
Abstract
Coronary computed tomographic angiography (CCTA) is a promising technique for ruling out coronary artery disease (CAD) in patients with chest pain. We aimed to investigate the prognostic impact of nonobstructive CAD on CCTA. We retrospectively reviewed patients who underwent CCTA between 2010 and 2016 at our institution. We divided them into 3 groups: (1) patients with no CAD, (2) patients with nonobstructive CAD, and (3) patients with obstructive CAD. We investigated the incidence of the primary outcome (combination of death, nonfatal myocardial infarction, unstable angina, and late revascularization). A total of 989 patients were included: 540 patients had CAD, which was obstructive (≥50% stenosis) in 256 cases. During the follow-up period, 99 events occurred (32 [7%] in patients without CAD, 26 [9%] in patients with nonobstructive CAD, and 41 [16%] in patients with obstructive CAD; P < .001). The presence of nonobstructive and obstructive CAD was an independent predictor of events (HR: 2.33 [1.15-4.69], P < .001; and 4.02 [1.98-8.13], P = .019, respectively) compared with no CAD. Nonobstructive CAD on CCTA is associated with a 2-fold increase in risk of coronary events compared with patients with no CAD.
Introduction
Coronary computed tomographic angiography (CCTA) is increasingly used for noninvasive imaging of coronary arteries. 1 In patients with clinical symptoms suggestive of coronary artery disease (CAD), CCTA is an important tool for appraisal of coronary anatomy, with studies suggesting excellent sensitivity and fair specificity for the detection of obstructive CAD when compared with invasive coronary angiography.2–5 Moreover, appraisal of patients with chest pain with CCTA as the initial diagnostic test provides a promising tool for further clinical management in terms of prevention of unfavorable clinical outcomes, such as acute coronary syndromes or coronary death.6,7
Besides its gatekeeping function in noninvasive detection of obstructive CAD, CCTA also provides information on nonobstructive atherosclerosis.8,9 Nonobstructive lesions may not be associated with anginal symptoms, and therefore do not represent a potential target for revascularization, but nonetheless represent an important underlying pathology that may cause subsequent progression of atherosclerosis, acute myocardial infarction, or cardiac death.6,10,11
We therefore evaluated the prognosis (mortality and cardiovascular events) of patients with nonobstructive CAD on CCTA.
Methods
Study Design and Population
Consecutive patients referred for CCTA between January 1, 2010, and April 30, 2016, at the Clinic for Nuclear Medicine, University Medical Centre of Ljubljana, were screened for inclusion. Inclusion criteria were 18 years of age or older, clinical indication for CAD evaluation because of anginal symptoms, clinical and risk factors information available at the time of scan.
Patients with known CAD, without stenosis appraisal (eg, due to high calcium score), with nondiagnostic CCTA because of artefacts (CAD RADS N) in 2 or more coronary segments, or with missing data were excluded.
Primary outcome was defined as a combination of death, nonfatal myocardial infarction, unstable angina, late revascularization (≥90 days after scan and not triggered by suspected obstructive stenosis on CCTA).
A researcher blinded to the CCTA results conducted follow-up for mortality (through national vital status database) and for nonfatal events (direct/telephone follow up with patients/next of keen/general practitioner, or review of medical records).
The study was approved by the National Medical Ethics Committee, Republic of Slovenia (approval number 62/06/14).
Coronary Computed Tomographic Angiography Scanning Protocol and Analysis
Coronary computed tomographic angiography scanning was performed using a 128-row multiple detector computed tomography scanner (Siemens Biograph mCT, Siemens Medical Solutions Inc). For patients who were ≥50 years of age, calcium scoring was performed upfront, and if it was reasonably low (Agatston score <300), angiographic protocol was continued.
We used an electrocardiogram (ECG) gated, prospective scanning protocol with intravenous (IV) administration of contrast (Iomeron 400, Bracco diagnostic Inc), when feasible. The final volume of contrast (average 75 mL) depended on the duration of the procedure. Patients were premedicated with 0.4 µg of sublingual glyceryl trinitrate (if not contraindicated) and metoprolol (25-100 mg orally or 5-15 mg IV if the heart rate exceeded 65 beats/min), at the discretion of physician performing the CCTA.
Data sets were reconstructed and all CCTA images were transferred to 3-dimensional image analysis workstation (Syngo.via, Siemens Healthcare GmbH 2009-2020, Siemens Medical Solutions Inc). Images were acquired either using prospective ECG triggering at 75% of RR interval (i.e., the interval between two consecutive R spikes in the ECG) or by retrospective ECG gating with images constructed at 5% intervals from 5% to 95% of RR interval. Images were analyzed as per institutional protocol by either a qualified radiologist or a qualified cardiologist (level III Society of Cardiovascular Computed Tomography certification), with radiology–cardiology consultancy immediately available on site in case of specific clinical/imaging issues or diagnostic uncertainty.
