians should be aware that recommendations can be influenced by their own personal attitudes toward a treatment whether counseling an individual patient or preparing a guideline recommendation and that these attitudes are not always consistent.
Our study has 4 main limitations. The first is that 57 patients (32.6%) did not write down their considerations when choosing their preferred treatment. Patients were asked to write down their preferred treatment and considerations at home, and answers were not checked immediately after receiving them in person or by mail in our clinic. However, regarding the consistent choice of TLM in most patients, we might expect that the considerations of patients without written argumentation would be similar to the ones we did receive. The second main limitation is that several doctors in the 2 different institutions informed the patients, which may have created bias. Although it is impossible to inform all patients in precisely the same way when several counseling physicians are involved, the written information regarding the study was exactly the same. The third main limitation is that patients were randomly counseled by the radiotherapist, which may have established inadvertent bias. In an ideal (study) setting, both specialties would be available for counseling in the same room. In our study, counseling by the radiotherapist was only performed when the radiotherapist was present in the outpatient clinics. In both participating hospitals, the ENT-surgeon is the primary physician and contact for patients with this type of tumor. It is not a standard procedure to have radiotherapist counseling as well at the first visit. After this visit, normally the multidisciplinary tumor board (ENT-surgeon, radiotherapist, radiologist, medical oncologist) decides on the best treatment option, taking into account a patient’s wishes whenever possible. If the treatment proposal is radiotherapy, then the patient is referred to the radiotherapist for further counseling. Although all effort was made to counsel patients in the same way, due to logistical reasons, this was not possible. Therefore, the ENT-surgeon also informed patients about radiotherapy in both groups. The chance that this bias in counseling influenced our results is imaginable since only a small subset of patients was counseled by both specialists (n = 32). Also, the order of counseling, first by an ENT-surgeon and afterward by a radiotherapist, could have influenced the outcome in this subgroup. The last main limitation is that there is the probability of ENT-surgeons having offered the patients to remove the tumor in the same session as the staging endoscopy. This is not recorded and might be an explanation for the overwhelming choice for TLM since patients have to undergo only 1 endoscopy directly combined with the tumor removal, instead of staging endoscopy combined with radiotherapy afterward. A minor limitation is that we did not perform a patient baseline characteristics comparison between the 2 groups since the size of the groups was so different. This limits analysis of potential factors influencing the treatment decision. We did not investigate and compare other patient characteristics between the 2 groups. It could be that differences in demographic factors, socioeconomic status, cultural background, personal factors such as risk adversity or social network, and patient-physician relation might have been of influence on the patient’s choice for a treatment. The patients studied are patients with early glottic carcinoma, fitting the study criteria drawn from consecutive patients with early glottic carcinoma presenting in academic centers in the Western part of the Netherlands. We believe that it is likely that in general they will have a similar mix of concerns and priorities guiding them in their treatment choices as patients in countries with similar variety in race and socioeconomic status. Whether our population is representative for the global population of glottic cancer patients is more challenging to tell, especially as the many different variations in global health care systems may greatly influence the final choice of the global patient cohort.
In conclusion, patients with early glottic carcinoma have to consider several factors when choosing a treatment modality. In this multicenter study, the majority of patients prefer TLM despite the Dutch national guideline advocating RT and despite the fact that it was explained to them in counseling and in writing that their voice would probably be better after RT. The main reasons for preferring TLM were shorter treatment duration and more treatment options in case of recurrence. Additional counseling of a small subgroup by the radiotherapist did not seem to affect our patients’ preferences. However, this subgroup was relatively small, and the outcome may have been influenced by the physician’s preference, the order of counseling of the physicians, or patient-related factors. We think it is important for physicians to be aware that their own attitude toward a treatment modality and recommendations can influence a patient’s treatment choice. More research is needed regarding the counseling and preferences of both physicians and patients to gain insight into the complex process of shared decision making. Further studies would need a larger number of patients, random order of counseling of all patients by both an ENT-surgeon and a radiotherapist, more information on patient-related factors, and insight into physicians’ preferences to substantiate our initial findings in this study that patients with extended T1 and limited T2 tumors prefer TLM to RT. Suitable decision-making tools for early glottic carcinoma should be developed for clinical practice.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This project was awarded a grant by ZOLEON, Stichting Oncologie Haaglanden West, Leiden, The Netherlands.