Coronary atherosclerosis was defined as any visualized lesion within, or adjacent to, the arterial lumen that could be differentiated from surrounding anatomical structures. Coronary artery disease was graded as no CAD (no atherosclerosis), nonobstructive CAD (1%-49% stenosis) or obstructive (≥50% stenosis) as appreciated through available intensity projection and multiplanar reconstruction methods.
Statistical Analysis
Baseline characteristics are expressed as mean (± standard deviation) for normally distributed continuous variables, as median (interquartile range) for non-normally distributed continuous variables, and as frequency (%) for categorical variables. Between-group differences were assessed by t test for normally distributed variables, by the Mann-Whitney U test for non-normally distributed variables, and proportions were compared using the χ2 test. Kaplan-Meier curves and log-rank test were used to evaluate event-free survival. Cox proportional hazard models were constructed to assess prognostic significance of absent, obstructive and nonobstructive CAD, and were expressed as hazard ratio (HR) with corresponding 95% CIs. A 2-tailed P < .05 was considered significant. Statistical analysis was carried out using SPSS Statistics version 23 (SPSS Inc).
Results
Study Population
Of the 1031 patients reviewed, 42 (4.1%) patients were excluded because of high calcium scores preventing adequate interpretation of angiographic findings. A total of 989 patients (mean age 61 years; 54% women) were included in the final analysis, with almost 55% of them having CCTA signs of obstructive or nonobstructive CAD (Table 1).
Baseline Characteristics of the Overall Population and Separately of Patients With No, Nonobstructive (1-50% Stenosis) and Obstructive (>50% Stenosis) Coronary Artery Disease (CAD).a
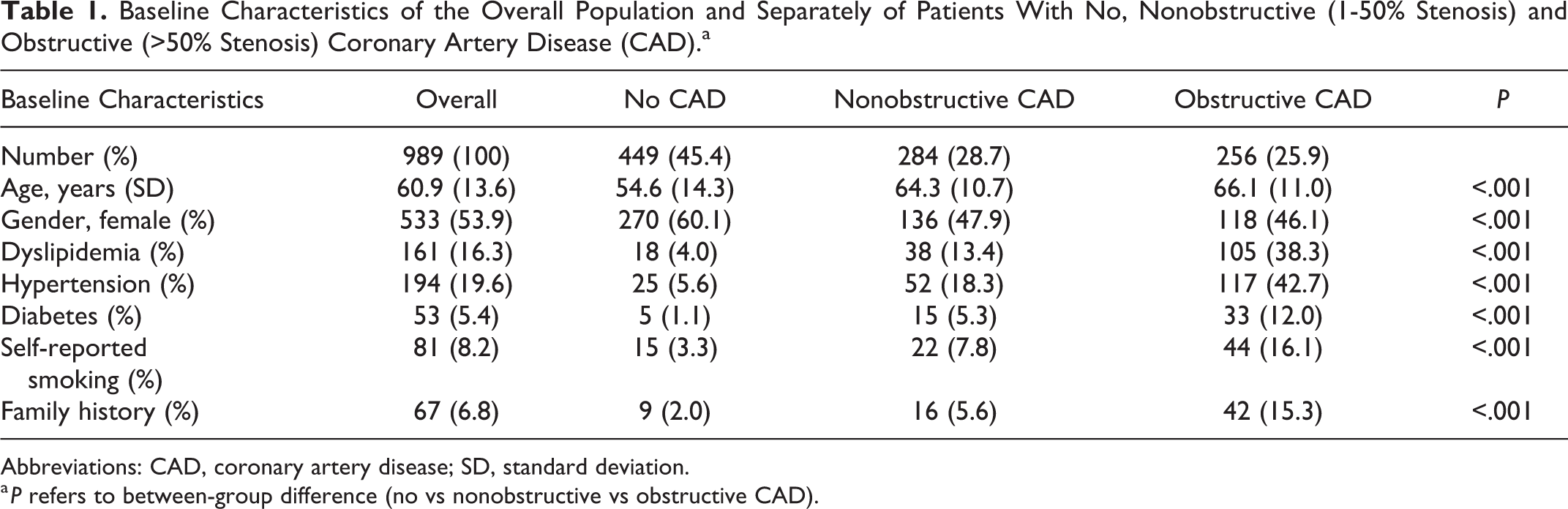
Abbreviations: CAD, coronary artery disease; SD, standard deviation.
a P refers to between-group difference (no vs nonobstructive vs obstructive CAD).
Baseline Characteristics
Patients with either obstructive or nonobstructive CAD were on average older and more often female. Traditional risk factors were more common in patients with obstructive CAD, participants in this group were older and more likely to be men (Table 1).
Referral Diagnosis
We were able to retrieve the referral diagnosis for 617 patients: 392 (63.6%) were referred due to chest pain; 13 (2.1%) due to shortness of breath on exertion; 153 (24.8%) to assess the presence of CAD based on other clinical factors, such as heart failure; and 59 (9.6%) to assess obstructive CAD based on previous inconclusive noninvasive tests, such as ECG exercise testing.
We were able to determine pretest probability of obstructive CAD (PTP) according to the last recommendations included in 2019 European Society of Cardiology guidelines 12 for the diagnosis and treatment of chronic coronary syndromes for 333 patients: 20 (4.9%) had a PTP <5%, 105 (25.9%) had a PTP 5% to 15%, and 280 (51.4%) had a PTP >15%.
End Points
During the mean follow-up period of 1606 days (interquartile range: 953), 7%, 9%, and 16% events occurred in patients without, with nonobstructive and with obstructive CAD, respectively (translating to 1.54%, 1.82%, and 4.07% annualized event rates, respectively).
Event rates exhibited a gradient from no CAD (2.3%) to nonobstructive single-vessel disease (5.2%), nonobstructive ≥2 vessel disease (6.5%), obstructive single-vessel disease (7.5%), and obstructive ≥2 vessel disease (9.7%), respectively, with annualized event rates ranging from 0.51% in no CAD, 1.16% in nonobstructive CAD and 2.01% in obstructive CAD, respectively. In the Cox regression analysis (χ2 461.18, P < .001) traditional risk factors emerged as predictors of events: hypertension (HR: 3.53 [2.40-5.35], P < .001), dyslipidemia (HR: 1.96 [1.34-2.90], P = .001), family history (HR: 1.92 [1.37-2.68], P < .001), and smoking (HR 1.82 [1.30-2.54], P < .001), presence of nonobstructive and obstructive CAD was an independent predictor of events (HR: 2.33 [1.15-4.69], P < .001, and 4.02 [1.98-8.13], P = .019, respectively) compared with no evidence of atherosclerosis (Figure 1).
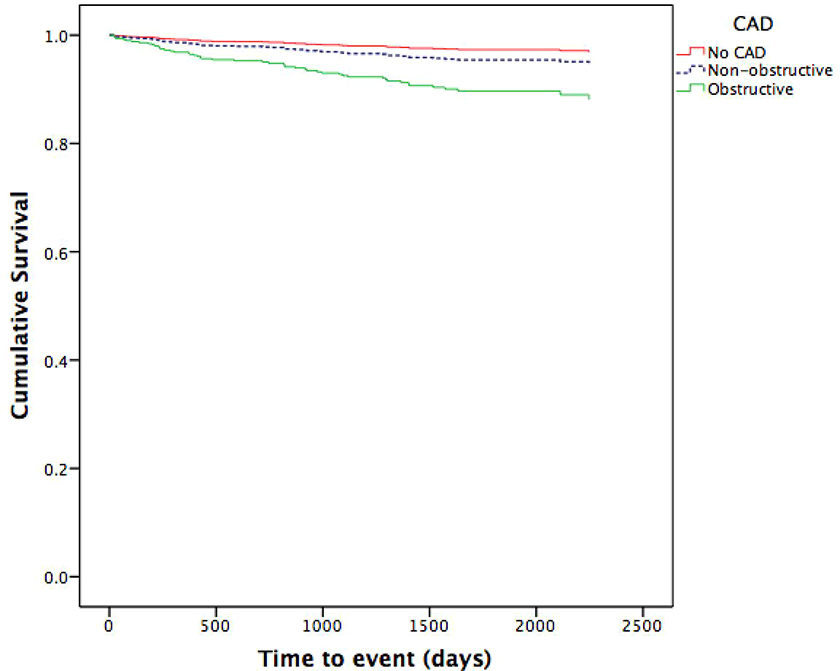
Kaplan-Meier curves for no evidence of coronary artery disease (CAD), nonobstructive CAD, and obstructive CAD.
Discussion
Our study confirms that CAD as detected by CCTA—irrespective of lesion severity, and number of affected coronary segments or arteries—carries an unfavorable cardiovascular prognosis. Patients with nonobstructive and obstructive CAD had a roughly 2- and 3-fold increase, respectively, in the rate of major cardiovascular events compared with individuals without evidence of atherosclerotic disease on CCTA. This is in line with previous observational studies.7,13,14
In terms of pathophysiologic understanding, nonobstructive atherosclerosis lesions are associated with risk of plaque rupture and subsequent atherothrombotic event. Although the risk of atherothrombotic events increases with increasing plaque burden in obstructive lesions, the risk is still present in nonobstructive lesions. This is particularly true for lipid-rich noncalcific plaques, which are less stable and more prone to fibrotic cap rupture and subsequent atherothrombosis.10,15 Nonobstructive CAD therefore still retains a strong predictive power that should not be neglected by clinicians.13,15
In terms of previous observational studies, data from the multicenter Coronary CT Angiography Evaluation for Clinical Outcomes: An International Multicenter registry suggests that obstructive CAD on CCTA carries an incremental prognostic value beyond that of clinical risk factors. 9 Nonobstructive CAD was also found to have an increase in mortality risk rate and a higher risk of major adverse cardiovascular events in both stable and acute chest pain.11,15 Patients with nonobstructive CAD have a worse mid- and long-term prognosis than those with completely normal arteries. 15 It has been also shown that the extent of CAD is an important prognostic factor, with proximal stenosis and presence of mixed or calcified plaques in proximal segments being the 2 CCTA parameters that improve outcome prediction.7,9,13,14 Furthermore, with the development of technology, we are now able to identify plaques with low attenuation and positive remodeling which seem to be independent predictors for future coronary events.16,17
Our findings are in line with previous reports on the prognostic impact of nonobstructive CAD.18–20 Nonobstructive coronary atherosclerosis, as evaluated by either invasive angiography or CCTA, has previously been associated with roughly a 2- to 3-fold increased all-cause mortality, nonfatal myocardial infarctions, and revascularizations, corresponding well with our HR of 2.3.18,19 Conversely, a meta-analysis limited to studies of patients with typical angina symptoms and only appraising all-cause death or nonfatal infarction (but not revascularization), yielded less homogeneous results, suggesting that patient selection (urgent vs elective symptomatic vs elective asymptomatic) is pivotal for inference of nonobstructive lesion–associated risk. Our study population represents a real-life setting of patients referred for suspected CAD, with two-thirds exhibiting angina symptoms. Thus, it contributes to the growing body of evidence that nonobstructive coronary atherosclerosis as detected in real-life CCTA settings represents a high-risk condition warranting aggressive preventive management and follow-up.
This study is not without limitations. It was a retrospective single-center study, which carries potential selection bias; however, we tried to minimize this by taking into account all consequent patients who were referred to our institution. We were unable to obtain the cause of death for the majority of the studied population due to inaccessible data; nonetheless, it is safe to assume that the high rate of fatal events in the nonobstructive and obstructive groups were mainly driven by cardiovascular mortality, given the very high risk for CVD-related death in this population. Each CT scan was evaluated by a single physician; that could have introduced some error in the subjective stenosis evaluation.
Given the high number of included consecutive patients, the fair geographical variability provided by a national referral center and based on the baseline characteristics and the determined PTP, we can assert with a fair amount of confidence that our sample size is fairly representative of the population. Therefore, our results are generalizable to a population of patients with low to intermediate likelihood of CAD, where CCTA is known to perform best.
Our study supports that patients referred for CCTA in this region have mainly moderate pretest likelihood of CAD. That is in line with guideline recommendations 12 since this group of patients would benefit the most from this diagnostic procedure. Participants with obstructive CAD were then further evaluated with other diagnostic procedures or referred for angiography, which is again in line with the recommendations. 12
It has been shown that patients with nonobstructive CAD are more likely to be undertreated, despite having a higher mortality than patients with no signs of CAD on CCTA.18,21 Addressing the impact of CAD diagnosed by CCTA on therapeutic changes and inspecting whether it triggers a more aggressive prevention treatment would be of clinical value. Unfortunately, we were unable to obtain sufficient data about medical therapy to perform this analysis; further studies are needed to address this issue.
In conclusion, nonobstructive CAD on CCTA is associated with a 2-fold increase in the risk of coronary events compared with patients without signs of CAD. Therefore, those patients merit aggressive management in terms of CAD prevention.
Footnotes
Authors’ Note
All authors contributed to (1) substantial contributions to conception and design, or acquisition of data, or analysis and interpretation of data, (2) drafting the article or revising it critically for important intellectual content, and (3) final approval of the version to be published.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.